


Introduction
Background & Rationale
The World Health Organization's (WHO's; Geneva, Switzerland) Foreign Medical Team (FMT) Working Group was established in response to growing concerns about the standards and competencies of FMTs that responded to sudden onset disasters (SODs). 1 There has been an increasing drive toward professionalizing the humanitarian response since the 1988 earthquake in Armenia,Reference Noji 2 following which (amongst other recommendations) was a recognition that better medical record keeping would improve post-event analysis and planning for future events.Reference Noji 2
Wherever and whenever medicine is practiced, a standardized method of recording and reporting patient encounters is needed both for the purposes of improving communication for individual patient follow-up, but also to allow for simpler collation and sharing/analysis of data to identify effective practices and inform the response to SODs. 3 An editorial by Mills et al drew attention to the pressing need for an overhaul in the way information from SODs is disseminated, mainly in terms of comprehensiveness, timeliness, accuracy, and transparency.Reference Mills, Robinson and Attaran 4
During the Haiti earthquake of 2010, arrangements for follow-up of surgical procedures were shown to be lacking. There were a number of reasons cited for this, including the number of different agencies involved in delivering care. This can be addressed by adherence to a standard method of recording and sharing data between registered teams to ensure standard follow-up procedures are completed.Reference Chu, Stokes, Trelles and Ford 5
This review interrogated the available literature for examples of medical record keeping by FMTs in SODs.
Objectives
This review sought to examine the published literature for:
-
1. What systems of medical record keeping have been used by FMTs in SODs;
-
2. What information has been collected by FMTs, as described in their publications;
-
3. How FMTs develop their medical record format; and
-
4. How the record is used once it is complete.
Report
Methods
Information Sources—Studies were identified by an electronic-database search. No limits were set for date or language; foreign language papers of significant interest were translated into English. The search was applied to the following databases:
-
• Scopus (produced by Elsevier; Amsterdam, Netherlands);
-
• Web of Knowledge (now “Web of Science,” produced by Thomson Reuters; New York, New York USA);
-
• Trip Database (produced by Jon Brassey and Dr. Chris Price; UK);
-
• British Nursing Index (produced by ProQuest LLC; Ann Arbor, Michigan USA);
-
• Cumulative Index to Nursing and Allied Health Literature (CINAHL; produced by EBSCO Information Services; Ipswich, Massachusetts USA);
-
• Embase via OVID (produced by Elsevier; Amsterdam, Netherlands);
-
• Medline via OVID (produced by Medline Industries, Inc; Mundelein, Illinois USA);
-
• PsycINFO via OVID (produced by the American Psychological Association; Washington DC, USA);
-
• Health Management Information Consortium (HMIC) via OVID (produced by the Department of Health's Library and Information Services and King's Fund Information and Library Service; UK);
-
• ProQuest (produced by ProQuest LLC; Ann Arbor, Michigan USA);
-
• PubMed (produced by National Center for Biotechnology Information; Bethesda, Maryland USA);
-
• Fade Library (produced by Liverpool Primary Care Trust; UK); and
-
• Applied Social Sciences Index and Abstracts (ASSIA) (produced by ProQuest LLC; Ann Arbor, Michigan USA).
Search—The basic search strategy involved a search for “Medical Records” (or its synonyms) combined with a search for “Sudden onset disaster” (or its synonyms) or “Foreign Medical Team” (or its synonyms). Identified studies were found by searching 13 electronic databases (on dates from August 27, 2013 through September 2, 2013) and a review of bibliographies of those studies deemed relevant to the review. Full details of the search may be found in Appendix 1 (available online only).
A secondary, limited literature search was performed to uncover any relevant missing work. A list of names (and limited synonyms) of the nongovernmental organizations on the Global Health Cluster (GHC) list 6 was created. All were included, unless:
-
1. The organization name generated an unmanageable number of unrelated results; and
-
2. The organization was not directly involved in dispatching teams to SODs.
The search was limited only to Medline and Embase, via the Ovid platform. Full details of the search may be found in Appendix 2 (available online only). A flow diagram of both searches is shown in Figures 1 and 2.
