



Introduction
Around the globe, intergenerational co-residence, where an older person lives with at least one adult child, has historically been a critical source of support for ageing parents. In the United States of America, for example, health circumstances or other forms of vulnerability often drive co-residence decisions, as elderly people who are widowed, disabled or both have been found to be particularly likely to live with an adult child (Crimmins and Ingegneri, Reference Crimmins and Ingegneri1990; Stinner et al., Reference Stinner, Byun and Paita1990; Coward and Cutler, Reference Coward and Cutler1991; Silverstein, Reference Silverstein1995; Lee and Dwyer, Reference Lee and Dwyer1996). Similar results have been reported in a multi-country study in Europe, where activity limitations among older partnerless individuals increase the odds of co-residence, especially in contexts of economic insecurity (Isengard and Szydlik, Reference Isengard and Szydlik2012). In Japan, intergenerational co-residence is widespread, even without disability or other health concerns, although it often occurs with an eye to the future. Drawing on research by Hashimoto (Reference Hashimoto1996) and Ogawa and Retherford (Reference Ogawa and Retherford1997), Brown et al. argue that Japanese expect to be vulnerable in old age, and they plan early in life to maximize the certainty of receiving support from adult children by living with them. The coresidence of a married child and the parents often [begins] … at the marriage of the adult child. (Brown et al., Reference Brown, Liang, Krause, Akiyama, Sugisawa and Fukaya2002: S217)
Where state welfare provisions for seniors are limited, as is true in many developing countries, intergenerational co-residence is also a crucial source of care for elderly people (Johar and Maruyama, Reference Johar and Maruyama2014). Our research focuses on China, where co-residence has long been the primary source of old-age support. While children who live independently can and do provide care to ageing parents in China, co-resident children are uniquely positioned to meet parents’ material and health-care needs comprehensively. Furthermore, because of the centrality of filial piety and related Confucian teachings in Chinese society (Ikels, Reference Ikels, Davis and Harrell1993; Sung, Reference Sung1998), shared living arrangements also allow children to provide their parents with a sense of purpose by fulfilling a cultural obligation (Silverstein et al., Reference Silverstein, Cong and Li2006). Indeed, various studies find that even after accounting for intergenerational transfers and/or proximity to non-coresident children, ageing parents in China who live with adult children are more likely to report better physical health (Li et al., Reference Li, Liang, Toler and Gu2005; Williams et al., Reference Williams, Zhang and Packard2017), subjective wellbeing (Chen and Silverstein, Reference Chen and Silverstein2000; Chen and Short, Reference Chen and Short2008; Qian and Knoester, Reference Qian and Knoester2015) and psychological wellbeing (Silverstein et al., Reference Silverstein, Cong and Li2006) than those who do not live with adult children.
In recent decades, however, fundamental demographic, socio-economic and cultural shifts have been threatening to dismantle this traditional system of support. Since 1990, rates of intergenerational co-residence in China have been declining, due in part to years of low fertility and increasing life expectancy, which have reduced the number of children available to live with a growing population of elderly parents. The decline in intergenerational co-residence is also partially attributable to increasing migration of young individuals from rural to urban areas and concomitant shifts in youths’ opportunities, aspirations and attitudes regarding traditional forms of filial care (Chan, Reference Chan and Ness2013; Ren and Treiman, Reference Ren and Treiman2015). Some scholars like Chu et al. (Reference Chu, Xie and Yu2011) contend that the Confucian underpinnings of the mainland Chinese family have been considerably weakened in the aftermath of the Cultural Revolution and the Communist Revolution. Others suggest that children now limit co-residence to times when parents are most vulnerable and in need of care, often the period just before death (Zimmer, Reference Zimmer2005; Zimmer and Korinek, Reference Zimmer and Korinek2010; Zhang et al., Reference Zhang, Gu and Luo2014; Cong and Silverstein, Reference Cong and Silverstein2015). In so doing, they effectively ‘modify, but do not violate, the tradition of filial piety’ (Takagi et al., Reference Takagi, Silverstein and Crimmins2007: S330).
In this article, we contribute to the existing literature on co-residence in China in two key ways. First, while most of the studies cited above draw on survey data from more than a decade ago, we analyse recent panel data from the 2012, 2014 and 2016 waves of the China Family Panel Studies (CFPS) to examine whether, and if so, under what circumstances, adult children are continuing to live with parents. Specifically, we aim to investigate whether the co-residential patterns that were prevalent in the past continue to be evidenced, particularly at times of parental need associated with ill health or other vulnerabilities. Second, the unit of analysis for our study is older couples instead of older individuals. We argue that when both older parents are alive and in union, children will make co-residence decisions based on the health concerns and other vulnerabilities of both parents. Existing evidence suggests that spousal support is the primary form of care older individuals in China rely on in the absence of a co-resident child (Zeng and Wang, Reference Zeng and Wang2003); a decline in the availability of potential help from a spouse or the increasing need to provide care for a spouse who is in failing health is likely to translate into the need for adult children to compensate. Thus, in contrast to studies that model lack of spousal support in terms of spouse's vital status alone, this study looks to assess both spouse's vital status and her or his health status. More specifically, this study focuses on intact unions at baseline and uses a longitudinal approach to examine whether children respond via co-residence to the physical, cognitive or emotional health needs of one or both parents at baseline, or to other forms of vulnerability, such as an increase in activity limitations or the dissolution of parents’ marriage between baseline and follow-up.
