


Introduction
This article examines definitions of elder mistreatment (covering abuse and neglect) in policy debates and documents and in research in the light of a major study of elder mistreatment, the United Kingdom (UK) Study of Abuse and Neglect of Older People. This was commissioned by the charity Comic Relief with co-funding from the Department of Health and conducted by a team from the National Centre for Social Research and from King's College London. The study included a national prevalence survey (O' Keefe et al. Reference O'Keefe, Hills, Doyle, McCreadie, Scholes, Constantine, Tinker, Manthorpe, Biggs and Erens2007) and a follow-up qualitative study involving in-depth interviews (Mowlam et al. Reference Mowlam, Tennant, Dixon and McCreadie2007). It was the first survey of elder mistreatment to include a qualitative follow-up, which enabled researchers to move beyond the prevalence figures and conduct a fuller exploration of respondents' experiences and understandings. This article draws primarily upon findings from the follow-up qualitative research. The study was informed by an advisory group with representatives from various stakeholder organisations and by an older people's reference group of people with relevant personal experiences.
Definitions of elder abuse and mistreatment
The definition of terms has long been contentious in the study of elder mistreatment (Bonnie and Wallace Reference Bonnie and Wallace2003; Brammer and Biggs Reference Brammer and Biggs1998; Lachs and Pillemer Reference Lachs and Pillemer2004; Penhale Reference Penhale2003). An early challenge for the study was to agree operational definitions. The research team sought to reflect current thinking, to identify the current consensus (if any), and to maximise comparability with previous surveys. We began by focusing on two widely accepted policy definitions, the first being the early and influential definition of ‘the abuse of vulnerable adults’ in British governments' guidance documents, No Secrets (Department of Health 2000) and In Safe Hands (National Assembly of Wales 2000). Drawing on a civil rights approach, this definition specifies abuse as ‘a violation of an individual's human and civil rights by any other person or persons’ (Department of Health 2000: section 2.5). It states that:
Abuse may consist of a single act or repeated acts. It may be physical, verbal or psychological, it may be an act of neglect or an omission to act or it may occur when a vulnerable person is persuaded to enter into a financial or sexual transaction to which he or she has not consented or cannot consent. Abuse can occur in any relationship and may result in significant harm to, or exploitation of, the person subjected to it.
The definition includes ‘discriminatory abuse, including racist, sexist, that based on a person's disability and other forms of harassment, slurs or similar treatment’ (section 2.7). The research team decided that this definition is too broad, since it includes all forms of harm and discrimination. The second considered definition was that developed by the charity Action on Elder Abuse and subsequently adopted by the World Health Organization and the International Network for the Prevention of Elder Abuse (hereafter the AEA/WHO definition). It is a narrower definition of elder abuse as ‘a single or repeated act or lack of appropriate action, occurring within any relationship where there is an expectation of trust, which causes harm or distress to an older person’ (World Health Organization and the International Network for the Prevention of Elder Abuse 2002, our emphasis). It was considered a more appropriate and workable definition for the survey.
The research team also reviewed the definitions used in previous surveys of the prevalence of elder mistreatment, as in Boston, Massachusetts (Pillemer and Finkelhor Reference Finkelhor, Pillemer, Hotaling, Finkelhor, Kirkpatrick and Strauss1988), Canada (Podnieks et al. Reference Podnieks, Pillemer, Shillington and Frizzel1990), Britain (Ogg and Bennett Reference Ogg and Bennett1992), and Amsterdam (Comjis et al. Reference Comjis, Pot, Smit, Bouter and Jonker1998). Each of these surveys took a different approach to defining mistreatment. For example, the Boston study did not include financial abuse, while the British study did not cover neglect (and none included sexual abuse). The designs of the survey questions also varied, e.g. whether single or multiple questions were used to identify different types of mistreatment. Most specified a narrow range of perpetrators, typically family members and paid care workers, effectively excluding the possibility of mistreatment by friends, neighbours, acquaintances and strangers, even though close friends have been recognised as in relationships that engender an expectation of trust (McCreadie Reference McCreadie2007). The age ranges that designate elder abuse also varied, with the Boston and Canadian studies specifying people aged 65 or more years, the British study people aged 60 or more years, and the Amsterdam study people aged 65–84 years. There were also differences in sampling strategies and in the interview mode – telephone interviews were conducted in Boston and Canada, and face-to-face interviews in Britain and Amsterdam. The prevalence estimates in these studies varied from 2.6 to 5.6 per cent.