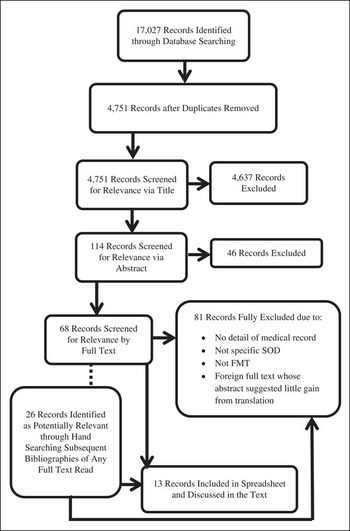
Figure 1 Flow Diagram of Included Records Following Primary Search. Abbreviations: FMT, foreign medical team; SOD, sudden onset disaster.

Figure 2 Flow Diagram of Included Records Following Secondary Search. Abbreviation: SOD, sudden onset disaster.
Eligibility Criteria—Any written piece produced by an FMT following an identified SOD making reference to the content of a patient-encounter record was included. Peer-reviewed journal articles were included, as well as published reports and conference proceedings.
Data Extraction
All papers that fit criteria for inclusion were entered in to a table with the headings shown in Table 1.
Table 1 Headings Used for Table of Data Extraction

Results
Study Selection
Studies that alluded to collection or analysis of medical case data by an FMT within the setting of an SOD, and described, or at least referred to, the medical record used in this process, were initially included. Papers where abstracts were in English, but whose full text was in another language, were only translated if the abstract indicated there would be unique and important content within the full text that would significantly enrich this review.
Following the primary search (shown in Figure 1), 68 papers were identified as possibilities for inclusion into the data extraction table. Following a hand search through their bibliographies, a further 26 studies were identified. Following full-paper analysis, 13 papers were included (Appendix 3; available online only) and the rest were excluded from the main discussion because:
-
1. They gave no detail of the medical record used;
-
2. They were not from an FMT;
-
3. They did not refer to a specific SOD; and/or
-
4. They had a foreign language full text, but the abstract suggested minimal novel information to be gained from translation.
Following the secondary search (shown in Figure 2), a further two papers fit the inclusion criteria and were added to the data extraction table in Appendix 3 (available online only).
Overall, two papers had their full texts translated to English, one from Mandarin, the other from German.
Study Characteristics
Fifteen studies over a period of 32 years (1979-2011) were included. The predominant type of SOD referred to in nearly two-thirds of papers was earthquake, followed by tsunami and hurricane. Table 2 shows this breakdown in full (note that one paper discussed two separate SODs).
Table 2 Type of SOD Referred to in Included Studies

Abbreviation: SOD, sudden onset disaster.
As shown in Table 3, four papers were focused on the Asian tsunami of 2004 and three were concerned with the Haitian earthquake of 2010. The remaining papers referred to nine separate SODs.
Table 3 Specific SODs, Named Only Where There are Two or More

Abbreviation: SOD, sudden onset disaster.
The majority of papers did not delineate the entire content of the record; instead, they referred to data “included” in the record. Table 4 shows a raw breakdown of what was contained within the records according to what was written in the papers.
Table 4 Information Present Within Medical Record

Abbreviation: PTSD, posttraumatic stress disorder.
Syntheses of Results
Variability existed in record keeping between FMTs, according to the included studies. However, the FMTs represented in the published literature were a fraction of the number of FMTs in operation. This paucity of published data made it difficult to establish the true level of variation in record-keeping methods across all FMTs.
Currier et al from Project Medishare and Burnweit and Stylianos from the American Red Cross (Washington DC, USA) described clearly that they had no adequate medical record-keeping method suitable for the response to Hurricane Katrina and the Haiti earthquake, respectively, and thus, one had to be developed during the response.Reference Currier, King, Wofford, Daniel and deShazo 7 , Reference Burnweit and Stylianos 8 In the latter, the authors agreed that the method of record keeping needed to be prepared in advance but be capable of modification according to situational needs. Theirs was one of the only papers to state that the patient's guardian was provided with a summary of the record.Reference Burnweit and Stylianos 8 The record they eventually used demonstrated the important aspects of note keeping, which arose during the response.Reference Burnweit and Stylianos 8 Unfortunately, no further details could be obtained from Currier et al regarding the record which evolved during Hurricane Katrina.