We frame our analysis using intergenerational solidarity theory and assess the relevance of each component: (a) parental needs, (b) opportunity structures, (c) family structural considerations, and (d) contextual-structural considerations for co-residence patterns today. We focus most closely on parental needs that derive from poor health or loss of spousal support, but also consider other needs-based reasons for co-residence, such as being older or in a lower socio-economic bracket. Conversely, having adequate/desirable housing and other resources to share would provide one form of opportunity for co-residence. Having one or more children with whom one might live would be one family structural consideration; although, in the Chinese context, co-residence decisions may also depend on whether those children are of the preferred gender (Teerawichitchainan et al., Reference Teerawichitchainan, Pothisiri and Long2015). Cultural-contextual considerations refer to societal conditions within which intergenerational relations develop. These include conditions of the social, economic and tax system, the welfare state, the labour and housing market, as well as rules and norms of institutions and groups. (Isengard and Szydlik, Reference Isengard and Szydlik2012: 453)
Literature review
The context of China
While it is clearly important to understand the role of family support for the wellbeing of elderly people in a variety of contexts around the world, there are especially critical reasons for examining whether traditional support systems continue to operate effectively in contemporary China. Approximately 20 per cent of elderly people globally reside in China (Giles and Mu, Reference Giles and Mu2007), and the country's old-age dependency ratio is projected to increase sharply in the coming years (Giles et al., Reference Giles, Wang and Zhao2010), particularly in rural areas (Zhuo and Liang, Reference Zhuo, Liang, Iredale and Guo2015). Socio-economic forces that first translated into the decline in intergenerational co-residence continue to be in play today and their impact is likely to be amplified by the country's changing age structure (Chen and Liu, Reference Chen, Liu and Uhlenberg2009). While many in recent generations of elderly people have had a number of adult children to rely on, ‘it will not be long before one-and-two child parents reach the age when they will need care’ (Thøgersen and Anru, Reference Thøgersen and Anru2008: 13).
In addition, older parents in China have traditionally preferred co-residing with a married son, a desire that derives from China's patrilineal kinship system and underlying Confucian values, but a desire that will be increasingly difficult to fulfil as smaller birth cohorts reach care-giving age. Research on co-residence patterns according to the gender of the child has generally confirmed the implementation of this preference; co-residence with adult daughters has been comparatively infrequent (Logan et al., Reference Logan, Bian and Bian1998; Logan and Bian, Reference Logan and Bian1999; Xie and Zhu, Reference Xie and Zhu2009; Chu et al., Reference Chu, Xie and Yu2011).
There is evidence that the preference to live with sons may be abating, however, particularly among those living in cities, those with more education and those in higher-status occupations (Logan et al., Reference Logan, Bian and Bian1998; Logan and Bian, Reference Logan and Bian1999; Whyte and Xu, Reference Whyte, Xu and Whyte2003; Pimentel and Liu, Reference Pimentel and Liu2004; Xie and Zhu, Reference Xie and Zhu2009). Moreover, adult daughters do provide aid to elderly parents in China (Whyte and Xu, Reference Whyte, Xu and Whyte2003; Xie and Zhu, Reference Xie and Zhu2009). In times of need, they may offer various forms of care themselves, occasionally even co-residing at least temporarily, as is increasingly being witnessed in urban areas (Xu, Reference Xu2013). Silverstein et al. (Reference Silverstein, Cong and Li2006) have argued that daughters may be particularly responsive to their parents’ investment in their lives, reciprocating in one form or another because their relationships are regulated less by cultural obligations (filial piety) and more by rules of reciprocity than is true for sons. Daughters may also help parents achieve their desired living arrangement by pressuring their brothers to fulfil their filial obligations (Zhang and Wang, Reference Zhang and Wang2010).
The Chinese government has yet to step in as a significant source of assistance for elderly people, either in response to or in anticipation of demographic and social changes. While there have been some governmental measures to support the growing elderly population in recent years – e.g. rural residents and non-employed urban residents can now receive social pensions (Liu and Sun, Reference Liu and Sun2016) and older individuals who are partially or fully disabled receive long-term care insurance from state-sponsored pilot programmes in select areas (World Bank, 2016) – most of these programmes are not fully developed or widely accessible and the level of assistance under the different insurance schemes is woefully limited (Liu and Sun, Reference Liu and Sun2016). Further, private-sector programmes (e.g. high-end residential homes for the aged in urban centres) are restricted to the more affluent segments of the population (Feng et al., Reference Feng, Zhan, Feng, Liu, Sun and Mor2011, Reference Feng, Liu, Guan and Mor2012).
Older individuals and their families who live in remote rural villages are particularly at risk given these gaps in social protection. The lack of an adequate social safety net not only makes rural elderly people financially insecure, but it also increases the care-taking burden of adult children. In addition to the strain placed on family-centred support systems by demographic forces and labour market prospects favouring urban dwellers, rural adult children often have to delay or forego out-migration if they have an ill parent (Giles and Mu, Reference Giles and Mu2007). If social safety nets were stronger, potential migrants in rural areas would be freer to pursue earning opportunities elsewhere to meet their families’ financial needs more effectively.
Instead, the Chinese state has repeatedly reinforced the importance of family support systems for the elderly. Both the 1950 Marriage Law and the 1954 Constitution state that it is the child's duty to care for ageing parents (Giles and Mu, Reference Giles and Mu2007). The 1996 Law on the Protection of the Rights and Interests of the ElderlyFootnote 1 reaffirms this filial obligation (see Article 11) and gives older parents the right to seek legal action against remiss family members (see Articles 43 and 45). The right to pursue legal remedy from children is also specified in the 2001 Marriage LawFootnote 2: ‘If children fail to perform their duty, parents who are unable to work or have difficulty in providing for themselves shall have the right to demand support payments from their children’ (Article 21). The 2013 law entitled ‘Protection of the Rights and Interests of Elderly People’ further emphasises the obligation of children ‘to tend to the “spiritual needs of the elderly”’, stating that they should visit parents ‘often’, that they should send occasional greetings to parents, and that ‘[companies] and work units should give employees enough time off so they can make parental visits’ (Wong, Reference Wong2013: 1). Although children of elderly people report feeling pressured by competing obligations (Wong, Reference Wong2013), attitudinal data suggest that the expectation of child support continues to exist among older individuals, particularly when they are going through a health crisis (Laidlaw et al., Reference Laidlaw, Wang, Coelho and Power2010; Wang et al., Reference Wang, Laidlaw, Power and Shen2010). The extent to which this tension is resolved in the form of intergenerational co-residence is the focus of our research.
