



Introduction
In recent years, rumination has gained attention as a possible transdiagnostic cause, exacerbator and maintenance factor in psychiatric disorders, as well as a potent target for treatment, particularly the cognitive behavioural therapies (Luca, Reference Luca2019; Watkins and Roberts, Reference Watkins and Roberts2020). In post-traumatic stress disorder (PTSD), rumination often takes the form of repetitive thinking about the trauma and its consequences, such as thoughts about justice, revenge, how the trauma could have been prevented, or the impact it has had on the patient’s life (Ehlers and Clark, Reference Ehlers and Clark2000; Speckens et al., Reference Speckens, Ehlers, Hackmann, Ruths and Clark2007).
A recent review found the connection between rumination and PTSD symptomatology to be well-established (Moulds et al., Reference Moulds, Bisby, Wild and Bryant2020). Meanwhile, ruminations and the intrusions characteristic of PTSD are found to be distinct on both a theoretical, phenomenological and functional level (Ball and Brewin, Reference Ball and Brewin2012; Ehlers and Clark, Reference Ehlers and Clark2000; Ehlers et al., Reference Ehlers, Hackmann and Michael2004; Ehlers and Steil, Reference Ehlers and Steil1995; Joseph et al., Reference Joseph, Williams and Yule1997). Based on the current literature, intrusions will be defined in this study as a recollection of the trauma itself with a sense of ‘nowness’ and a re-experiencing of central sensory impressions. In contrast, rumination in PTSD is defined as post-event repetitive, evaluative chains of verbal thoughts of a less concrete nature, often thoughts about consequences of the trauma, e.g. ‘Why did this happen to me?’ or ‘Why do I keep having these symptoms?’ (Hackmann et al., Reference Hackmann, Ehlers, Speckens and Clark2004; Speckens et al., Reference Speckens, Ehlers, Hackmann, Ruths and Clark2007). Also, their duration differs, as intrusions often last only a matter of seconds or very few minutes, while rumination can take place for minutes or even hours at a time (Speckens et al., Reference Speckens, Ehlers, Hackmann, Ruths and Clark2007). Further investigation of the relationship and co-occurrence of these phenomena is vital to future development of theories and treatment targets in psychotherapy.
Rumination in PTSD
Evidence, both from experimental and correlational cross-sectional designs, has shown that rumination plays a part in the development and maintenance of PTSD symptoms (Ball and Brewin, Reference Ball and Brewin2012; Kubota and Nixon, Reference Kubota and Nixon2017; Laposa and Rector, Reference Laposa and Rector2012; Santa Maria et al., Reference Santa Maria, Reichert, Hummel and Ehring2012; Szabo et al., Reference Szabo, Warnecke, Newton and Valentine2017; Zetsche et al., Reference Zetsche, Ehring and Ehlers2009). It has also been shown to be a predictor of symptom severity and chronicity in PTSD (Birrer and Michael, Reference Birrer and Michael2011; Nolen-Hoeksema and Morrow, Reference Nolen-Hoeksema and Morrow1991). Finally, rumination plays a well-established role in depression and depressive symptoms, which are often seen co-morbid to PTSD (Ehring et al., Reference Ehring, Frank and Ehlers2008; Elhai et al., Reference Elhai, Grubaugh, Kashdan and Frueh2008).
Rumination in PTSD can be understood as a maladaptive coping strategy, both cognitively and emotionally. Cognitively, rumination hinders effective goal-directed problem-solving and processing of the traumatic event, as it is abstract and involves avoiding emotional connection to and cognitive reappraisal of the trauma (Ball and Brewin, Reference Ball and Brewin2012; Ehlers and Clark, Reference Ehlers and Clark2000). Parallel to being a cognitive coping strategy, rumination can function as a maladaptive emotion regulation strategy (Aldao et al., Reference Aldao, Nolen-Hoeksema and Schweizer2010), with evidence from a community sample with a high level of PTSD linking it to problems in emotion regulation (Pugach et al., Reference Pugach, Campbell and Wisco2020). As such, rumination may be utilized in response to the experience of intrusions (Birrer and Michael, Reference Birrer and Michael2011; Michael et al., Reference Michael, Halligan, Clark and Ehlers2007), potentially as a form of emotional avoidance (Ehlers and Clark, Reference Ehlers and Clark2000). However, rumination as cognitive and emotional coping strategies seems inefficient – ruminating about the trauma has been found to result in intrusions ‘often’ or ‘always’ for 65% of a PTSD-patient sample (Birrer and Michael, Reference Birrer and Michael2011), and experimental studies have shown that ruminating about a traumatic experience can maintain intrusions (Kubota et al., Reference Kubota, Nixon and Chen2015; Santa Maria et al., Reference Santa Maria, Reichert, Hummel and Ehring2012). Experimental, longitudinal and cross-sectional studies with mediation analyses on PTSD and depression patients as well as healthy participants suggest a connection between ruminations and dysphoria, anxiety, or other negative feelings. These could then function as internal triggers for intrusions (Ball and Brewin, Reference Ball and Brewin2012; Brown et al., Reference Brown, Hetzel-Riggin, Mitchell and Bruce2018; Michael et al., Reference Michael, Halligan, Clark and Ehlers2007; Newby and Moulds, Reference Newby and Moulds2012; Smets et al., Reference Smets, Luyckx, Wessel and Raes2012).
Thus, it is evident that rumination plays an important role in PTSD, but the exact relationships between rumination, intrusions and underlying mechanisms are currently unresolved. Evidence so far suggests a bidirectional influence between intrusions and rumination, leading to a vicious, self-maintaining circle, although the strength of causality may not be equal in both directions. A recent review reports that evidence on the matter so far is mostly based on retrospective self-report measures, interviews, and/or non-PTSD samples (Szabo et al., Reference Szabo, Warnecke, Newton and Valentine2017), leaving a need for clinical, real-time investigations of the phenomena in PTSD populations.
High-resolution symptom registration with the wearable One Button Tracker
When investigating symptom occurrence and frequency, researchers and therapists typically rely on verbal or written, retrospective self-report. However, self-report risks capturing metacognitive beliefs about the symptom rather than the phenomenon itself, as well as being biased by state factors (Rosenkranz et al., Reference Rosenkranz, Takano, Watkins and Ehring2020). Furthermore, problems with concentration and memory are common in PTSD, making memory an unreliable source of information. Even when a registering scheme is used several times a day, the information will be prone to substantial recall bias (Trull and Ebner-Priemer, Reference Trull and Ebner-Priemer2009), typically towards more negative experiences, and registration being forgotten or neglected because of the effort required (Shiffman et al., Reference Shiffman, Stone and Hufford2008).
The field of ecological momentary assessment (EMA) addresses the issues in autobiographical recall, securing ecologically valid observations by having the participant report experiences in or close to the context and time in which they occur (Schiffman et al., Reference Shiffman, Stone and Hufford2008; Trull and Ebner-Priemer, Reference Trull and Ebner-Priemer2009). In recent years, the development of smartphones and wearable technologies has contributed significantly to this methodology by making it easier to collect data with higher temporal resolution and closer contextual proximity to real life outside of assessment or therapeutic sessions (Griffin and Saunders, Reference Griffin and Saunders2020).