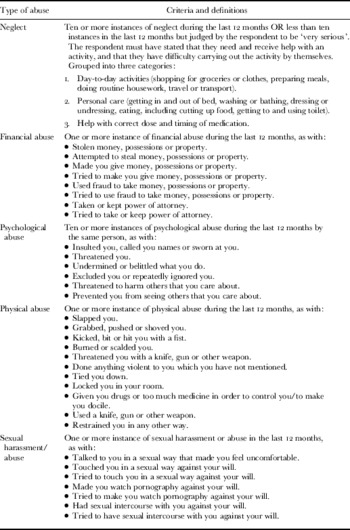
Despite these variations, a definition that is comparable on some dimensions with the earlier studies was possible. From the AEA/WHO definition, it was decided to focus on harms perpetrated in relationships deemed to create an expectation of trust, an attribute that is now widely accepted by researchers as central to the recognition of elder mistreatment (Bonnie and Wallace Reference Bonnie and Wallace2003). In the UK study, this was captured by focusing on harms perpetrated by family members, close friends and paid workers (including doctors, nurses, social workers, mental health nurses, community nurses, health visitors, home helps/home-care staff, sheltered housing wardens and unspecified paid or voluntary-sector care workers). The survey also adopted specific definitions of abusive behaviour, with frequency thresholds where relevant, that drew upon those used in earlier surveys and best practice approaches in research on family violence (O'Keefe et al. Reference O'Keefe, Hills, Doyle, McCreadie, Scholes, Constantine, Tinker, Manthorpe, Biggs and Erens2007: 18). These covered physical, psychological, financial and sexual abuse and neglect (see Table 1). Although not included in the main prevalence estimates, the survey also collected and reported data about mistreatment perpetrated by neighbours, acquaintances and strangers.
Table 1. Behavioural definitions used in the survey for the UK Study of Abuse and Neglect of Older People
The follow-up qualitative research
The main survey conducted face-to-face interviews with a random sample of 2,111 people aged 65 or more years. The follow-up qualitative study conducted semi-structured interviews with 42 respondents, including 36 respondents to the main survey who had reported mistreatment that were purposively sampled to be representative of the national distributions by gender, age, ethnic group, constituent UK countries, living arrangements (alone or with others), types of mistreatment and perpetrators. Given the limitations of the main survey sample, the qualitative sample was augmented with three respondents who were recruited through community-based, black or minority-ethnic older people's organisations. Three interviews were also conducted with family members who had provided respondents with support at the time of the mistreatment. A sample of this size is usual for a qualitative study and allows issues to be explored in sufficient depth for meaningful analysis (Bryman Reference Bryman2008; Ritchie and Lewis Reference Ritchie and Lewis2002).
The qualitative interviews lasted between 60 and 90 minutes, and were carried out at the respondents' homes using a topic guide that was developed in consultation with the funders and study advisors. This ensured systematic coverage of key topics but was used flexibly so that the respondents could focus on the issues they found most relevant and discuss them in their own words. The interviews explored experiences of mistreatment, feelings and reactions, coping, reports of mistreatment and impacts. They were transcribed verbatim and analysed using Framework, a tool for analysing qualitative data (Ritchie and Lewis Reference Ritchie and Lewis2003). The final sample reflected well diverse types of mistreatment and respondents (Table 2), but certain groups were under-represented, including people from Northern Ireland, those aged 85 or more years, and people from black or minority-ethnic backgrounds. The survey did not include respondents with cognitive impairments, and it is likely that the sample under-represented the most vulnerable older people, including those unable to take part because of illness (Biggs et al. Reference Biggs, McCreadie, Manthorpe, Tinker, Hills, Doyle and Erens2008). Consequently, the findings from the qualitative research, though otherwise robust, may not reflect the experiences of these groups.
Table 2. Characteristics of the qualitative sample

Note: ‘Target’ was the minimum target sample size.