Theoretical framework
Collectively, the interactions between older parents and adult children reflect various forms of intergenerational solidarity (Bengtson, Reference Bengtson2001; Voorpostel and Blieszner, Reference Voorpostel and Blieszner2008; Bordone, Reference Bordone and Wright2015; Pezzin et al., Reference Pezzin, Pollak and Schone2015). Older parents and adult children can express solidarity by participating in activities together and maintaining frequent contact (associational solidarity), by fostering emotional closeness, respect and support (affectual solidarity), by reinforcing family-specific values and beliefs (consensual solidarity), by meeting familial obligations and roles (normative solidarity), and by sharing resources such as time, money and housing (functional solidarity) (Bengtson and Roberts, Reference Bengtson and Roberts1991; Isengard and Szydlik, Reference Isengard and Szydlik2012).Footnote 3 In this study, we focus on a specific expression of intergenerational solidarity: co-residence. While older parents and adult children who do not live in the same household can and do care for each other in a variety of ways, including by making monetary or in-kind transfers, and although co-residence might create or exacerbate certain tensions (e.g. related to loss of privacy or social control) (Umberson et al., Reference Umberson, Crosnoe and Reczek2010), the sharing of living space can enhance intergenerational solidarity across each of the dimensions outlined above.
We seek to understand the drivers of intergenerational co-residence as a form of intergenerational solidarity in contemporary China by drawing on recent scholarship that engages that framework and foregrounds the role of micro-level needs and opportunity structures, meso-level family structures and macro-level contextual structures (Szydlik, Reference Szydlik2008; Isengard and Szydlik, Reference Isengard and Szydlik2012). We provide examples of each component of the framework in the Introduction. While our research examines co-residence patterns in a context in which filial piety has been normative and where altruistic behaviour is said to drive many family-related behaviours, we cannot directly attribute the motivations behind decisions to move in or out of co-residential arrangements to particular ideological or altruistic drivers.Footnote 4 Instead, we address the factors that enhance intergenerational solidarity, highlighting the importance of parental needs, while also considering the role of opportunities for co-residence, as well as family structural and contextual factors.
Our primary concern is the extent to which the needs-based variables, health limitations and widowhood, are associated with Chinese co-residence patterns, net of age and other factors. Empirical evidence indicates, for example, that in addition to a parent's failing physical, cognitive and/or emotional health, the loss of a spouse in old age is particularly likely to prompt intergenerational co-residence (Knodel and Ofstedal, Reference Knodel, Ofstedal and Hermalin2002; Zhang, Reference Zhang2004; Zimmer and Korinek, Reference Zimmer and Korinek2010; Korinek et al., Reference Korinek, Zimmer and Gu2011; Lei et al., Reference Lei, Strauss, Tian and Zhao2015). As Li et al. (Reference Li, Liang, Toler and Gu2005: 637) state, ‘for many older adults, becoming widowed is perhaps the most difficult, yet inevitable, role transition’. Indeed, survivors often suffer (additional) physical and mental health deterioration (Williams et al., Reference Williams, Zhang and Packard2017), further complicating their circumstances. In China, marriage remains practically universal, so most older adults have the protection of spousal care, at least for a time. In addition, the centrality of spousal support has probably increased over time as the decline in co-residence with children has been matched by a rise in co-residence with only a spouse, particularly among younger elderly people (Zeng and Wang, Reference Zeng and Wang2003). The loss of a spouse is thus often associated with the loss of an integral support system that must be offset by other forms of familial or social support.Footnote 5 Since the likelihood of becoming widowed and of experiencing declining health increases with age, and since older age is also associated with an array of other risk factors such as increased social isolation, we consider age as an additional needs-based variable in our analysis.
We also assess whether socio-economic status (SES) is associated with co-residence patterns. SES attained through education and/or earnings can be related to either needs or opportunities for co-residence, or both. For example, while low SES may constitute a need for co-residence within this framework, higher levels of financial wellbeing can provide opportunities for shared living arrangements. At the same time, substantial wealth may allow elderly people and/or their kin to purchase alternatives to co-residence, net of their health-care or other needs (Chen and Chen, Reference Chen and Chen2016). For individuals from lower socio-economic backgrounds, the marginal benefits of co-residence and resource pooling tend to be greater than is true for those in wealthier families, as co-residence may be the primary way those with fewer financial assets receive assistance.
We consider two family structural variables in this analysis. These include (a) the number of living adult children, since having more adult children should increase the chances of having ‘at least one suitable child with whom respondents might prefer to live’ (Meng et al., Reference Meng, Xu, He, Zhang and Lin2017: 10); and (b) having at least one living adult son, because, as we have noted, sons have historically been the preferred gender in China.
Finally, although cultural-contextual structures are often assessed cross-nationally, they are also important to our study, as contextual differences continue to exist between rural and urban China. Again, as we have noted, rural elderly people are vulnerable in unique ways, given their lack of access to social safety nets. All else being equal, this would suggest that they have a higher need for co-residence than their urban counterparts. Yet, despite their higher vulnerabilities, rural elderly people may actually be less likely to live with an adult child, because with the widespread out-migration of young adults to urban areas, the ‘long time-space separation between the caregivers and their vulnerable parents increasingly becomes an obstacle for the [rural] elderly to access traditional routine care’, including co-residence (He and Ye, Reference He and Ye2014: 353; see also Giles et al., Reference Giles, Wang and Zhao2010).
Hypotheses
Based on the literature cited above, we hypothesise the following about the likelihood of elderly couples transitioning into or staying in co-residence with an adult child, relative to living independently in both waves:
(1) When one or both spouses report physical, cognitive or emotional health concerns at baseline, they will be more likely to be living in co-residential living arrangements at both time-points, or to shift into co-residence in the interval, than will their healthier counterparts.
(2) If one or both spouses experience deteriorating health in the interval, they will be more likely to shift into a co-residential living arrangement than will those who do not.
(3) Older individuals who lose a spouse in the interval will be more likely to shift into a co-residential living arrangement than will those whose unions are intact at baseline and follow-up.
(4) Older elderly couples will be more likely to live in a co-residential living arrangement at baseline and follow-up than will younger elderly couples.
(5) Older couples who have at least one adult son, and older couples with more adult children, will be more likely to co-reside at baseline and follow-up than will those without at least one adult son.
We do not posit specific hypotheses for income or education because while lower-SES couples may be more likely to co-reside at baseline and follow-up than middle-SES couples for needs-based reasons, they may also be less likely to co-reside for opportunity-related reasons, i.e. they may be unable to afford suitable housing. Similarly, wealthier families may be more likely to co-reside at baseline and follow-up, since they can afford more adequate housing for shared residence; yet, they may be less likely to co-reside since they can afford to live separately if they so desire. We also do not have a specific hypothesis about the role of urban versus rural residence, our single indicator of cultural-contextual structure, in shaping co-residence decisions because, as recent scholarship suggests, countervailing influences are currently shaping co-residence patterns in important ways in urban and rural contexts.