However, there is still a need to refine methods in order to obtain data with a higher level of quality in terms of accuracy, precision and adherence. Former studies have shown compliance rates using electronic diaries ranging from 50 to 90% (Schiffman et al., Reference Ehring, Frank and Ehlers2008). A recent study by Yang et al. (Reference Yang, Ryu and Choi2019), which measured mood and stress over a week using a smartphone-based self-report app, had a completion rate of only 70.66% (out of the number of scheduled measures). The study saw a rapid decline in rates after 5 days of use, hinting that participants quickly experience fatigue in answering an array of questions. Also, in studies involving traditional EMA methods, participants typically report with less reliability when symptoms worsen (Griffin and Saunders, Reference Griffin and Saunders2020). That is, EMA schemes typically prompt the participant to register phenomena in relation to time intervals, random or set. However, it is possible that this form of time-based prompting may trigger intrusions in itself (so-called reactivity; Rattel et al., Reference Rattel, Grünberger, Reichenberger, Liedlgruber, Miedl, Blechert and Wilhelm2019), and/or lead to inflated reporting of intrusions in clinical samples (Kleindienst et al., Reference Kleindienst, Priebe, Petri, Hecht, Santangelo, Bohus and Schulte-Herbrüggen2017).
The wearable One Button Tracker employed in this study was developed to offer a simple, accessible, and discrete method to track psychological phenomena, as it can be operated without looking at it and in less than a second. Registering with the instrument is driven by the participant’s subjectively experienced phenomena, as defined by the clinician and participant in collaboration, in the moment they occur. This ensures the highest possible temporal resolution, as well as enhancing the sense of agency for the participant and consequently aiding adherence (Larsen et al., Reference Larsen, Eskelund and Christiansen2017).
The aim of this proof-of-concept study was to advance clinical research on rumination and intrusions in PTSD by investigating whether it was possible to differentiate between the phenomena in a clinical population in the patients’ everyday lives, as well as the possibility of investigating the nature of the relations between them. This was executed with the aforementioned novel One Button Tracker, which was developed to address validity issues caused by attention and memory difficulties, as well as factors related to adherence. The instrument produces high-resolution data in real time, making it particularly suited to investigate temporal relations between psychological phenomena.
The study’s aims were therefore twofold, exploring the following hypotheses: (a) rumination and intrusions appear subjectively as distinct phenomena when experienced by PTSD patients and (b) rumination and intrusions can be assessed separately in daily living using a wearable self-tracking instrument in a way which provides potential to further investigate the temporal relations between the phenomena. In addition to the investigation of the One Button Tracker’s potential in theoretical research on psychological phenomena, results were also evaluated with an eye to their value for use in psychotherapy.
The following criteria were used to evaluate the hypotheses:
-
Participants confirming subjectively to be able to differentiate between rumination and intrusions in their daily lives and that differentiating the two phenomena were experienced as meaningful.
-
Participants reporting being able to register the phenomena using the tracking instrument, with the data from the tracker instrument confirming proximate adherence via comparison of the baseline week and second week frequencies (see ‘ Procedure ’ in Method section).
-
Participants’ reports of occurrence and temporal relationship between intrusions and rumination concur with data obtained via use of the One Button Tracker. Both should show a temporal proximity between the phenomena, with the quantitative data providing additional information over and above the verbal self-report.
Method
The study was a proof-of-concept case study with two participants, lasting a period of approximately 2 weeks. The participants were recruited from a larger data collection in a study testing a mobile application for PTSD (Scharff et al., Reference Scharff, Lau, Riisager, Moeller, Salimi, Gondan and Folke2020). As a part of that project, the participants had been diagnosed with PTSD by two independent researchers, both clinical psychologists. The initial intake session was a part of an assessment for referral to treatment in the Mental Health Service, Capital Region, Denmark (MHS-CRD; Danske Regioner, Reference Danske2017), where PTSD symptoms, including intrusions, were assessed in an interview based on the criteria in the ICD-10 (World Health Organization, 1993), and rumination was assessed briefly based on a clinical description of the phenomenon (see Appendix B in the Supplementary material). In a second intake session, the Mini-International Neuropsychiatric Interview (MINI; American Psychiatric Association, 2013; Sheenan et al., Reference Sheenan, Lecrubier, Sheenan, Amorim, Janavs and Weiller1998) was used to formally assess symptoms of PTSD and generalized anxiety disorder, including intrusions and rumination, as well as other mental disorders. Finally, self-report accounts of intrusions were assessed using the PTSD Check List for DSM-V (PCL-5) and the International Trauma Questionnaire (ITQ) along with other self-report measures not reported in this study. For a full description, see Scharff et al. (Reference Scharff, Lau, Riisager, Moeller, Salimi, Gondan and Folke2020).
Inclusion criteria were:
-
Minimum 18 years of age.
-
Referred to PTSD package treatment in the MHS-CRD, i.e. living up to the ICD-10 criteria for PTSD with at least moderate severity.
-
Both ruminations and intrusions were present. No pre-defined criteria were set for the frequency of rumination or intrusions.
Exclusion criteria were:
-
Acute suicidal risk at the time of referral to treatment in the MHS-CRD.
-
Untreated bipolar or psychotic disorder.
-
Present or recent substance abuse (where ‘recent’ is defined as within the last 3 months).
-
Inability to understand and/or read Danish.
-
Concurrent psychiatric or psychological treatment outside of the MHS-CRD.
Participants
Participant A was a 30-year-old woman who had been physically assaulted 10 years prior to referral. After an exacerbation in symptoms, she was formally diagnosed with PTSD and referred to treatment in MHS-CRD a few months prior to this study. Due to a waiting list for initiation of treatment, she had not yet commenced treatment at the inclusion time of the study. Participant A had frequent intrusions but reported at the intake interview that she thought she seldomly ruminated. However, her self-report measures showed that there was some rumination present (see Results), and she was included in the study on the basis of high motivation. She was treated with sertraline-hydrochloride at the initiation of the study period by a psychiatrist independent of the study.
Participant B was a 23-year-old woman, who as a child of primary school age had witnessed a close family member becoming the victim of a gunshot. She had lived with PTSD symptoms since the trauma but was only formally diagnosed prior to referral to PTSD treatment in the MHS-CRD. Shortly after the referral, but before commencement of treatment, she completed the 14 days tracking regime. Participant B described herself to be affected by a great deal of both rumination and intrusions. She was not taking psychotropic medication during the project period.
Procedure
Participants were invited to three sessions in the laboratory for instruction, training, and debriefing. These were interspaced by two approximately 1-week data collection periods. For participant A, for logistical reasons the first and second periods lasted 10 days and 7 days respectively, totalling 17 days of tracking. For participant B, the sessions took place with 1-week intervals, totalling 14 days of tracking (see Table 1).
Table 1. Overview of the duration of the case studies and the number of observations registered by the two participants

At the first session, the participant filled out self-report measures (for a description, see the Materials section below) and was instructed to track mood levels daily on a visual analogue scale (VAS) throughout the study. The participant was then given a brief psychoeducation about intrusions and ruminations, based on the definitions as described in the Introduction and in Appendix B (see Supplementary material), and was instructed to register them with a single press on the One Button Tracker without distinguishing between the two phenomena. This first week of data collection was carried out for several reasons: firstly, to establish an individual baseline for the frequency of occurrence of both phenomena. A comparison of the frequency of ruminations and intrusions combined between the first and second week of tracking was used to provide a proximate proof of the participants’ adherence to the tracking regime, in that high adherence and consistency in tracking could be assumed to produce approximately the same registration frequencies for the two weeks. In order to qualify the level of adherence with the available data, observations from both weeks 1 and 2 are provided for inspection in the present article (Table 1; Figs 3 and 4).