The analysis
The initial stage of analysis was familiarisation with the interview transcripts, which informed the development of thematic matrices or ‘charts’ that comprehensively summarised the data. References back to the full transcript enabled points to be explored in more detail and pertinent quotations to be identified. There was a chart for each broad topic: its columns represented specific themes, and each row referred to one respondent. This device makes the interview data more accessible and facilitates comprehensive and consistent analysis, while at the same time ensuring that links with the verbatim data are retained. It allows for in-depth within-case analysis as well as for case comparisons, and for patterns and analytical themes to be identified and explored systematically and in depth. A full account of the substantive findings from the qualitative research, and more details about the methodology, have been published in Mowlam et al. (Reference Mowlam, Tennant, Dixon and McCreadie2007). This article draws upon the in-depth interviews to explore the difficulties with and anomalies of definitions of elder mistreatment in large surveys, and how these influence our understanding of its prevalence and provenance. The discussion considers in sequence three key issues: the ‘expectation of trust’ concept and relationship categories, the scope and nature of behavioural definitions of abuse and neglect, and the use of chronological age.
Trust and relationship categories
As noted, the AEA/WHO defined elder mistreatment as occurring in relationships ‘where there is an expectation of trust’. This concept has been captured in previous prevalence surveys by using ‘relationship categories’, primarily it appears to distinguish harms committed by family members from those perpetrated by paid care staff. The UK national survey additionally distinguished harms committed by close friends. In this way, mistreatment associated with specific relationships was distinguished from wider social harms, discrimination, and harm inflicted by people not known to the older person. An important finding of the supplementary qualitative research, however, was that the interviewees identified various problems with the use of ‘in a relationship of trust’ to limit the scope of recognised elder mistreatment. Both respondents and analysts had difficulties with the categorisation of people into relationship categories. The assumption that the identified relationship categories imply an expectation of trust did not always reflect older people's experiences – we believe the theoretical basis for the assumption is unclear. This has been reflected in many survey instruments, which make no distinction between trust in affective relationships and the idea of ‘a position of trust’. Trust also appeared to be a matter of degree and context-dependent, rather than simply present or absent (i.e. it was not dualistic) as most definitions of elder mistreatment imply.
Classifying individuals into relationship categories
There were various examples in the in-depth informants' accounts of perpetrators who were not readily assigned to a relationship category (the term perpetrator is used in this article although strictly they were alleged perpetrators). One was recorded in the main survey as the respondent's partner, but during the qualitative interview the respondent referred to him alternately as a partner and a close friend, explaining that the relationship was not sexual, and in a related interview with a family member the same person was described as a lodger, because he had his own room and contributed towards household expenses. In another example, a perpetrator was categorised in the survey as an acquaintance, but this person, although not biologically related, was raised in the same household as the respondent's partner and was described by the respondent as ‘like family’. Some respondents were also uncertain or tentative about whether extended and reconstituted family members should be categorised as ‘family’. ‘Neighbour’ was also ambiguous, because respondents were not always clear whether the term referred to a next-door neighbour or someone living ‘nearby’. Some were unclear about the boundary between a neighbour and a friend. To exemplify, some respondents said that he or she and one or more neighbours had each other's door keys, helped each other and socialised together. In several cases, people described staying in touch with neighbours after they had moved to another area; in one case, they spoke on the telephone every day.
Others found it difficult to distinguish between an acquaintance and a friend. For example, one respondent met with the perpetrator of her mistreatment at a local club where they socialised with other friends and club members. In this case, the perpetrator was described in the main survey as an acquaintance, which the respondent confirmed during the qualitative interview: ‘He was just a casual acquaintance, we weren't personal friends’. In another instance of a perpetrator being cited as an acquaintance in the main survey, the respondent said, ‘Well, he was a friend in a way but after he did that to me I never spoke to him’. How should researchers respond to such ambivalence in the relationship categories and descriptions? One clear requirement is to expand the range of people who might perpetrate abuse. This could be done by collecting fuller information about the nature and frequency of emotional, sexual, domestic, financial and other contacts. Inevitably there would be disagreement about the appropriate inclusion and exclusion criteria. Given the immense variability of abuse, we argue that pre-designating the perpetrators is misguided and that open-ended inquiry should be employed.
Understandings and experiences of trust
The use of relationship categories to imply an expectation of trust in many cases did not reflect the respondents' experiences. The qualitative interviews revealed great diversity in the quality and nature of family relationships, and revealed that many respondents did not trust care workers or friends but did trust neighbours, some acquaintances and even strangers. To elucidate these findings, the research team turned to the theoretical literature on the expectation of trust in different types of relationship. We found several theoretical bases for the presumption, some connected to particular relationships, but that none were well developed or undisputed.