Data
The data for this study come from the CFPS, which is a bi-annual panel survey of Chinese communities, families and individuals across 25 provinces in China and is representative of 95 per cent of the Chinese population. The CFPS uses a multi-stage probability proportional to size sampling design. Counties (in rural areas) and administrative units (in urban areas) are the primary sampling units (PSUs). Administrative villages (in rural areas) and neighbourhood communities (in urban areas) are sampled within the PSUs and households are sampled within those villages and neighbourhoods. The first wave of the CFPS was conducted in 2010; however, our analysis draws on the 2012, 2014 and 2016 waves because more of the variables of interest to our analysis are consistently measured across those waves.
To construct our analytical data-set, we follow older couples (i.e. where at least one partner is age 65 or more at baseline) between one survey wave considered the baseline and the subsequent wave, which is considered the follow-up to it. We create a stacked data-set so that older couples from the 2012 wave constitute the first baseline (and the 2014 wave is the follow-up to it) and older couples from the 2014 wave, including surviving couples from the first baseline and newly sampled couples, constitute the next baseline, with the 2016 wave as its follow-up. To measure the impact of baseline health status on co-residence at follow-up, we treat the interval between successive waves as the observation period, so couple-intervals uniquely identify each observation in our analytical data-set. Given the stacked structure of our data-set, a couple can contribute up to two observations, so we adjust the standard errors in regression analyses to account for couple-level clustering.
Further, we restrict our analytical data-set to couples who have at least one adult child alive (age 21 or more) at baseline and follow-up, who have complete information on co-residency status at baseline and follow-up, who have complete information on sample weights and who have complete information on the follow-up status of both spouses (i.e. died in the interval or successfully re-interviewed at follow-up). We only include couples with at least one spouse alive at follow-up and successfully re-interviewed. We also drop couples or individuals who experienced a shift out of co-residence between waves as our analysis focuses on factors that predict staying in or shifting into a co-residential arrangement versus maintaining independent living.
For the combined baselines, we have 3,900 couples with at least one adult child alive at baseline. From this sample, nine couples were dropped because both spouses had died in the interval, four couples were lost to follow-up and four couples were dropped from the sample because they had no adult child alive at follow-up. Of the remaining 3,883 couples, 101 were dropped because of missing data on sampling weights, and the 218 who experienced a shift out of co-residence in the interval were also dropped, as noted above. Hence, 3,564 couples constitute the final analytical sample for this paper. Of these 3,564 couples, 1,291 couples appear twice in the analytical data-set (i.e. we have information for these couples for the 2012 baseline and 2014 follow-up and for the 2014 baseline and 2016 follow-up) and 982 couples appear once in the analytical data-set (i.e. we have information for these couples for either the 2012 baseline and 2014 follow-up or the 2014 baseline and 2016 follow-up).
When we assess the impact of couple's cognition status at baseline and couple's depression status at baseline on living arrangements across both waves, we limit our analysis to the 2012 baseline because cognition and depression were not measured consistently across waves and because the 2012 measures are preferable to those from 2014 for this analysis. The 2012 CFPS indicators of cognition (immediate word recall (IWR) and delayed word recall scores) are less closely associated with educational attainment than the CFPS 2014 measures of cognition (word test and mathematics test scores) and the CFPS 2012 measure of depression draws on a wider set of distress symptoms than does the 2014 measure.Footnote 6 Word recall scores are thought to be more independent of knowledge acquired through formal education – they are measures of working memory capacity and fluid intelligence (Xie et al., Reference Xie, Zhang, Tu, Ren, Sun, Lv, Ding, Hu and Wu2017).Footnote 7 The final sample size for this sub-sample is thus 1,671 couples and regression analyses that use this sub-sample do not cluster standard errors at the couple level.
The attrition of individuals between survey rounds due to death or loss to follow-up is a common issue in panel studies where older individuals are tracked (Li et al., Reference Li, Liang, Toler and Gu2005). From our original target sample, attrition was quite limited, but it was not random. For instance, in the few cases in which both spouses died in the interval, couples were more likely to have a wife with limitations at baseline or have both spouses with activity limitations at baseline or have at least one spouse with below-average word recall at baseline than was true of couples who were successfully followed-up and re-interviewed. The results are more mixed for couples who were lost to follow-up. While couples lost to follow-up were less likely to have a husband with limitations at baseline, they were more likely to have at least one spouse with poor word recall at baseline than couples who were successfully re-interviewed. The results of this paper should therefore be read keeping these selective attrition issues in mind.
Since we do not have complete case data for all the 3,564 couples in our sample, we use multiple imputations to generate ten imputed or complete data-sets. While there are no missing data for the dependent variable used in our analysis, 28 per cent of the analytical sample have missing data on at least one independent variable of interest.Footnote 8 Although missingness for our main independent variables is associated with observed values of other variables,Footnote 9 we can ensure valid statistical inference by imputing missing data using multiply imputed chained equations (Allison, Reference Allison2001). The results of the analysis do not change if we use more than ten imputations.
Multiple imputation is a simulation-based approach for analysing data-sets with missing values. It involves three steps: (a) filling in missing values with multiple sets of simulated values, effectively generating m completed data-sets (m = 10 here); (b) estimating the model of interest separately for each completed data-set; and (c) integrating the results from each analysis into a final result (Rubin, Reference Rubin1996). For this study, multiple imputation was implemented using the MI suite of commands for Stata (StataCorp, 1985). Reviews of the various strategies to deal with missing data conclude that multiple imputation is generally superior to traditional methods of handling missing values, i.e. listwise deletion, pairwise deletion and mean substitution (Allison, Reference Allison2001; Acock, Reference Acock2005).
Methods
Multinomial logistic regression models are used to identify the factors associated with living arrangements in both waves. Our outcome variable has three categories: (a) no co-resident adult child in either wave; (b) a shift from having no co-resident adult child at baseline to having at least one co-resident adult child at follow-up; and (c) at least one co-resident adult child at baseline and follow-up. Our analysis uses the first category as the base comparison group, and focuses on determining which couple-level predictors are associated with a relatively higher probability of shifting into co-residence between waves, as well as a relatively higher probability of being in a co-residential set-up in both waves.