Secondly, the first week of registering functioned as a practice period in which the participant was able to train self-tracking and the use of the instrument, as well as explore and gain awareness of and experience intrusions and rumination. This practice period took place in order to provide the highest possible validity of data when differing between the phenomena in the second week. Furthermore, the practice period provided a starting point for the subsequent psychoeducation in the differences between the phenomena.
In the second session, the participant filled out the same self-report measures. Then followed a brief presentation of the self-collected data, which was shown to the participant in a visual representation and held up against the results on the mood scale. Subsequently, the participant underwent a training module on intrusions and ruminations in order to be able to differentiate between the two phenomena as they occurred (see a detailed description in the Materials section below). The participant was then instructed to differentiate between the phenomena in the second tracking period and register observations with a short and long button press, respectively. The procedure with long and short presses – and not, e.g., one and two presses – was chosen to intuitively reflect the nature of the briefer intrusions versus ruminations of typically longer duration, thus aiding the participant in remembering the protocol.
In the third session, the participant repeated the self-report measures and was again presented with the self-collected data, which were held up against the mood scores. Finally, the participant gave a brief, semi-structured interview, approximately 20 minutes in duration, about the experiences of tracking intrusions and rumination (see interview guide in Supplementary material Appendix A).
Materials
One Button Tracker
The One Button Tracker consists of a small box with one round button and is wearable on a watch-like strap, alternatively as a necklace or carried around in a pocket. The design has been developed to ensure ease of use, i.e. having only one button makes it possible to administer it without looking at it. The instrument records all presses on the button directly onto the internal storage of the device, including the duration (in milliseconds) of the press. Data can be transferred via a USB connection to any compatible personal computer, where a web-based application provides instant data analysis with visualizations depicting the occurrence of the investigated phenomena, grouped according to time of day, week day and month. A full charge of the instrument’s battery lasts for approximately 30 days and the battery is recharged using the USB cable.
Training module
The training module in the second session was designed to teach the participant to distinguish between ruminations and intrusions in the second week of tracking. The first part of the module was the Intrusion and Rumination Interview (for a detailed description, see Speckens et al., Reference Speckens, Ehlers, Hackmann, Ruths and Clark2007), which consists of two parts each covering intrusions and rumination. Using the interview in the context of this study served to educate about the phenomena rather than classify content scientifically, as in Speckens and colleagues’ original study. The interview asks the participant to come up with examples of typical intrusions and rumination and describe them in terms of duration, the subject and content of the intrusion/rumination, degree of sensory versus verbal/cognitive content, and the accompanying feelings. The interview would then feed into a dialogue with the participants about the differential phenomenological experiences of rumination and intrusion, relating their unique experiences to the theoretical characteristics (with ruminations and intrusions defined as in the Introduction of this article). To aid in memory for use throughout the remainder of the study, participants were given a take-home sheet with the most important differences between rumination and intrusion (see Appendix B in the Supplementary material).
For participant B, the interview was modified slightly according to her own wish, leaving out parts of the original interview about triggers and the particular content of thoughts and intrusions which touched upon certain emotionally sensitive parts of her trauma. The retained parts of the interview were deemed sufficient by the research team for its psychoeducative purpose in this study.
The participant was then given a quiz of 10 vignettes describing either rumination or intrusion; after going through the answers given by the participant, she was administered another six vignettes which had to be answered correctly in order for the participant to qualify for tracking in week 2 (see Appendix C in the Supplementary material). Participant A answered all 16 items correctly. Participant B answered correctly on nine out of the 10 initial items, and answered all six items correctly in the additional vignettes. In conclusion, the participants were thus both deemed to be able to sufficiently distinguish between rumination and intrusion.
Self-report measures
The participants were assessed with the following self-report measures at the baseline session, as well as at the second and third sessions (except for the PCL-5, which was administered at the initial data collection for the context study only):
Mood Visual Analogue Scale (VAS)
The participant’s mood was registered daily on a 14 cm VAS (Heller et al., Reference Heller, Manuguerra and Chow2016) at approximately the same time every day, around bedtime. The scale went from Negative over Neutral to Positive mood along the length of the VAS line.
Generalized Anxiety Disorder 7-item Scale (GAD-7; Reference Spitzer, Kroenke, Williams and LöweSpitzer et al., 2006)
The GAD-7 scale assesses the severity of generalized anxiety. Participants rate the frequency with which they experience symptoms of anxiety. Cut-offs for mild, moderate and severe anxiety are 5, 10 and 15, respectively (range 0–21).
Hamilton Depression Rating Scale, self-report (HAM-D6; Reference Timmerby, Andersen, Søndergaard, Østergaard and BechTimmerby et al., 2017)
The HAM-D6 consists of six items which assess symptoms of depression. Participants rate intensity of symptoms on a Likert scale, with cut-offs of 7, 9 and 12 for mild, moderate and moderately severe/severe depression, respectively (range 0–22).
PTSD Checklist for DSM-V (PCL-5; Reference Weathers, Litz, Keane, Palmieri, Marx and SchnurrWeathers et al., 2013)
The PCL-5 consists of 20 items measuring the 20 PTSD symptoms in the DSM-V. The items are scored on a 5-point Likert-scale indicating the degree to which a particular symptom has been present in the past month.
Response Style Questionnaire (RTQ)
The Ruminative Response Scale (RRS) subscale of the RTQ was used to assess trait rumination (Nolen-Hoeksema and Morrow, Reference Nolen-Hoeksema and Morrow1991). The RRS consists of 22 items which assess ruminative responses to sad and depressed mood. Participants rate the frequency of their use of unhelpful ruminative strategies, with higher scores suggesting higher levels of rumination (range 22–88).
The Metacognitive Anger Processing scale (MAP; Reference MoellerMoeller, 2016)
The MAP is a 26-item scale, scored from 1 (‘never’) to 4 (‘all the time’). It assesses metacognition in relation to anger in three domains: uncontrollable anger rumination (e.g. ‘I cannot let go of angry thoughts’; 9 items), positive beliefs about the functions of anger (e.g. ‘anger helps me solve problems’; 9 items), and negative beliefs related to anger, particularly those focused on danger, harm and madness in association with anger (e.g. ‘anger could make me go mad’; 8 items). We distributed the whole instrument, but for the relevance of this study, only scores from the anger rumination subscale (range 9–36) will be presented.
Penn State Worry Questionnaire (PSWQ; Reference Meyer, Miller, Metzger and BorkovecMeyer et al., 1990)
The PSWQ consists of 16 items which assess the general disposition to worry. Participants rate to what extent they identify with statements about worrying, with higher scores suggesting higher levels of worry (range 16–80; 16–39 points signify low worry, 40–59 moderate worry, and 60–80 high worry).
Analysis
Quantitative data
The data generated by the One Button Tracker is a time series of observations with precision in seconds. Each event corresponds to an activation of the button and includes the duration of the button press in milliseconds. For each participant, we processed the data from the tracking instrument by observing the duration of the button press. This enabled us to split it into two time series representing intrusions (short press) and rumination (long press), respectively. This was done by making a cut-off between the maximum length of presses in the first week (where the participant was only instructed to use short presses) and the length of long presses in the second week. The cut-off between a long and short press was established for each participant through visual inspection of a graph showing duration of presses for the observations.
Further processing of the data included counting the number of observations per day for intrusions and ruminations, respectively. To assist our analysis of the temporal order and possible causality of intrusions and ruminations, we calculated the temporal distance between observations of the two phenomena which were close in proximity. A length of one hour between the occurrence of the phenomena was chosen as a lenient cut-off for proximity. No further clean-up or processing of the collected data was performed.