Trust in affective and family relationships
It is generally assumed that family members can be trusted more than others, and the presumption of an expectation of trust in family relationships is well established. Giddens (Reference Giddens1993: 295) asserted that ‘kinspeople can usually be relied upon to meet a range of obligations more or less regardless of whether they feel personally sympathetic towards the specific individuals involved’. Theoretical expositions posit that family members have a sense of similarity to each other and shared norms and values (Misztal Reference Misztal1996). Such views have been challenged, however, notably by feminist critics who point to the family as a site of potential conflict, exploitation and oppression (Okin Reference Okin1989), and by those who draw attention to the rivalries and rifts in families, as in those involved in crime or family businesses (Von Lampe and Johansen Reference Von Lampe and Johansen2003). In the specific context of elder mistreatment, Chappell et al. (Reference Chappell, Gee, McDonald and Stones2003) and Biggs and Powell (Reference Biggs and Powell2001) have pointed out that moral and normative ideas about trust in families conflict with the descriptions of ‘the family’ as a site of inter-generational stress, conflict and violence, as are common in accounts of elder mistreatment.
Rational choice theorists present an alternative argument for the presupposition of trust in family relationships, that dense inter-personal networks and frequent interactions among the members increase the information individuals have about each other, which creates the conditions for mutual trust. Hardin (Reference Hardin2002) thought this reasoning simplistic, however, and pointed out that whether frequent interactions increase trust depends on many factors, and argued that increased knowledge might generate greater mistrust. Cook, Hardin and Levi (Reference Cook, Hardin and Levi2005: 3) also examined the limits of intra-familial trust and argued that, ‘when the temptation to become untrustworthy is great we tend to think of other ways of ensuring the competence and motivation of those on whom we are taking a risk. … This is often true even in families’. Furthermore, as family networks in modern societies become more dispersed and the dissolution and reconstitution of families more common, the ‘thick’ connections that are thought to underlie familial relationships of trust may become less prevalent (Glaser et al. Reference Glaser, Stuchbury, Tomassini and Askham2008; Williams et al. Reference Williams, Stacey, Sawyer and Wahlstrom2005).
The in-depth interviews showed that most of the family members who were not trusted were distant relatives or those acquired through reconstituted families, but there were also examples of not trusting siblings, sons, daughters and grandchildren. In a few cases all contact had ended, sometimes following mistreatment, as in the case of a grandchild who repeatedly stole money from a respondent. Other respondents described their mistrust of family members who were not cited as perpetrators of mistreatment. For example, one respondent said that she thought her son only stayed in touch to ensure his inheritance, while another felt that her son and his children had not been grateful for the financial and other support that she had provided, and so she had stopped sending cheques at Christmas and birthdays. In other cases, respondents had not been in touch with relatives for many years following arguments and disagreements. Also anomalous were cases of abuse in which the perpetrator was dependent on the victim of the mistreatment or not fully responsible for their behaviour. Such situations create ambiguity about the expected direction of the trust, i.e. who trusted who? The reported cases included spouses with dementia or mental illness, and a foster child with emotional and behavioural difficulties. The respondents in such cases tended to see themselves as being in a position of trust rather than having an expectation of trust in the ‘perpetrator’.
Positions of trust
The relationship with a care worker is professional rather than personal. It is based on contractual arrangements and governed by professional codes of conduct or practice, agency law, professional licensing boards and regulators, and a national scheme that vets who is permitted to work with vulnerable people (Stevens and Manthorpe Reference Stevens and Manthorpe2007). Theorists argue that such organisational and legal frameworks attempt to guarantee probity in formal care relationships and therefore create the basis for an expectation of trust (Cook, Hardin and Levi Reference Cook, Hardin and Levi2005; Hardin Reference Hardin2002). The key principle in these cases is the legal definition of a ‘position of trust’, which refers to anyone who has a duty of care towards another person, which includes not only professional carers but also family members, neighbours, friends and others who provide protection, care or a service or support for another person (Sentencing Guidelines Council 2004). The in-depth interviewees had many difficulties with the presumption that formal care staff are in ‘a position of trust’, and there was considerable variation in the degree to which they trusted care workers. Some described a high level of trust, and many said of workers that they saw regularly that they had come to know them well. In other cases, however, the respondents explicitly described mistrust. One, for example, mentioned that she followed the home-care worker around the house to ensure that she did not steal anything.