In the CFPS, co-residence is defined as sharing a residential unit, namely sharing a kitchen. If an individual is away from his or her family household unit but is expected to return in three months or less and continue living with the family in the long-term, then he or she is considered to be a co-residing family member in the survey. For the full analytical sample, 2,011 couples had no co-resident child at baseline or follow-up, 281 couples experienced a shift into co-residence between waves, and 1,272 couples had a co-resident child at baseline and follow-up. For the sub-sample that uses the 2012 baseline and 2014 follow-up only, 962 couples had no co-resident child at baseline or follow-up, 136 couples experienced a shift into co-residence between waves, and 573 couples had a co-resident child at both baseline and follow-up.
Because we expect children to make co-residence decisions based, at least in part, on the vulnerability status of both parents, the key independent variables in this analysis are (a) couple-level measures of health and (b) union dissolution. To provide a holistic picture of how older couples’ health is associated with living arrangements, we examine multiple dimensions of health at baseline: self-reported health of both spouses, activity limitations of both spouses, word recall measures of both spouses and depression scores of both spouses. We also examine how changes in couple's health, namely changes in couple's activity limitations between waves, are associated with co-residence decisions. We construct our baseline couple-level measures such that they allow us to assess whether adult children respond differently to maternal and paternal vulnerability. The coding structure of our couple-level health measures is specified below.Footnote 10
Couple's activity limitations at baseline is a four-category variable that measures whether (a) neither spouse had any activity limitations at baseline; (b) only the husband had activity limitations at baseline; (c) only the wife had activity limitations at baseline; or (d) both spouses had activity limitations at baseline. Those in the first category constitute the reference group. In the CFPS, individuals were asked to self-report which activities – going outdoors, eating, performing kitchen activities, doing laundry, cleaning, taking public transportation, going shopping – they were unable to perform independently. This information was used to construct the activity limitation variable, i.e. whether the husband and/or wife had any of the seven specified activity limitations. The CFPS did not ask individuals about their ability to perform activities of daily living (bathing, dressing, feeding, toileting, transferring and continence), so we are unable to construct a limitations measure for those activities.Footnote 11
Couple's IWR score at baseline is a four-category variable that measures whether (a) neither spouse had an IWR score that was equal to or less than the mean minus half standard deviation (mean – 0.5 SD) cut-off for their age group; (b) only the husband had an IWR score that was equal to or less than the mean – 0.5 SD cut-off for his age group; (c) only the wife had an IWR score that was equal to or less than the mean – 0.5 SD cut-off for her age group; or (d) both spouses had IWR scores that were equal to or less than the mean – 0.5 SD cut-off their age group. Like the variable measuring couple's limitations at baseline, the first category constitutes the reference category. IWR scores measure the number of words (out of ten) that respondents were read and could correctly recall, in any order, immediately after the reading (Xie et al., Reference Xie, Zhang, Tu, Ren, Sun, Lv, Ding, Hu and Wu2017). Therefore, the IWR score ranges from 0 to 10, with a higher score representing higher cognitive capacity.
Couple's depression at baseline is a four-category variable that measures whether (a) neither spouse had significant depressive symptoms at baseline; (b) only the husband had significant depressive symptoms at baseline; (c) only the wife had significant depressive symptoms at baseline; or (d) both spouses had significant depressive symptoms at baseline. Couples in the first category constitute the reference group. We use the 20-item Center for Epidemiological Studies Depression Scale (CES-D) to determine the extent of depressive symptomatology for older couples in our analytical sample. CFPS respondents were asked to score how frequently they experienced 16 depressive symptoms and four contentment symptoms, on an ordinal scale of 1 to 4 (1 = almost never; 2 = sometimes, 1–2 days; 3 = often, 3–4 days; 4 = most of the time, 5–7 days), in the last week. To compute a composite score, we changed the ordinal scale to a 0–3 range and reverse-coded the items of contentment, then added up the responses for all symptoms. An older individual was determined to have significant depressive symptoms if they had a composite score of 16 or more (Radloff, Reference Radloff1977).
In addition to examining the association between baseline measures of couple-level health and co-residence patterns, we exploit our longitudinal data by examining how changes in older couple's health are associated with living arrangements. For this, we construct a five-category variable that captures changes in older couples’ activity limitations between baseline and follow-up: (a) neither spouse had limitations at baseline or follow-up (reference group); (b) at least one spouse had limitations at both baseline and follow-up; (c) neither spouse had limitations at baseline but at least one spouse developed limitations by follow-up; (d) union dissolved in the interval; and (e) all others.Footnote 12 Note that we are unable to create comparable measures for change in couple's depression and cognition, as the CFPS does not have consistent measures for these health variables in the 2012 and 2014 waves.
For all analyses other than the one focusing on changes in couples’ limitations over time, union dissolution in the interval (primarily caused by the death of a spouse between baseline and follow-up) is a separate vulnerability indicator. For this measure, we do not specify the gender of the spouse who remained alive at follow-up because the cell sizes become small; from the full analytical sample of 3,564 couples, 89 couples experienced union dissolution in the interval with only the female partner alive at follow-up and 39 couples experienced union dissolution in the interval with only the male partner alive at follow-up. Bivariate analysis (not shown) suggests that compared to couples who remained in union at follow-up, women who experienced widowhood in the interval were relatively more likely to shift into a co-residential arrangement with a child between waves or stay in a co-residential set-up in both waves; however, similar results were not observed for men who experienced widowhood in the interval.
Other couple-level variables believed to be associated with needs, opportunities, or family-structural or contextual-structural considerations for co-residence were measured at baseline:
• Couple's age is a dummy variable that indicates whether or not both spouses were age 75 or more at baseline.
• Couple's residence is a dummy variable that indicates whether or not, at baseline, the couple was living in a community classified as urban by the Chinese Census Bureau.
• Education level of the more educated spouse is a three-category ordinal variable that measures the highest level of education attained by the more-educated spouse (no education, primary, secondary or more). Couples where neither spouse had attained any formal education constitute the reference category.