De-briefing interview method and analysis
The de-briefing interview was carried out as a semi-structured interview with questions directed at possible positive and negative effects of symptom tracking and new insights acquired, as well as the experienced distinction between ruminations and intrusions (see Appendix A in the Supplementary material). The interviews were transcribed verbatim and data were analysed and coded for emerging themes in relation to the research questions.
Results
Self-report questionnaires
The self-report measurements for both participants can be seen in Figs 1 and 2. Furthermore, both participants experienced PTSD symptoms at baseline as registered on the PCL-5, with participant A experiencing the highest symptom load with a score of 71 (highest possible score: 80), and participant B scoring 57 points. Both participants also experienced moderate to severe levels of depressions and anxiety, as measured on the HAMD-6 and GAD-7, throughout the study.
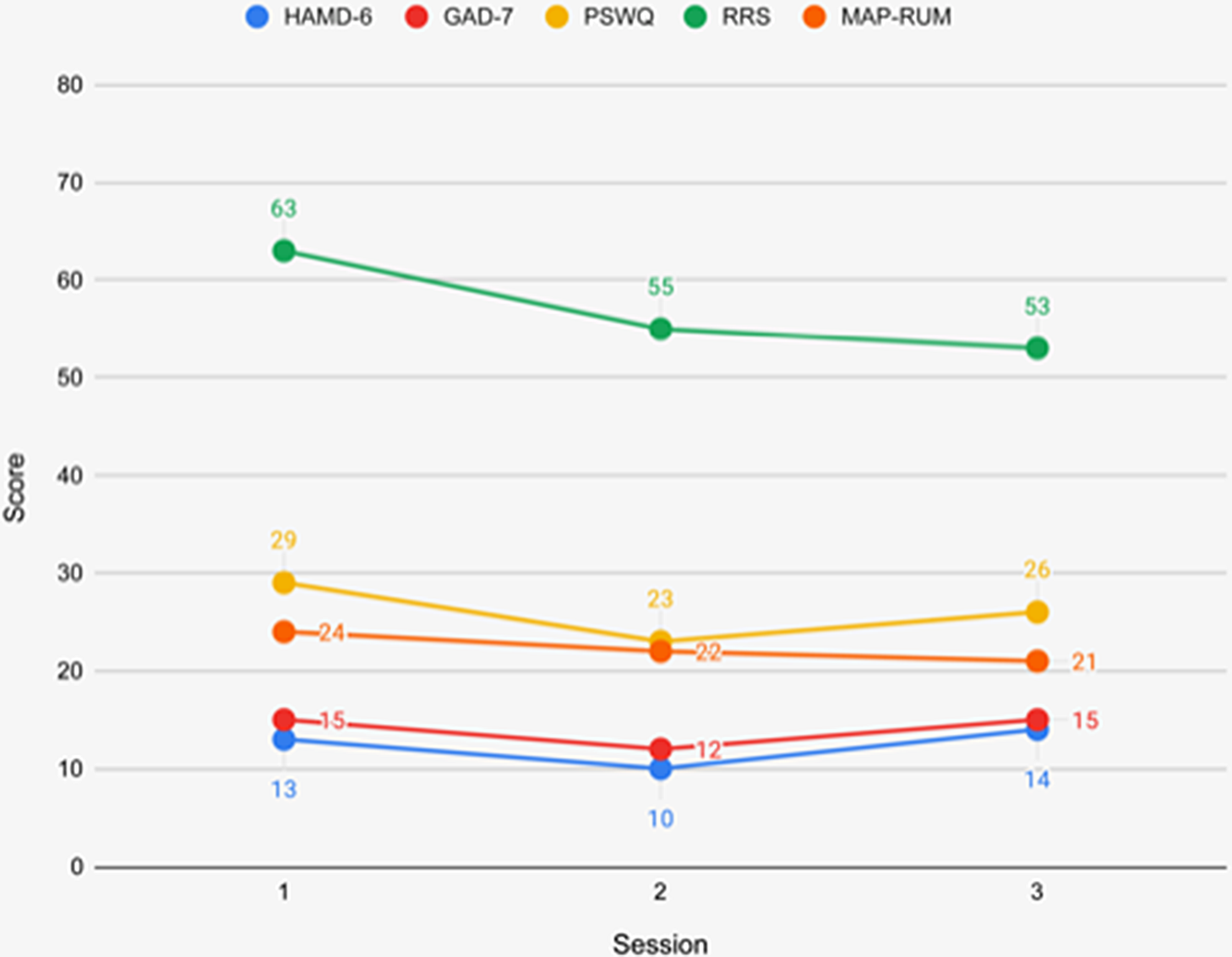
Figure 1. Self-report measurements for participant A.
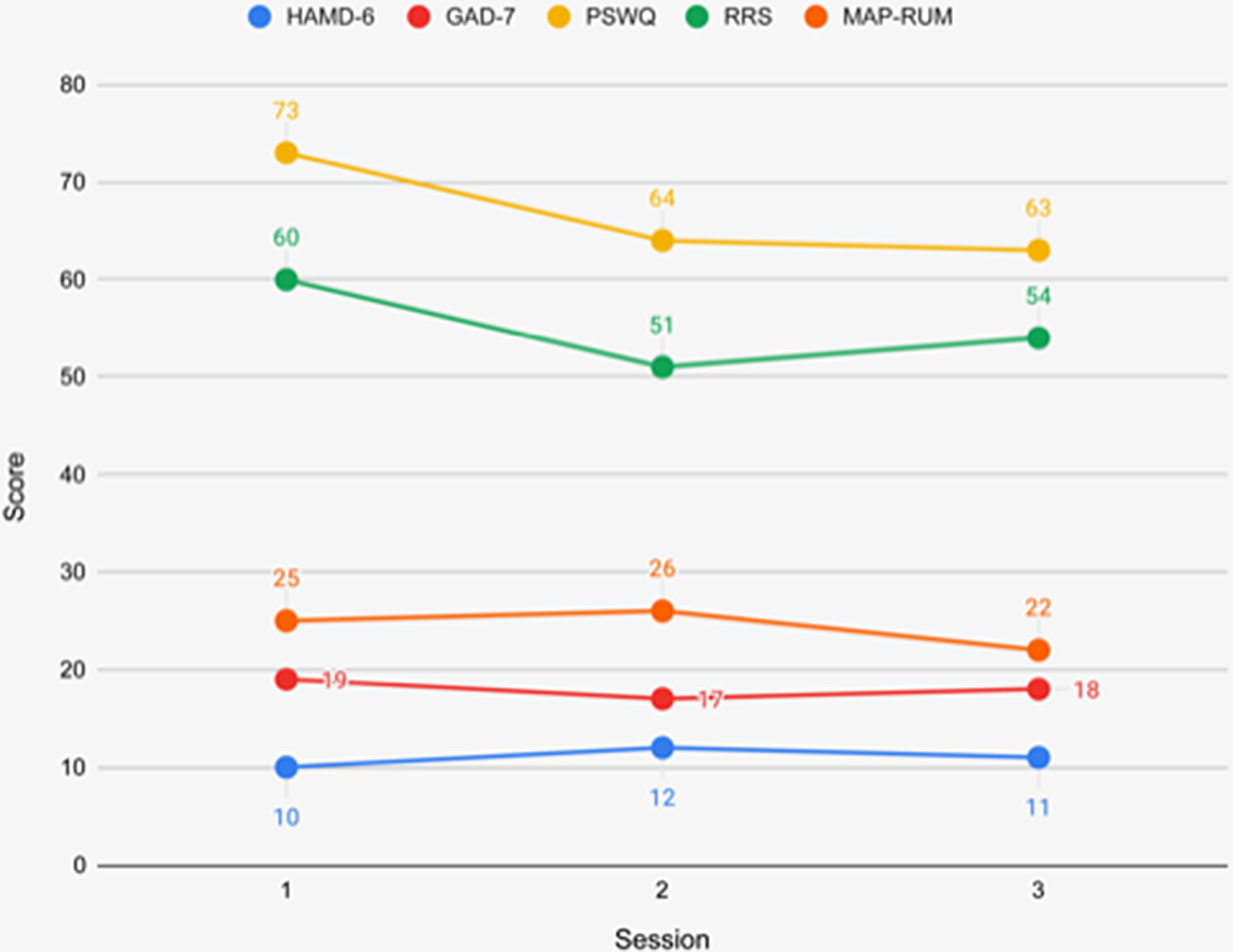
Figure 2. Self-report measurements for participant B.