At the same time as the American Red Cross team was developing their record, a team comprising Fond Parisien Disaster Rescue Camp (Haiti), Operational Medical Institute (Global), and Harvard Humanitarian Initiative (Cambridge, Massachusetts USA) were trialing an electronic medical record for managing Haiti earthquake casualties.Reference Callaway, Peabody and Hoffman 9 This was the only paper to highlight that its record included individual tent and/or social security numbers. This kind of information is required in order to track data to the correct person; however, it raises questions of confidentiality and ownership of data.
The third paper produced from the Haiti earthquake of 2010 came from the Morbidity and Mortality Weekly Report produced by the Centers for Disease Control and Prevention (Atlanta, Georgia USA). 10 The University of Miami Global Institute (Florida USA)/Project Medishare group used field-hospital paper notes to collect standard information; although, it was unclear what happened to these notes following the patient encounter. They made a specific point of recording diagnoses which were not injury-related because this made up 42% of the admissions to the field hospital. 10 This fact in itself demonstrated that a medical record for a SOD must have a minimum data set (MDS) comprising some method of collecting non-injury-related medical problems.
The Hong Kong Red Cross (China), in their data from the Sichuan/Wenchuan earthquake, did not provide much detail of the medical record they used; however, they too cited that just under 40% of patients presented with chronic health problems. 11 All the other papers citing the content of the medical records used in the Sichuan/Wenchuan earthquake reflected work done by local medical teams (LMTs). This is likely to be because the Chinese government mostly managed the earthquake itself with minor outside input. 12
Another common source of publications was the South Asian tsunami of 2004. The International Committee of the Red Cross (ICRC; Geneva, Switzerland), Indonesian Red Cross, and Norwegian Red Cross, in combination, were included in two papers. The first found that 29% of surgical interventions were directly tsunami-related; however, many non-disaster-related surgical cases also came to the field hospital in Banda Aceh (Indonesia).Reference Riddez, Kruck, Gardarsdottir and Redwood-Campbell 13 Medical records must, therefore, be suitable for all the cases that may attend a field hospital. The second paper from the same group had a different focus: they were collecting data nine weeks after the tsunami using a specific data collection tool.Reference Redwood-Campbell and Riddez 14 They found that only 12% of patients at that stage were attending with conditions directly connected to the SOD.Reference Redwood-Campbell and Riddez 14 According to the authors, prior to their data collection tool, the only reliably collected information was age and gender, and because patients took their notes home with them, there was no reliable way of accessing them further.
A team from Korea University (Greendoctors) was also present in the aftermath of the tsunami.Reference Lim, Yoon, Jung, Kim and Lee 15 This team was prepared for data collection in advance and kept medical records on all patients. In keeping with what was found in the other papers from the tsunami, most presentations were of chronic health problems.Reference Lim, Yoon, Jung, Kim and Lee 15 Another Korean team (the Korean Disaster Medical Assistance Team (DMAT)) started collecting data seven days after the tsunami, and they too recognized the burden of medical rather than surgical/trauma cases amongst those presenting for health care.Reference Kwak, Shin, Kim, Kwon and Suh 16 These observations were in keeping with well-established comparisons of, and commentaries on, tsunamis and earthquakes. In tsunamis, those with bad injuries were unlikely to be able to swim, and therefore, to survive, hence a higher ration of those dead to those injured; whereas in earthquakes, more of those badly injured were likely to survive.Reference Gerdin, Clarke and Allen 17 , Reference de Ville de Goyet 18
The earliest included paper was published in 1983 about the 1979 Tumaco earthquake in Colombia.Reference Gueri, Guerra and Gonzalez 19 Authors discussed multiple aspects of the earthquake response; many groups were involved, including local hospitals, the Red Cross, the fire department, civil defense, family welfare, the ministry of health, and departmental health services. Even from this disaster nearly 35 years ago, suggestions were made for having a quick “card” system of recording information to improve data collection.