• Couple's family income is a three-category ordinal variable that indicates the income tertile the couple belonged to at baseline (highest, middle, lowest). Income tertiles are calculated using per capita family income and those in the middle-income tertile constitute the reference category. Family income includes wage income, net business income, property income, transfer income and other income (e.g. transfers from non-coresident relatives/friends) of all family members living in the household and immediate family members who were not co-resident but were economically dependent on the household. Family income per capita is family income-adjusted for family size (Xie et al., Reference Xie, Zhang, Tu, Ren, Sun, Lv, Ding, Hu and Wu2017).
• Number of adult children is a four-category ordinal variable that measures the number of living adult children (one, two, three, four or more) the couple had at baseline. Couples who had only one adult child alive at baseline constitute the reference category.
• Had an adult son is a dummy variable that indicates whether or not the couple had at least one adult son alive at baseline.
Results
Table 1 displays sample characteristics. This table suggests that being in good physical and mental health at baseline, as measured by activity limitations, depression and IWR, was associated with living apart from adult children at both time-points. The same appears to be true of remaining free of activity limitations in both waves and remaining in union. In contrast, older couples (with both spouses over age 75) appear especially likely to have been co-resident with adult children at both waves, and those with more living children appear more likely to have shifted into co-residence than to have been living without an adult child at either wave. Those with at least one living son at baseline appear both more likely to have been co-resident at both time-points and more likely to have shifted into co-residence than to have been living without an adult child at either time. While these distributions are in the hypothesised direction, it should be noted that we cannot run tests of statistical significance for bivariate associations in this table because there are no estimation options or tests of independence for contingency tables using multiply imputed data. As a result, the column percentages here are simply suggestive of how older couples in different living arrangements are distributed across our variables of interest.
Table 1. Distribution of independent variables by co-residence status at baseline and follow-up

Notes: Multiply imputed weighted samples were used. Distributions for the following variables (couple's depression status at baseline, couple's immediate word recall (IWR) score at baseline) are for the 2012 baseline–2014 follow-up sub-sample (unweighted N = 1,671). Distributions for all the other variables shown here are for the full analytical sample (unweighted N = 3,564). The distribution of the baseline covariates and union dissolution in the interval across living arrangements are similar for the full analytical sample and for the sub-sample. CES-D: Center for Epidemiological Studies Depression Scale (20-item). SD: standard deviation.
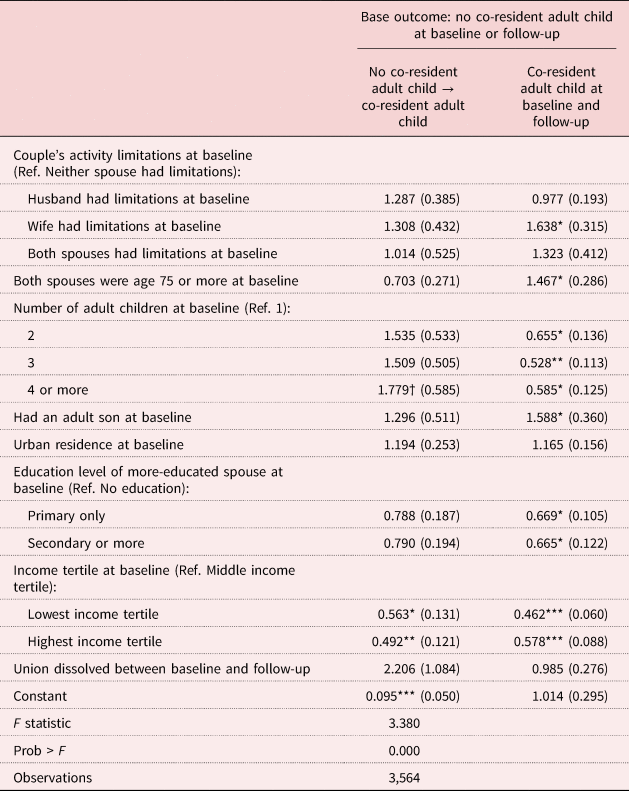
That said, simple multinomial logistic regressions that use no co-resident child in either wave as the reference outcome and examine associations between some of our primary variables of interest and stability/shifts into co-residence suggest that the associations are statistically significant at the bivariate level and in the direction expected (see Table 2). For instance, in comparison to cases in which neither spouse had activity limitations at baseline, when the wife had limitations at baseline, couples were more likely to live in a co-residential set-up in both waves. Similarly, in comparison to cases in which neither spouse had limitations at baseline or follow-up, when one or both spouses had limitations in both waves, couples were more likely to be co-residing in both waves. Further, compared to couples where neither spouse had limitations at either time-point, those who experienced union dissolution were somewhat more likely to shift into co-residence in the interval. The effect of union status is also significant when coded simply as a dummy variable, comparing those whose unions dissolved to those who were married at both time-points. Without controlling for other factors, those whose unions dissolved in the interval were more than twice as likely to shift into co-residence (vis-à-vis living independently from adult children) as were those who were married at both time-points.
Table 2. Simple multinomial logit regressions that describe the relationship between each main independent variable and living arrangements

Notes: Multiply imputed samples were used, and baseline cross-sectional weights applied to all the simple regressions above. Standard errors (SE) are in parentheses. Simple regressions that use couple's activity limitations at baseline, change in couple's activity limitations and union dissolution in the interval as the main independent variables use the full analytical sample (unweighted N = 3,564) and use SE clustered at the couple level. Simple regressions that use couple's immediate word recall (IWR) and couple's depression scores at baseline as the main independent variables use the 2012 baseline–2014 follow-up sub-sample (unweighted N= 1,671). Ref.: reference category. CES-D: Center for Epidemiological Studies Depression Scale (20-item).
Significance levels: † p < 0.1, * p < 0.05, ** p < 0.01.
Couples where the wife had poor cognition at baseline were nearly 40 per cent more likely to be in a co-residential arrangement in both waves than couples where neither spouse had poor cognition at baseline. Couples’ depression scores were associated with co-residential arrangements as well: when both spouses reported significant depressive symptoms at baseline, they were not only nearly 40 per cent more likely to be co-resident at both time-points, but also nearly twice as likely to experience a shift into co-residence between waves, than were couples where neither spouse had significant depressive symptoms.