At the first session, both participants had similar scores on rumination. On the RRS, the scores indicated a markedly ruminative response style to sadness or anxiousness, while scores on the MAP rumination subscale, averaging about 2.7 points per item for both participants, indicated a moderately high inclination for anger rumination. The latter is not surprising, given that irritability and anger are part of the PTSD syndrome. The PSWQ, however, showed a large discrepancy in the state worry for the two participants, with scores indicating low and high trait worry tendencies for participants A and B, respectively.
The depression and anxiety scores seemed to fluctuate only slightly across the three measurement time points. It is, however, worth noting that scores on the RRS and the MAP rumination subscale for both participants, and on the PSWQ for participant B, were markedly lower at the third measurement point.
Tracking data
Adherence to tracking was high, with both participants remembering to wear and use the tracker during every waking hour during the project period, except for one day (participant A; day 15) and half a day (participant B; day 10). Additionally, participant B forgot the daily mood registration a few days in the beginning and end of the project period.
An overview of the number of days and observations made with the tracker is shown in Table 1, and the observations are seen in Figs 3 and 4. Participant B had a higher frequency of observations than those of participant A which remained at approximately the same level during the two periods of tracking, with 108 (first period) and 91 observations (second period), giving an indication of high adherence and consistency in tracking (as explained in the Method section).

Figure 3. Overview of observations for participant A.
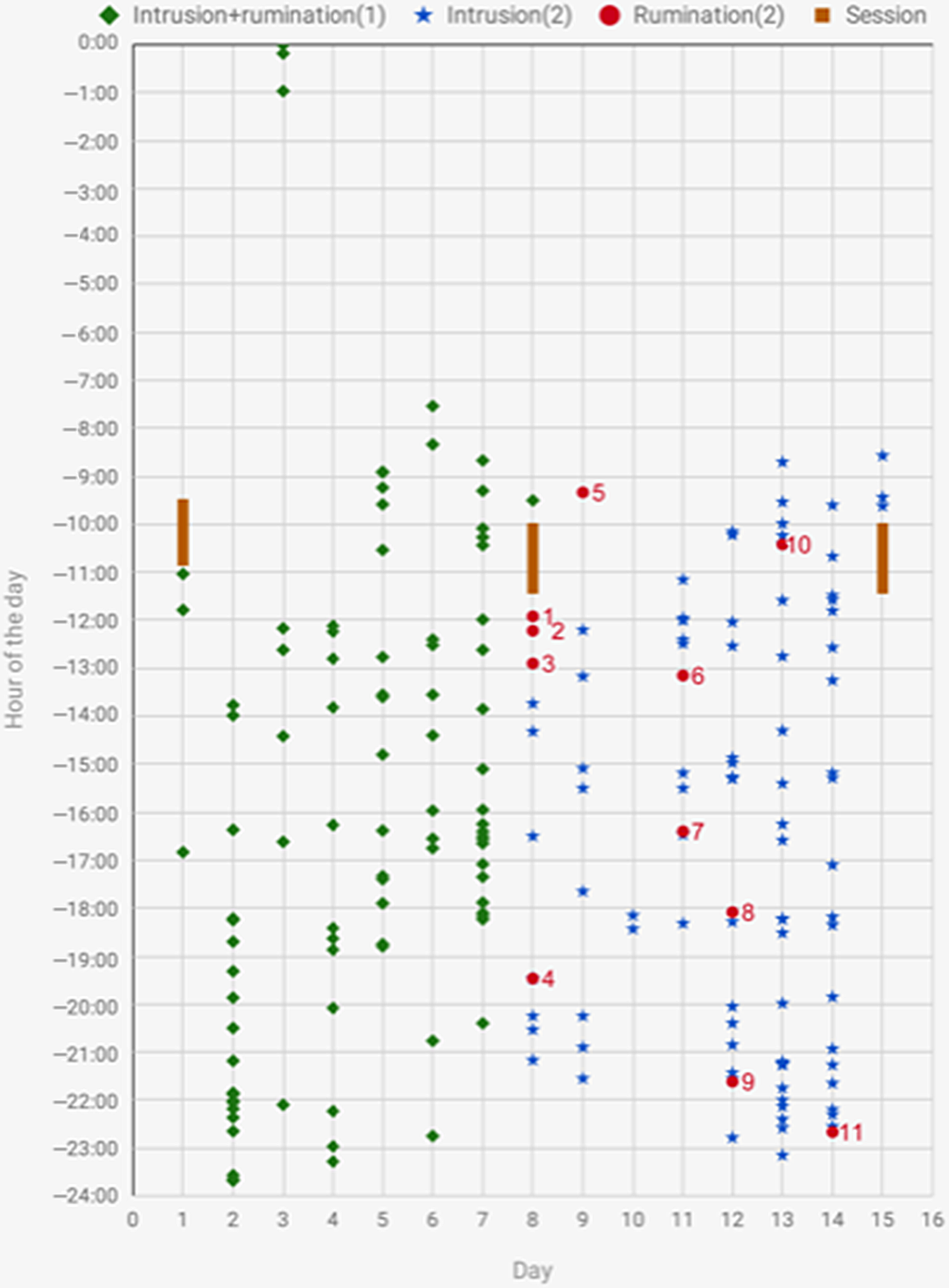
Figure 4. Overview of observations for participant B.
As can be seen in Table 1, participant A had considerably fewer observations during the second period of tracking, even when taking into account the longer duration of the first period (10 versus 7 days with 52 observations versus 18 observations). However, according to her, this was caused by a change in medications from sertraline-hydrochloride to vortioxetine on day 11 of tracking, which partially relieved the emotional numbing caused by sertraline-hydrochloride. The participant reported having a more unstable mood in the second period of tracking, along with experiencing side-effects leading her to sleep substantially more and therefore experience fewer occurrences of intrusions and rumination. Unfortunately, this prevents using the established baseline of intrusion and rumination frequencies as a proximate indicator of degree of adherence to tracking for participant A.
Differentiating between short and long button presses
The idiosyncratic cut-offs between a long and a short button press on the self-tracking instrument were established as 500 ms for both participants, with a short button press (below 500 ms) indicating an observation of an intrusion incident, and a long button press (above 500 ms) indicating an observation of a rumination incident. A clear temporal distinction was seen between long and short presses.