Trust in friends, neighbours and acquaintances
While there are literatures in sociology and social psychology on friendship, neighbouring and acquaintances, no coherent account of trust in these relationships was identified. The in-depth interviews made it apparent that friendships vary greatly, as common experience suggests. The respondents described, for example, long-standing friendships that involved a high level of trust, others in which trust was provisional or partial, and some in which there was clear mistrust. Some ‘friendships’ were sustained mainly through proximity or shared activities, and some were described as unstable. In short, whether a person was considered a ‘close friend’ was highly subjective. On the other hand, some respondents placed considerable trust in people that conventional reasoning on elder mistreatment largely ignores and does not identify with an ‘expectation of trust’. In cases of doorstep fraud, the respondents had trusted strangers because they appeared ‘well presented’ and ‘respectable’. Many respondents also trusted people in the local community, for example, a respondent with mobility impairments talked about leaving her door unlatched so that the milkman and postman could let themselves in, only locking the door once it got dark. Respondents trusted their neighbours in various ways, as with their door keys and access to their homes while they were away. A period change was implied, in that the respondents reminisced of a time when they said it was common and accepted practice to trust neighbours and others in the local community, and doubted that this still applied.
The forms, degrees and conditionality of trust
That trust has different forms and levels and is context-dependent has been argued by many theorists. The consensus is that trust is rarely unconditional and that it is best represented as a multifaceted relationship, whereby a person is trusted in specific ways in specific circumstances (Cook, Hardin and Levi Reference Cook, Hardin and Levi2005; Hardin Reference Hardin2002; Luhmann Reference Luhmann and Luhmann1980). This concept of trust as multi-dimensional, fluid and modifiable is inconsistent with the dichotomisation of relationships into those with and without trust. The informants' comments without exception corroborated this representation: they did not regard trust as either present or absent but rather a quality that varied in strength and form. They described broad and comprehensive trust in some, and qualified trust in others. For example, when a respondent and her friend were sitting together in the car and about to drive away, the friend suddenly said she needed to use the bathroom before they left and the respondent gave her house keys to the friend so she could go back into the house. The friend let herself into the respondent's home during which time she was thought to have stolen money. The respondent had not let her have unsupervised access to her home at other times.
Several cases were reported of family and friends visiting but not being given door keys, and there were variable expectations and levels of tolerance of guests being unsupervised in other rooms. There was also considerable variability in the extent to which the respondents let family members get involved in their financial and legal affairs. Moreover, the respondents varied in the degree to which they confided in others about the mistreatment they had experienced. Some had confided in others, but in other cases the respondent did not tell friends or family about their mistreatment because they were not confident that they would respond in a helpful way. For example, one respondent said that she did not tell her son about her mistreatment because she thought he might assault the perpetrator and get himself arrested.
To sum up, a strong message emerged from the in-depth interviews with people who had direct experience of mistreatment and abuse: it is that the policy and practice discourses surrounding ‘elder abuse’ must acquire a more subtle and realistic understanding of the nature of trust and its role in vulnerable people's dealings with others. The theoretical underpinnings need to be developed and the rationale for an expectation of trust in different types of relationship needs to be specified. Its applications need to reflect older people's experiences, and a distinction should be made between trust in affective relationships and ‘positions of trust’. More generally, the relevance of trust in descriptions and explanations of elder mistreatment needs critical examination, with closer attention to how the relevance of the concept in distinguishing between elder mistreatment and other harms and difficulties. Particular attention also needs to be given to how and whether the concept can be effectively captured in survey research using relationship categories.
Definitions of abusive behaviour
The behavioural definitions used by the UK Study of Abuse and Neglect of Older People took the form of lists of specific behaviours based on both previous research, as on family violence, and the perceived consensus among opinion formers (Table 1). The in-depth interviews identified anomalies in the list, however, and there were indications that it is too inclusive and captures both incidents of mistreatment and what were regarded as different harms and inter-personal difficulties. Some named mistreatments were also open to misinterpretation, particularly in more complex situations and those resulting from service failures. The behaviours that were most unequivocally regarded as abusive were theft and fraud by care workers or family members, physical assaults and various forms of psychological mistreatment, such as being deliberately ignored by others in the household or repeatedly undermined and demeaned. These behaviours are manifestly relatively severe, or they affect people who are unusually vulnerable or dependent on the perpetrator. Some behaviour fitting this description was nonetheless not classified as mistreatment because of the relationship with the perpetrator, such as some cases of doorstep fraud or harassment by neighbours.