Activity limitations
In Tables 3–6, we run multinomial logistic regressions to examine the net associations between our independent variables of interest and living arrangements. As we have indicated, all models in these tables use no co-resident adult child in either wave as the reference category.
Table 3. Multinomial logit regressions describing the relationship between couple's activity limitations at baseline and living arrangements
Notes: Relative risk ratios are reported. Standard errors are in parentheses and clustered at the couple level. Baseline cross-sectional weights have been applied. Ref.: reference category.
Significance levels: † p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001.
Table 4. Multinomial logit regressions describing the relationship between change in couple's activity limitations and living arrangements

Notes: Relative risk ratios are reported. Standard errors are in parentheses and clustered at the couple level. Baseline cross-sectional weights have been applied. Ref.: reference category.
Significance levels: † p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001.
Table 5. Multinomial logit regressions describing the relationship between couple's depression at baseline and living arrangements

Notes: Relative risk ratios are reported. Standard errors are in parentheses. Baseline cross-sectional weights have been applied. CES-D: Center for Epidemiological Studies Depression Scale (20-item). As per Radloff (Reference Radloff1977), older individuals who have CES-D score of 16 or more are classified as significantly depressed. Ref.: reference category.
Significance levels: † p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001.
Table 6. Multinomial logit regressions describing the relationship between couple's immediate word recall (IWR) at baseline and living arrangements

Notes: Relative risk ratios are reported. Standard errors are in parentheses. Baseline cross-sectional weights have been applied. Ref.: reference category. SD: standard deviation.
Significance levels: † p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001.
Consistent with the simple regression described in Table 2, Table 3 suggests that, net of other factors, compared to couples where neither spouse had activity limitations at baseline, when the wife had activity limitations, couples were more likely to live with an adult child in both waves. Union dissolution in the interval does not remain significant in this table; however, we find more support for our hypothesis that the loss of spouse brings about a need for intergenerational co-residence in Tables 4–6.
Further, several of our baseline variables in Table 3 are in the direction hypothesised. Couples who were older and who had at least one adult son were more likely to co-reside with an adult child in both waves. Although we did not posit a specific hypothesis for either education or income, the same was true of couples with no formal schooling. These findings suggest that older parents’ needs (associated with older age, and with no educational attainment), as well as family structure considerations (availability of an adult son) help shape co-residence patterns. We also find a non-linear relationship between income and the probability of co-residence, as couples in the lowest and highest income tertiles were both less likely to shift into co-residence between waves or co-reside in both waves than were couples in the middle-income tertile. While for the wealthier couples this might represent an ability to purchase alternative arrangements, for the poorest couples, who have fewer resources to begin with, the lack of opportunity to pool those limited resources via intergenerational co-residence may represent additional disadvantage. More generally, the results pertaining to income highlight the tension that exists between having the need to co-reside versus having the opportunity to co-reside (and having the opportunity to live independently out of choice). Lastly, we find that the relationship between the variable measuring number of adult children at baseline, and co-residence, is more complex than hypothesised. On the one hand, couples with four or more children were more likely to transition into co-residence with a child than couples with only one child; on the other hand, couples with two or more children were less likely to live with an adult child in both waves compared to couples with only one child.
We further utilise the longitudinal structure of our data to examine how changes in couple's health-care needs, measured in terms of changes in couple-level disability between waves, correlates with living arrangements. Net results shown in Table 4 indicate that when one or both spouses had limitations at both time-points, they were more likely to be co-residing with an adult child at both waves than were couples who reported no limitations at either wave. Table 4 also reaffirms the salience of union dissolution as a form of vulnerability affecting intergenerational co-residence; compared to those without disability at either time-point and whose marriages remained intact, older individuals who lost a spouse between waves were more likely to experience a shift into co-residence with a child. We did not find, as hypothesised, that couples who were in good health at baseline but experienced a deterioration in health in the interval were more likely to shift into co-residence; but the association between other couple-level health changes and living arrangements are as expected. Other baseline variables in this table display similar associations with living arrangements as seen in Table 3.
Depression
While Tables 3 and 4 examined the association between functional health and living arrangements, Table 5, which uses the 2012 baseline–2014 follow-up sub-sample, examines how parents’ emotional health-care needs (measured in terms of depressive symptomatology at baseline) are associated with living arrangements. In keeping with our hypothesis, we find that our two main measures of elderly needs are significantly associated with shifts into co-residence, net of other factors. We find that shifts into co-residence were more likely (a) among couples where both spouses had significant depressive symptoms at baseline than among couples where neither spouse had significant depressive symptoms; and (b) among elderly people who experienced union dissolution between waves than among those who were in union in both waves.
Cognition
Table 6, which also uses the 2012 baseline–2014 follow-up sub-sample, looks at the relationship between couple-level cognition at baseline and living arrangements. The results in this table are again consistent with the intergenerational solidarity framework and in keeping with the results of Tables 3–5; older couples’ cognitive health-care needs, much like their disability and emotional health-care needs, shape co-residence patterns in present-day China. Table 5 shows that co-residence at both time-points was more likely when the wife had poor word recall for her age group than when neither spouse had poor word recall for their age group. The results from Table 6, like those from Tables 4 and 5, also suggest that union dissolution in the interval was, as expected, correlated with shifts into co-residence. For the most part, other baseline variables have the same associations with living arrangements as seen in prior tables.
Summary and discussion
Older Chinese adults who are in poor health and/or who are widowed are in many ways vulnerable in contemporary China. While ongoing demographic and social changes have reduced the number of potential care-givers for the growing elderly population, state support for elderly people remains largely inadequate, further emphasising the importance of intergenerational care-giving within families. In this paper, we analyse couple-level panel data from CFPS and ask whether older parents’ needs in China, specifically those arising from poor physical, cognitive and emotional health, or from loss of a spouse, motivate a specific type of intergenerational solidarity: co-residence. We also examine the relevance of other micro-level needs and opportunities, and meso- and macro-level structural considerations for co-residence. We specifically add to the existing literature by (a) conceptualising older generations’ needs in a novel way – at the couple level rather than at the individual level – because, we argue, children make co-residence decisions based on the vulnerabilities of both parents; and (b) examining the relevance of intergenerational solidarity theory for present-day China, drawing on more recent panel data than was available for prior studies.