The ICRC's field hospital in Kashmir, following the earthquake in 2006, produced a short paper that cited a large proportion of surgical/trauma victims were eventually hospitalized (almost 92%).Reference Helminen, Saarela and Salmela 20 This high surgical/trauma load two weeks after the earthquake was due to regional geographical difficulties; patients requiring surgery had not been easy to access earlier on. As time went on, the proportion of injured patients reduced in favor of patients with medical illness. Therefore, a medical record must be easily adaptable to an MDS covering illness as well as injury, because the proportions of each will vary over time.
Several DMATs from the Federal Emergency Management Agency (Washington DC, USA) were sent to Hawaii (USA) following Hurricane Iniki in 1992.Reference Henderson, Lillibridge, Salinas, Graves, Roth and Noji 21 These teams were LMTs working within US territories; however, the practicalities of their mobilization and deployment may be compared to that of an FMT. The authors demonstrated the split of cases (with data collection commencing five days after the hurricane passed the island), which included approximately 40% with injuries. They reported that records varied from a comprehensive patient account to a basic list of the numbers of patients treated in a day. The authors suggested that one member of the team could be assigned the role of data collection to ensure this was more accurate and reliable.Reference Henderson, Lillibridge, Salinas, Graves, Roth and Noji 21
The New Mexico-1 (USA) DMAT responded to both hurricane Andrew in 1992 and the flood from tropical storm Allison in 2001.Reference Nufer, Wilson-Ramirez and Crandall 22 The premise of this paper was to compare the medical needs of patients from each SOD by comparing information contained within the DMAT's medical encounter form. There was more medical history and prescriptions for the hurricane patients, despite a similar age range. The authors suggested this could be due to different evacuation patterns between the two SODs, or because hurricanes cause more structural damage, and thus, getting into a home to retrieve medication becomes more difficult.Reference Nufer, Wilson-Ramirez and Crandall 22 The flood patients presented more with illness than injury as compared to the hurricane, which is in keeping with more wound-causing debris after a hurricane. These differences may be predictable partly because of the pattern of impact of different SODs, as shown in Table 5, which was produced by the Pan-American Health Organization (Washington DC, USA). 23
Table 5 Pattern of Impact of Different SODs

Abbreviation: SOD, sudden onset disaster.
aPotential lethal impact in absence of preventative measures.
The Japan Self-Defense Forces provided medical intervention in the Honduras floods of 1998.Reference Shinchi and Ashida 24 The primary author of this paper was present at this operation and noted that standard hospital records are not suitable for such situations. Similarly, they noted that triage tags were too brief. Therefore, they proposed their own record, which fit onto a single sheet of paper and adopted the use of circling items if they were there or not, to facilitate efficiency of use.Reference Shinchi and Ashida 24 The authors described what happened to the record (ie, if it was being used as a prescription chart as well as a record, it was handed in at the pharmacy, and if not, it was handed in to the treating medical officer). They also translated it into two languages (English and Japanese) for use in forthcoming disasters.Reference Shinchi and Ashida 24 This record was developed by a specific organization according to the need they identified during a specific SOD and provides some good insight into key considerations when developing a medical record, based on experience in the field.
Cyclone Nargis took place in Myanmar in 2008 and a Korean disaster relief team reviewed the medical records of over 2,000 patients seen in their clinics.Reference Kim, Han, Kim, Kim and Hong 25 , Reference May, McGwin and Lancaster 26 Very few trauma cases were included in the medical workload, despite the SOD being a cyclone. However, the team collected data from patients seen one month after the SOD, which may explain the reduced trauma workload at that stage.Reference Kim, Han, Kim, Kim and Hong 25 This reinforced that medical records for SODs should be designed to accommodate different timescales after disasters, and therefore, a wide enough range of medical conditions, while remaining short and simple to complete.