In other cases, however, the researchers sensed that they had heard only one side of a situation, which although upsetting and heated, did not seem to be the sort of experience that the research was intended to capture. Many of these cases involved legal, financial and other serious disputes, or respondents who were not dependent on the perpetrator or very vulnerable. While the described behaviours were potentially upsetting, they were the least severe of those reported. They included, for example, a series of heated exchanges or arguments, or minor physical altercations such as someone pushing past someone during an argument. Some of the allegedly abusive behaviours appeared to be normal expressions of disagreement and conflict in adult relationships (Harbison Reference Harbison1999). If behavioural definitions are too narrow, they risk excluding moderate and low-severity incidents of mistreatment. Such incidents may be the most prevalent and can be harmful or upsetting for older people, so it is important that they are recognised. On the other hand, if behavioural definitions are too encompassing, they will not make a meaningful distinction between abuse and other conflicts or disputes, which would mean that older people are subject to policy and third-party interventions that similar conflicts and disputes amongst other adults would not prompt.
Where the perpetrators had cognitive impairments, including dementia, severe mental illness or behavioural disorders, the harmful behaviours were sometimes extreme. For example, there were reports of respondents being physically attacked and in fear for their safety, and of the police, social and health-care professionals becoming involved. In some of these cases, given the severity of the harm, the behaviour could be considered abusive, but there were also many such cases when the perpetrator's ‘aggression’ was quickly contained and not the source of fear or concern for the older person caring for them. For example, the wife of one of the respondents had Alzheimer's disease and when distressed sometimes hit out at her husband. These incidents were relatively infrequent and he felt that he could manage them with little effort. He did not consider himself in any way abused by his wife and did not understand why the interviewer wanted to focus on this when there were other aspects of the situation that caused him far more distress and difficulty.
Finally, there were examples of harms being ascribed to individuals when the underlying problem appeared to be a failure of formal services. For example, one respondent was recorded in the survey as having been neglected by a care worker. The follow-up qualitative interview established that she was unable to get washed or dressed without the care worker's help, but that some days the worker did not come. The interview revealed that the respondent received assistance from several care workers. We were later able to establish that when a worker failed to show, this was because the providing organisation had not allocated a replacement, rather than a failing or neglect by any individual care worker. Another example concerned a husband who was described in the survey as neglecting his wife. It turned out that because of a long-standing phobia, he was unable to undertake a particular personal care task even though he willingly provided many other forms of support and care. The wife relied on health services to perform the avoided task, but it was not always provided when needed. Overall, the behavioural definitions appear to need further refinement, with particular attention to the tendency to be over-inclusive. Consideration also needs to be given to the ambiguities and difficulties involved in classifying the harms arising from more complex situations and situations where there are underlying service failures.
Chronological age in discriminating ‘elder’ abuse
The respondents were asked about incidents that occurred after turning 65 years of age. Chappell et al. (Reference Chappell, Gee, McDonald and Stones2003: 3) argued that defining old age as beginning at 65 years is a social construction, influenced by the age at which people are expected to withdraw from the workforce, rather than having any biological basis. It can therefore be argued that distinguishing the mistreatment of different groups of adults on the basis of their chronological age is arbitrary, and that the label ‘elder mistreatment’ unnecessarily problematises old age (Leroux and Petrunik Reference Leroux and Petrunik1990). Some commentators have argued that a better alternative would be to develop an age-free concept of vulnerability (e.g. Kane Reference Kane, Harel, Erlich and Hubbard1990). While this study has identified various apparent age-related factors that are linked with the occurrence and experience of elder mistreatment, we emphasise that these factors do not apply to all older people (and some apply to only a small minority), and are rarely, if ever, unique to older people. There was also evidence that some of these factors are socially rather than biologically determined, and that some manifest ageism, sexism and other discriminatory attitudes.