Our results are in keeping with our theoretical framework and primary hypotheses, showing consistent associations between various measures of parents’ needs and living arrangements. We find that shifts into co-residence were more likely when both parents had relatively high depression levels at baseline, and when a parent lost a spouse in the interval. We also find that when the mother had poor cognition at baseline, when the mother had activity limitations at baseline, and when both parents had limitations at both baseline and follow-up, the probability of intergenerational co-residence at both waves was higher than it was for less-vulnerable counterparts. Similarly, net of health concerns, older parents were more likely to co-reside with an adult child in both waves than were younger parents. This may signal recognition that older elderly people are likely to become increasingly frail and in need of assistance as time passes.
From an international comparative perspective, these results suggest two things. First, adult children in China today, much like adult children in various other contexts, actively respond via co-residence to parental needs reported at baseline or to shifts in need brought about by widowhood. Second, adult children are likely to be in co-residence or stay in co-residence with older parents who report health needs at baseline or who seem likely to develop such needs over time. Thus, consistent with the results of the Japan study by Brown et al. (Reference Brown, Liang, Krause, Akiyama, Sugisawa and Fukaya2002), cited above, anticipatory co-residence (such that adult children co-reside with ageing parents, foreseeing a decline in physical or mental health) appears to be a possibility in China. The comparison with Japan is of course suggestive, since with our data we cannot determine the precise motivation for or timing of entry into co-residence for those who were already co-residing at baseline.
While our analysis indicates that health concerns, loss of a spouse and older age are all associated with co-residence patterns, evidence regarding other needs and opportunity-based factors is more mixed. This is consistent with the trade-offs between needs and opportunities suggested in the literature. For example, although lack of a formal education predicts intergenerational co-residence in both waves, our results for family income highlight the tension between having the need to co-reside versus having the opportunity to co-reside. The intergenerational solidarity framework suggests that both needs and opportunity structures are important for making co-residence possible. We find that those in the lowest income tertile, who tend to have the greatest need for resource pooling from co-residence, have a lower probability of co-residing at follow-up than those in the middle income tertile, who likely have better housing and other financial resources and thus a relatively greater opportunity to share living arrangements. That said, we also find that those in the highest income tertile are less likely to share accommodations than those in the middle-income group, probably because their affluence enables them to purchase substitutes for co-residence and to live independently out of choice. This preference for, and implementation of, independent living among wealthier older couples is not China-specific; it is also increasingly evidenced in other Asian countries such as South Korea (Kim and Rhee, Reference Kim and Rhee1997), Japan (Brown et al., Reference Brown, Liang, Krause, Akiyama, Sugisawa and Fukaya2002), Indonesia and Singapore (Frankenberg et al., Reference Frankenberg, Chan and Ofstedal2002).
The differing dynamics observed across income groups are noteworthy not only because they highlight how micro-level needs and opportunities influence co-residence, but also because they provide some insight into how living arrangements may evolve going forward. While the current generation of older adults may expect and want to co-reside with children, particularly at times of heightened need, over time, as economic opportunities and cultural mores continue to change, preferences for living together may decline, yielding to preferences for more independent living and other alternatives.
Living arrangements are shaped by meso-level family structural conditions as well, and our results highlight the ongoing importance of a particular structural condition – the availability of a male child – for co-residence in both waves in China. With declining family size, the durability of a support system that is heavily reliant on adult sons will be increasingly tested. Yet, it should be reiterated that co-residential living is only one form of care-giving; non-coresident sons and daughters can support parents through quasi co-residence or through short-term co-residence.
Finally, our results do not find a significant association between the one contextual-structural variable we are able to assess, rural–urban residence, and living arrangements. This non-significant result does not necessarily mean that contextual factors do not matter for living arrangements and for the wellbeing of elderly people in China, however, and the scope of analysis in this paper does not allow us to disentangle the different dynamics that are at play. Earlier work has identified numerous ways in which rural elderly people's need for co-residence conflicts with space and time considerations that make it harder for their migrant adult children to respond effectively when needed, and current policy continues to leave elderly people in remote rural villages highly vulnerable. A hybrid policy approach that combines the expansion of social safety nets, local work opportunities for youth and a reduction in barriers to mobility for elderly people is going to be necessary for meeting the needs of rural elderly people and their family members going forward (Giles et al., Reference Giles, Wang and Zhao2010; Song, Reference Song2017).Footnote 13
Limitations
This study has several limitations. In addition to the selective attrition that occurred over time (discussed above), the analysis we have presented only considers how the needs of older parents shape co-residence decisions. We are not able to assess the ways in which child care and other needs of adult children also motivate multi-generational co-residence in present-day China (Chen, Reference Chen2005; Chen et al., Reference Chen, Liu and Mair2011; Ko and Hank, Reference Ko and Hank2014). That said, we did conduct additional analyses (not shown) to account for the middle-generation's child care needs by including a four-category variable for the presence of a co-resident grandchild.Footnote 14 The purpose of this was to see whether older couples’ shifts into co-residence with an adult child were correlated with the shifts into multigenerational co-residence with a young grandchild to potentially care for and we found a significant positive association between these two transitions.Footnote 15 We also found that after controlling for adult children's potential child-care needs, older parents’ needs (arising from poor health and/or widowhood) continue to raise significantly the probability of shifts into co-residence or co-residence in both waves. Given this, our main finding that older parents’ needs help shape co-residence decisions still holds; in fact, our additional analysis provides suggestive evidence that living together allows the older and the middle generation to meet their needs simultaneously.
Our analysis is also limited because our data do not allow us to determine whether shifts into co-residence are achieved by adult children moving in with older parents or older parents moving in with their children. Relatedly, we do not have information on the head of the household at follow-up. This is important because the process through which co-residence is achieved and the distribution of decision-making power in a co-residential arrangement could potentially have implications for the future health status of elderly people and vice versa. Finally, many older couples are likely to experience multiple vulnerabilities simultaneously (e.g. they can experience union dissolution and worsening health), and while we are unable to analyse the effects of this, given cell size considerations, future research that uses larger samples with more data on the timing of events could consider the ways in which concurrent or sequential vulnerabilities affect co-residence patterns.