Patterns of the observed phenomena
The observations of the phenomena can be seen in Figs 3, 4, and 5. As Fig. 3 shows, the observations for participant A in the second tracking period were too scarce to conjure a clear pattern of the relationship between intrusions and ruminations. However, it should be noted that the observations of rumination were all preceded by intrusions. Markedly, on the last day of tracking, the participant registered an intrusion incident immediately followed by a rumination incident (7 s apart). In the other two instances, there was about 2 h from the intrusion to the rumination, and an incident of intrusions followed 54 min after the first rumination incident.

Figure 5. Overview of the temporal relation between rumination and intrusion incidents for participant B.
For participant B, Fig. 5 gives an overview of the temporal relationship between intrusions and rumination. In situations 4, 6, 9, 10, and 11, incidents of intrusions precede ruminations, while in situations 7 and 8, rumination clearly precedes intrusions. Situation 3 consists of three observations of rumination within the hours after a research session (see Fig. 4), concluding in an intrusion incident. This is consistent with the participant’s own report that she became emotionally affected after being confronted with her condition and its consequences as a part of the talks and evaluations in the sessions. Additionally, the bi-directional occurrences of intrusions and ruminations in situations 4 and 7 show how the phenomena may reciprocally follow each other.
In the scores of mood for participant B (see Fig. 7), two of the days with a high frequency of ruminations (days 8 and 11) were also days with particularly low mood. For participant A (Fig. 6), a possible relationship between mood and the occurrence and frequency of either intrusions or rumination was obscured by the uniform mood reports on days 1–13, reflecting a subjective feeling of numbness caused by the first type of anti-depressant which she switched from on day 11.

Figure 6. Mood scores for participant A.
Qualitative data
From the de-briefing interviews, the following themes emerged:
Theme 1: Distinguishing between rumination and intrusion
Both participants reported that they were clearly and meaningfully able to distinguish between ruminations and intrusions in their subjective, phenomenological experience as the phenomena unfolded. Participant B experienced differences in duration, with intrusions being briefer, and in the sudden occurrence and uncontrollability of intrusions, while rumination was perceived as more self-initiated and -maintained. By registering the phenomena, both participants obtained insight into their differential occurrences, e.g. in relation to certain triggers and in different contexts or times of the day. For instance, participant B realized that while her avoidance behaviour mostly consisted of avoidance of being at home (as the trauma had occurred at home, and this was where most ruminations took place), intrusions mostly occurred outside of the home, triggered by uncontrollable stimuli.
Theme 2: Rumination in the context of PTSD
A differential function of the two phenomena emerged. Participant A discovered that while intrusions came out of the blue and felt outside of her control, conversely she felt she had purposefully and successfully avoided thinking about the trauma and consequently had had the impression that she never ruminated. After receiving psychoeducation about rumination and intrusions and having raised her awareness of rumination, however, she had realized that she did in fact ruminate on three occasions during the second week. Over the course of the project period, it became clear to her that her efforts to avoid thoughts about the trauma disguised a form of emotional and cognitive avoidance which was keeping her from processing the trauma more effectively. When asked about how intrusions affected rumination and vice versa, she reported that intrusions lead to rumination in all but one instance (which was confirmed in the tracking data, see above).
Participant B experienced that intrusions would always come first and that the content of ruminations were often related to the intrusions, e.g. ruminating about ‘why do I have to experience this?’.
Theme 3: Effects and advantages of using the One Button Tracker
Participant A found that tracking in real-time gave her a clear sense of the internal phenomenology of the phenomena, which she previously had only theoretical knowledge about. The realization that her avoidant behaviour towards thoughts about the trauma was problematic made this clear to her as a possible theme to be addressed in psychotherapy which she had been referred to commence shortly. Having collected the data herself, participant A experienced a sense of ownership as it provided an acceptable and approximately objective depiction of her condition. The sense of ownership made it possible for her to surpass her self-reported ‘resistance’ or avoidance of engaging in trauma-related experiences, in turn adding to her motivation for engaging in psychotherapeutic treatment.
Furthermore, the accessibility of the instrument and the possibility of making observations in a matter of a seconds made it possible for participant A to register intrusions and rumination even in emotionally high-charged states. Additionally, she experienced an unexpected therapeutic effect of the tracking itself right in the moment when it occurred: when having intrusions, she would often feel that her body ‘froze’ and she could hardly move, let alone get out of the situation by moving away physically. However, surprisingly to herself, it turned out that she was still able to press the button on the instrument. This gave her a sense of being able to distance herself from the phenomenon, to somehow externalize it and retain a sense of agency in an otherwise seemingly uncontrollable situation.
When presented with her tracking data, participant B was surprised by the high number of data points. This showed to her that her condition was more severe than she had previously realized, and gave her an understanding of the extent to which it had affected her life, leading to a more self-compassionate approach towards herself as someone who was trying to do her best in a difficult situation. In relation to tracking with the instrument, as opposed to other forms of registering, she found an advantage in its accessibility, both in terms of physical, but also psychological proximity. The instrument allowed her to track the phenomena while proceeding in her current activity with minimal interruption, adding to the validity of data both in terms of adherence and recall bias.
Theme 4: Negative effects of using the instrument
Participant B found that her PTSD symptoms had exacerbated somewhat with the additional attention given to her condition during the project period. However, it was not clear whether the cause was the tracking itself, or the concurrent assessments for intake into psychiatric treatments. She found a temporary exacerbation acceptable as she considered it a necessary part of the healing process.
Both participants noted that the visibility of the instrument, when worn in a wristband, could prompt other people to ask questions about it. Participant A resolved this issue by wearing the instrument in a string around the neck. For participant B, the instrument was experienced positively as a conversation starter, providing a possibility to share her experiences and feelings openly with others, which provided her with emotional relief and a sense of relational proximity.
Discussion
As the qualitative data of this study indicate, it seemed possible for both participants to adequately notice, subjectively distinguish and register rumination and intrusions as two distinct phenomena using the One Button Tracker. Furthermore, it was seen how intrusions and rumination can have differing effects and functionalities for PTSD patients in their everyday lives. Finally, the study demonstrated how the tracking instrument provides data which makes it possible to investigate the psychological phenomena further with high data resolution, elimination of recall bias and possibilities for good adherence. This could aid with the development of both theory and treatment regarding the phenomena in the future.
Thus, this suggests support for the study’s two hypotheses: (a) rumination and intrusions appear subjectively as distinct phenomena when experienced by PTSD patients and (b) rumination and intrusions can be assessed separately in daily living using a wearable self-tracking instrument in a way which provides potential to further investigate the temporal relations between the phenomena. In addition, the participant perspective uncovered in the de-briefing interviews revealed future prospects for the instrument’s utility in research and clinical treatment centred on intrusions and rumination.
High-resolution, real-life tracking
The study utilized an innovative method with which rumination and intrusions were investigated with fine-grained temporal accuracy, which enabled a demonstration of how temporal relationships could be investigated. It also provided high validity of data: the tracking regime made it possible to educate the participants in differentiating between two phenomena via subjective experience, tested and tried in real life, rather than only theoretically. Finally, adherence was deemed as high, possibly due to the simplicity of use which makes it potentially useful also for participants with less personal capability and motivation for following more extensive self-observation regimes. The study thus demonstrates the potential in this method for further exploring the relationship between ruminations and intrusions in PTSD, which could refine both psychological theory and treatment in the future.