Age-related poor health is commonly considered relevant to the mistreatment of older people and is implicit in the frequently described ‘stressed carer’ scenario. This and other similar surveys have confirmed a clear relationship between mistreatment and poor health. Mistreatment among men with self-reported ‘bad’ or ‘very bad’ health was almost ten times higher than among men with ‘good’ or ‘very good’ health, and for women the equivalent ratio was over six. The connection between chronological age and health varied enormously among the respondents, however, and in fact most did not have poor health: 61 per cent of all respondents described their health as ‘very good’, another 31 per cent as ‘fair’ and only eight per cent as ‘bad or very bad’. Poor health is not unique to older people. The reported incidents and experiences of mistreatment included those where poor health appeared to have a bearing on the mistreatment or its effects, but there were also examples where poor health did not appear to be relevant. Reliance on others for washing and dressing because of poor health featured in some accounts. Others spoke of how experiencing health problems had made them feel generally more vulnerable and less able to stand up for themselves. In other cases, respondents reported that their health had worsened as a result of mistreatment. Mental frailty also featured in cases of doorstep and other types of fraud or deception. Some respondents who thought themselves in good health believed that, because older people are frequently perceived as being frail and vulnerable, they were ‘easy targets’. Loneliness is not confined to older people but featured in some accounts, with both the survey and qualitative research suggesting that this increased the risk of mistreatment. Some of the qualitative research respondents described feeling very isolated and/or expressed fear of being alone during their final years. In some cases, fear of being alone caused respondents to stay in abusive relationships or to get involved in relationships that in the view of friends and family were ill-advised and that later became abusive.
There were also disputes and difficulties about a range of practical and financial issues which are likely to have above-average frequency among older people. These included disputes over the settling of deceased spouses' estates, and concerns about children or others trying to obtain property and money through a power of attorney, by assisting in the management of financial affairs, or by pressurising older people to include them in wills or to benefit them financially in other ways. Explicit ageism also featured in various incidents with neighbours, acquaintances and others, sometimes in conjunction with other discriminatory attitudes. This included use of the term ‘old’ as an insult and situations where it appeared that older single or widowed women were targeted for unwanted sexual advances because, in the words of one respondent, it was assumed they were not ‘getting any’. Conversely, there were also cases where there appeared to be no apparent age-related factors relevant to the experience of mistreatment. This included some incidents of theft, inter-personal abuse and long-standing domestic abuse. The value and purpose of maintaining an age-related concept of mistreatment requires clearer articulation and there is a need to clarify and distinguish the roles of chronological age, apparently age-related difficulties and ageism, as well as sexism and other discriminatory attitudes. There is also a need to situate elder mistreatment more clearly in relation to all types of mistreatment of all adults.
Conclusions
The UK Study of Abuse and Neglect of Older People provided a valuable opportunity to explore the definitional issues that are the starting point for all epidemiological or aetiological understanding, and its findings suggest that elder mistreatment continues to exhibit what Finkelhor and Pillemer (Reference Finkelhor, Pillemer, Hotaling, Finkelhor, Kirkpatrick and Strauss1988) described as ‘definitional disarray’. It may well be that abuse, neglect and the embedded concept of ‘expectation of trust’ are essentially contested concepts, which like ‘love’ or ‘fairness’ invoke widespread agreement about an abstract general notion but lead to unresolved arguments about precise and operational definitions (Gallie Reference Gallie and Gallie1964). To the degree that this is the case, final and authoritative definitions of elder mistreatment are unlikely to be achieved. Certainly definitions of elder mistreatment continue to reflect a range of concerns in the development of policy and practice and the different perspectives of vocational and interest groups (Stones Reference Stones and MacLean1995).
If research is to be effective and useful, however, clear, understandable and unambiguous definitions of elder mistreatment are required. To the degree that the idea of elder mistreatment is essentially contestable, it may be that definitions will need to be provisional, flexible and pragmatic, and particular to specific research and policy purposes. What is clear is that current definitions of elder mistreatment require further clarification and elucidation, particularly with regard to the notion of trust, the scope and nature of behavioural definitions, and the role and relevance of chronological age. Without such clarification and development, there is a danger that much of the energy and time given to research and debate will be undermined by fuzzy and unclear notions of what exactly it is that is being discussed. Unless we are clear about what we are measuring and trying to understand, research findings will be less helpful and informative than they should be.
Acknowledgements
The views expressed in this paper are those of the research team, not necessarily those of Comic Relief or the Department of Health in England. The authors are grateful to the participants in the interviews and to everyone who contributed to the study. More details about the study can be supplied by the lead author.