Discussion
Medical record keeping by FMTs in SODs can represent a distinct challenge in terms of time and resources. Nevertheless, to achieve the basics of good medical practices as expressed by the medical councils of the UK, the USA, Australia, India, Pakistan, and Hong Kong, as examples of national regulatory bodies, timely and accurate records must be a high priority. 27 - 32 There are now WHO minimum standards for FMTs, which include a commitment to:
-
1. Report regularly (using either national or internationally agreed reporting format) to the national authorities both during the response and prior to departure;
-
2. Keep confidential records of interventions, monitoring, and complications;
-
3. Provide individuals with a treatment record and a referral/follow-up plan; and
-
4. Join a wider referral system, both accepting from and referring to other FMTs, LMTs, and approved other countries. 33
There is considerable variation in the aspects of medical record content which is emphasized by different teams within their papers. This may suggest that there is a difference of opinion as to what information is considered most useful, and therefore, may be a useful starting point for developing an MDS.
This review has demonstrated the potential benefits of developing standards of practice surrounding what should happen to the record following the patient encounter. Furthermore, this review highlights how important it is that the MDS contains enough scope for the medical (rather than just surgical/trauma) presentations seen in high numbers, depending on the type of SOD and time elapsed since it occurred.
Although the intention to improve record keeping is primarily to improve care on an individual and population level, there is also a rising global requirement for improved accountability of FMTs. This is especially true in the context of a growing and very open cynicism over the role of the aid “industry” and its economic/political motivations balanced with the notion of the humanitarian cause. 34 In the UK, following the Humanitarian Emergency Response Review (HERR), 35 focus on this has been sharpened because the report identified accountability as one of the seven key areas of new approach. Another of these objectives is “to innovate,” and to achieve this, accurate data are needed from SODs to feed into work by organizations, such as Enhancing Learning & Research for Humanitarian Assistance (Global) 36 who are a dedicated collaborative network supporting the generation of an evidence-base for humanitarian intervention.
The benefits of standardized medical record keeping and reporting by FMTs in SODs may contribute to those specific goals of the GHC and HERR:
-
1. Better individual care and patient-centric care; 33
-
2. Accountability to the patient and the community; 35
-
3. Better disease early-warning and notification to allow outbreak and surveillance to begin early; 33
-
4. Better referral pathways and support of local health systems; 33 and
-
5. Better data, research opportunities, and quality improvement. 35
Limitations
Reviewing the literature alone is not enough to gain an accurate picture of what the large numbers of FMTs are doing in SODs, because there is a scarcity of relevant publications. In addition, commentary on medical records may be brief within a paper; therefore, this search, though aiming to be thorough, may have missed some relevant publications. The authors have included some papers from well over 20 years ago. This may be critiqued because the concept of standardized medical records, even in civilian practice, has been a development better connected with the past 10 years. However, the authors considered it important to highlight that medical record keeping in SODs has presented challenges for a long stretch of time, and it is only very recently that work has been started to look at how to improve it. Further work must entail targeting experienced FMTs and LMTs directly to find out the exact content and structure of their current patient records, as well as how they were developed. These may then be analyzed in comparison. This will provide further information for the development of an MDS to improve the design and content of a standard medical record for SODs. It has already been established that a liaison between local and foreign teams improves the coordination and effectiveness of a medical response to an SOD; therefore, it is also likely to improve the quality of data collection design.Reference Roy, Shah, Patel and Coughlin 37
Conclusion
It is an inescapable fact that record keeping is an integral aspect of health care delivery. At best, the literature demonstrates that attempts are undoubtedly being made to make records. However, the practice across providers of humanitarian aid is not subject to a minimum standard and varies widely. This situation undermines the quality of care being provided by FMTs in SODs. Work to establish how the WHO recommendations can be implemented must take place via engagement with LMTs in order that a cohesive solution is found to standardize FMT record collection, storage, and reporting.
Supplementary material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S1049023X15000102