According to the interview data, tracking with the One Button Tracker seemed to provide a heightened degree of data validity with the elimination of recall bias as well as maximization of motivation and adherence to the registering regime. Furthermore, the simplicity of registering the phenomena right as they occurred provided participant A with a heightened sense of agency due to the ability to act in an otherwise confined situation by pressing the button as an intrusion occurred. Finally, the self-collection of data made it possible to mentally surpass an otherwise prevailing tendency to avoid confrontation with her symptoms and condition.
The self-tracking method offers a simplicity of use that seems to add to the completeness, quality, and usefulness of data. As demonstrated in the study, letting the data collection be driven by the phenomena’s occurrences, while registering the observation with an instrument requiring a minimum of effort, might improve adherence. This was both because the participant was able to adhere even when experiencing severe symptoms, and possibly also because the registration was prompted by an internal rather than an external factor, leading to higher engagement and agency. Furthermore, this approach secured the highest possible temporal resolution of data. As fine-grained data are essential for detection of precise relationships between the phenomena, the self-tracking method shows promise as an alternative method to data obtained from fixed or randomly prompted cues for registration used in most EMA methods, or more traditional post-hoc verbal or written reporting. However, further studies are needed comparing this method directly with other methods in order to establish possible advantages and disadvantages more definitely.
Theoretical considerations
The interviews reveal that the distinction between intrusions and rumination was experienced clearly and that both phenomena made sense to the participants in the context of their disorder. Participant A reported to attempt to push thoughts about the trauma out of her mind, initially thinking this worked well for her, but it revealed itself as a rather unsuccessful strategy as she had high scores on the RRS and MAP-RUM and did report rumination with the tracker during the study. This lends support to the general finding of avoidance as a maladaptive strategy. More specifically, it supports the necessity of processing trauma material, including triggers of negative thought, in an emotionally more adaptive way, which participant A also came to realize using the tracker method. Especially for participant B, a pattern of a temporal relationship between ruminations and intrusions emerged. Intrusions most often occurred first, suggesting that, in line with current theory (see the section Rumination in PTSD ), rumination could serve the function of a coping mechanism and/or a form of avoidance behaviour to the negative emotions experienced in connection with intrusions. Interestingly, participant B did not subjectively experience the reverse, that ruminations could lead to intrusions, although the data show that in some instances there was a connection in time with rumination being followed by intrusions. A tentative explanation for this could be that in her subjective experience, an intrusion was experienced as a sudden interruption to an activity or trail of thought, giving way to a new cascade of rumination, perhaps with different content related to the content of the intrusion. Also, the incoherence between her report and the data highlights the usefulness of a more temporally fine-grained registration of the phenomena of interest than post-hoc self-report. On that note, as seen in Fig. 7 (days 8 and 11), an intricate relationship between mood, rumination and intrusions could exist – here, rumination could tentatively be seen to co-occur with low mood, in line with earlier work finding that low mood induced by rumination may pave the way for (more) intrusions because intrusions are activated by negative mood (Ball and Brewin, Reference Ball and Brewin2012; Brown et al., Reference Brown, Hetzel-Riggin, Mitchell and Bruce2018; Michael et al., Reference Michael, Halligan, Clark and Ehlers2007; Newby and Moulds, Reference Newby and Moulds2012; Smets et al., Reference Smets, Luyckx, Wessel and Raes2012).
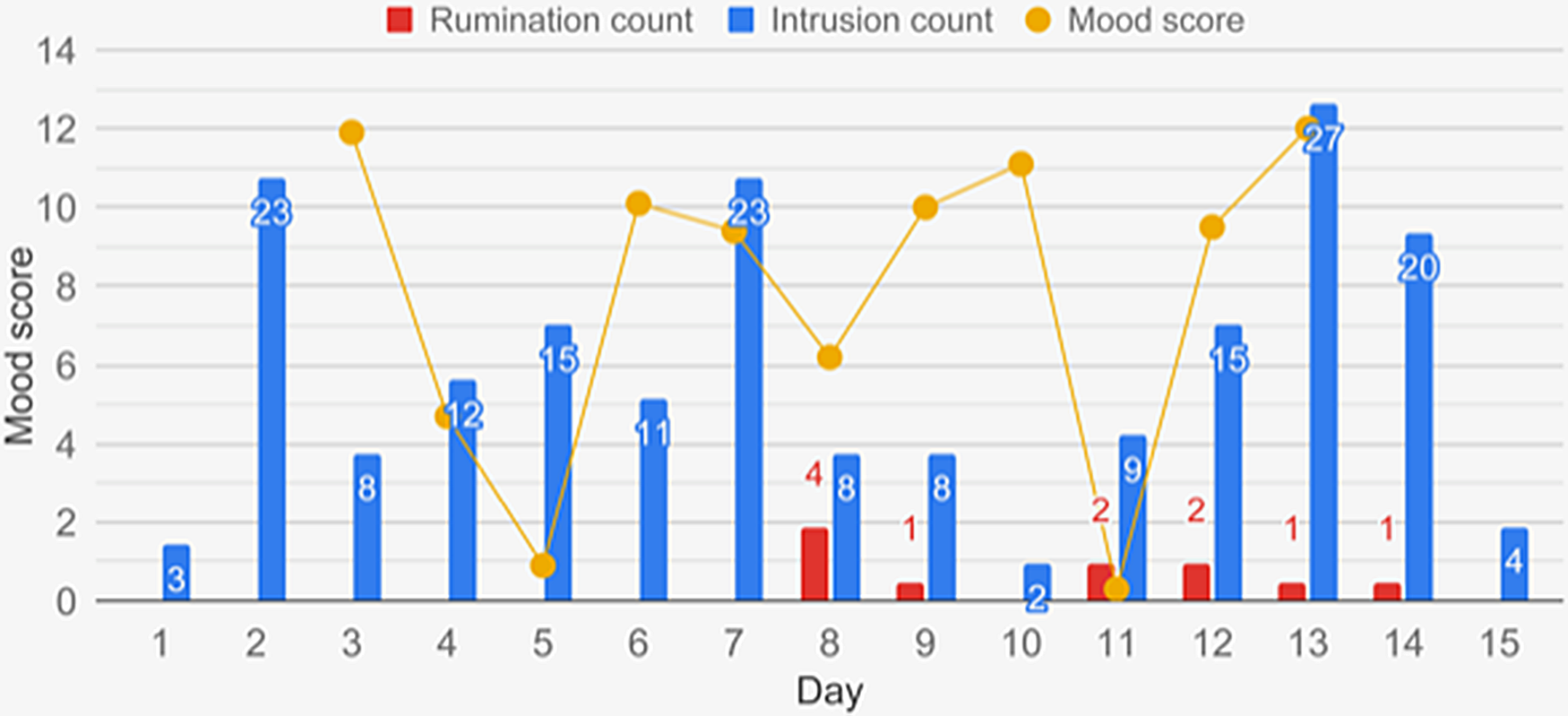
Figure 7. Mood scores for participant B.
Clinical perspectives
The clinical perspectives of the results in the study are promising. The knowledge and heightened awareness obtained in the process of tracking provided the participants with new insights about the differential function, occurrence, and impact of rumination and intrusions. Furthermore, the decline in rumination scores for both participants, and worry scores for participant B, hints that enhanced knowledge and awareness about rumination in itself can be therapeutic, providing improvement even before an explicit therapeutic intervention took place. The levels of depression and anxiety did not change simultaneously. It could therefore be speculated that the awareness and change in rumination behaviour precede change in psychiatric symptoms, although this would need further investigation in studies of a larger scale.
Also, the concreteness of self-experience and -collection of data aids in moving away from the maladaptive abstractness of ruminative thinking. The data would be directly and easily available for visual inspection and use in therapeutic sessions and for monitoring treatment progress or decline. Further prospects for treatment include linking tracking to tailored interventions, e.g. methods for disengaging from rumination, which are applied in the moment and subsequently registered on the instrument. The real-time self-tracking thus provides a link from what goes on in the therapy session directly to the lived life as it unfolds for the individual.
Limitations
Limitations to the study include the initial self-reported low levels of rumination for participant A, and that her mood reports and frequency of symptoms were affected by a change in medication during the study, as this makes comparisons between periods 1 and 2 less informative and obscures a possible detection of relevant associations. Participant A was therefore not an ideal candidate for a proof-of-concept case study such as the current one regarding the aims of investigating the occurrence of rumination in PTSD and the temporal relationship between rumination and intrusions. However, while participant A had low trait rumination as shown on the PSWQ, she did indeed have similar scores to participant B on the RRS and the MAP-RUM, indicating a tendency to ruminate in response to negative feelings. Furthermore, she reported three incidences of rumination in the second week, indicating that psychoeducation and more awareness of rumination changed her former perception of not ruminating. As such, her data was included here, as they provided some interesting information about the latent or unrecognized occurrence of rumination even in people who think they do not ruminate.
Participant B had only registered her mood for part of the project period. The scarcity of data points and confounding of mood scores therefore did not make it possible to establish a conclusive pattern between intrusions, mood, and ruminations. Also, mood was registered as a daily average; a more fine-grained temporal registration might have been able to reveal more accurate temporal relations between mood, ruminations, and/or intrusions. However, for the sake of simplicity, and as the main focus was on rumination and intrusions, registration with the One Button Tracker was here restricted to these two phenomena. Also, this was done on the grounds of previous work during the development of this method, where patients with a high and complex symptom load expressed preferring focus on the fewest possible phenomena when self-tracking.
Another limitation is the lack of a theoretically and clinically determined cut-off for how close the temporal proximity between the phenomena should be in order to classify them as being connected. For the purpose of this study, a rather lenient cut-off of 1 h was chosen. However, this should clearly be investigated further in order to establish an evidence-informed cut-off for use in future studies.
Also, registering psychological phenomena in situ with an instrument such as the one used in this study will likely be most accurate when a clearly distinguishable phenomenon presents itself to the individual in a manner that enables immediate, conscious observation of its initiation, and for phenomena of longer duration, also its termination. An intrusion is one such phenomenon due to the nature of its sudden appearance, short duration, and subsequent momentary registration. Meanwhile, rumination may evolve more gradually over time in an ongoing trail of thought and therefore may be harder to consciously notice and register in the moment it first starts to occur, and when it subsequently vanishes. Addressing the former, it was deemed sufficiently valid if the participants registered rumination as soon as they noticed it, thus retaining the possibility to detect a form of temporal order between psychological phenomena with reduced recall bias, even if rumination or other less distinct phenomena may be easier to clearly identify in retrospect. The termination of a rumination was not registered in this study, and the resulting lack of knowledge of the duration of a rumination makes it difficult to establish a direct or causal relationship between rumination and intrusions via inspection of the quantitative data only. However, such a registration could have interfered with the usual unfolding of a trail of rumination, thus compromising validity of data. As definite knowledge of the duration of a rumination is lacking, combining the quantitative and qualitative data currently provides more valid, if not yet exhaustive, insight into the relationship between the two phenomena.
Having said this, it must also be stressed that rumination and intrusions in their natural occurrence may present more muddled, as occurring in brief succession, even non-categorizable. The psychoeducation in the distinction between the phenomena attempted to couple the participants’ experiences in the first week of registering with theoretical knowledge as described in the Introduction. However, the phenomenological distinction between rumination and intrusions necessarily remains subjective.
A further limitation is the lack of a self-report measure specifically investigating rumination about the trauma and its consequences. Including such a measure would have been highly relevant to further enlighten the nature of rumination in PTSD. However, no such instrument seems to have been developed and sufficiently validated up to this date (Moulds et al., Reference Moulds, Bisby, Wild and Bryant2020). When available, it should be included in similar studies in the future.
Obviously, a case study such as the current one does not provide solid evidence, making it possible to generalize to a larger population of PTSD participants. The selection of participants for the study was not representative, seeing that both were young women, were recruited on the grounds of high motivation, and that the participants were particularly cognitively high functioning. While a certain degree of motivation is a pre-requisite for participating in a research project, the results from this project should be investigated further in a more diverse sample. Particularly, cognitive deficits will present a challenge for a large proportion of PTSD patients, and it should be explored further to what extent this will interfere with the adherence and quality of data for research and treatment purposes. Also, the quantitative evidence in the form of tracking data and self-report measures can only be interpreted with a great deal of tentativity due to lack of power.
Conclusion
Given the prominence of rumination in PTSD and its relation to the core PTSD symptom of intrusions, rumination is an important, distinct treatment target in psychotherapy for PTSD. In this study, both quantitative and qualitative data were collected, together providing interesting information about the occurrence of intrusions and rumination in PTSD patients and the effects and experiences when registering them.
The role of rumination in relation to intrusions in PTSD still needs to be investigated further in clinical studies on a larger scale. This study demonstrated the possibilities in investigating rumination and its relation to intrusions and possibly other psychological phenomena, using novel instrumentation for real-time registering of their occurrences. This could prove for future insights and improvements for both research in the field, for adaptations and selections of psychotherapy methods, and directly for the participants tracking symptoms or other psychological phenomena.
Acknowledgements
The authors would like to thank the two participants who with their generosity, in terms of both time and effort, made this study possible. Furthermore, a huge thanks to PhD student, MSc Psychology, Frederik Bernt Scharff for his assistance in recruiting participants.
Financial support
This work was supported by the Council of the Danish Victims Fund (Offerfonden; I.-M.T.P.A., S.B.M. and L.H.G.R.; grant number 18-610-00018) in the role of funder of the larger research project which provided participants for the current study. The development of the One Button Tracker and its clinical feasibility testing was funded in part by the Technical University of Denmark and Innovation Fund Denmark (J.E.L. and T.B.C.; grant number 9122-00121B). The funding sources only provided financial support and had no involvement in the content of the study or the study article.
Conflicts of interest
The One Button Tracker used in the study was invented and developed by the authors J.E.L. and T.B.C.
Ethical statement
The authors have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. The current study was submitted for approval by the Danish National Committee on Health Research Ethics (journal no. H-19008326), who deemed that as the study was a methodological study rather than an intervention study, it did not need further approval from the Committee to be carried out. Participants gave written and verbal informed consent separately to the two studies. They could withdraw consent at any time and were informed that this would not affect their treatment at the MHS-CRD.
Data availability statement
The data that support the findings of this study are available from the corresponding author, I.-M.T.P.A., upon reasonable request.
Supplementary material
To view supplementary material for this article, please visit: https://doi.org/10.1017/S1754470X2100012X
Key practice points
-
(1) Self-tracking of psychological phenomena with a One Button Tracker is a valuable source of information for both client and clinician.
-
(2) Tracking in real-time can possibly provide more accurate and detailed information than traditional CBT registration methods.
-
(3) The One Button Tracker could possibly improve adherence to registration of psychological phenomena due to its accessibility and ease of use for the client.
-
(4) Tracking in daily life can itself provide benefits beyond insight in the occurrence of a phenomenon.











Comments
No Comments have been published for this article.