We present a newborn infant with a circumaortic double left innominate vein. The patient presented in extremis due to severe coarctation of the aorta, and while assessing the aortic arch on the initial echocardiogram, an abnormal vessel pattern was noted in the suprasternal long-axis aortic arch view. Previously described as a “double circle” sign, Reference Malakan Rad1 two vessels were seen passing underneath the aortic arch with another passing over the arch (Fig 1). Further investigation of this abnormal finding in the orthogonal plane revealed a bifurcation of the left innominate vein into branches that coursed above and below the aortic arch and inserted into the superior caval vein at separate locations, thus encircling the aorta (Fig 2).

Figure 1. 2-D echocardiographic image in the suprasternal long-axis aortic arch view demonstrating “double circle” sign (AAo = ascending aorta; RPA = right pulmonary artery; SbDLIV = subaortic double left innominate vein; SpDLIV = supraaortic double left innominate vein).

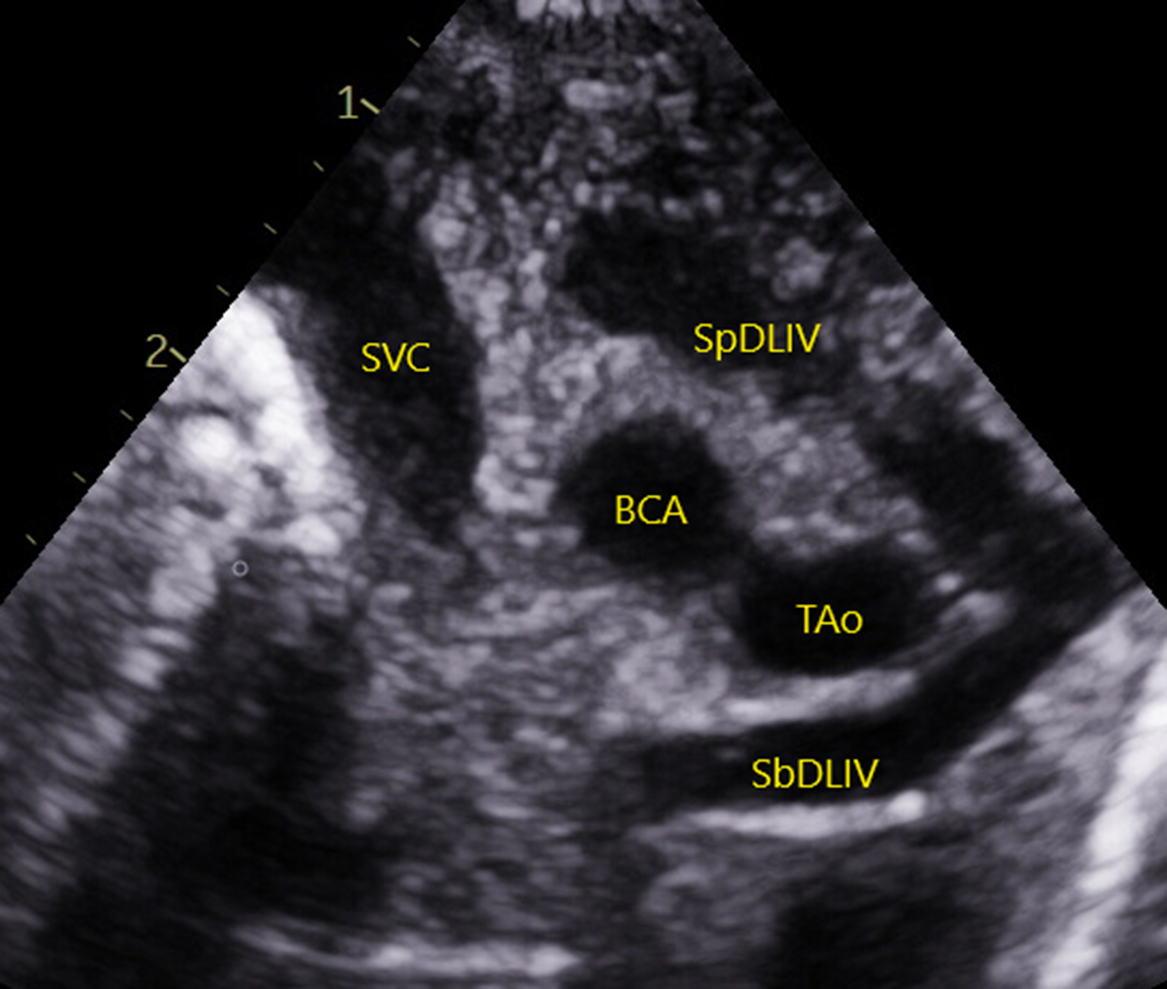
Figure 2. 2-D echocardiographic image in the suprasternal coronal view demonstrating the bifurcation of the double left innominate vein and their circumaortic course (BCA = brachiocephalic artery; SbDLIV = subaortic double left innominate vein; SpDLIV = supraaortic double left innominate vein; SVC = superior caval vein; TAo = transverse aortic arch).
Intraoperative findings confirmed the echocardiographic diagnosis of circumaortic double left innominate vein (Fig 3). Diagnosis of this rare systemic venous anomaly was particularly important prior to this neonate’s operation as the vessels encircled the hypoplastic aortic arch, directly affecting the surgical field of interest. While the surgical approach via median sternotomy due to the hypoplastic transverse aortic arch was not directly affected by the venous anomaly, knowing about the abnormality pre-operatively, the surgeons were able to quickly confirm the anatomy, mobilise and retract the subaortic left innominate vein away from the hypoplastic arch, and repair the aortic arch without any added difficulty or complications. The double left innominate vein was left intact as there was not any evidence to suggest it would cause any clinical problems in the future, although it will be observed over time as the patient is followed post-operatively in the outpatient setting.

Figure 3. Intraoperative photograph of circumaortic double left innominate vein (AAo = ascending aorta; SbDLIV = subaortic double left innominate vein; SpDLIV = supraaortic double left innominate vein).
Anomalies of the left innominate vein are rare, with double left innominate vein being the rarest type. Reference Ko, Sun and Liang2 While circumaortic double left innominate vein has been previously reported in a handful of patients with CHD, Reference Gupta, Theut, Joshi and Aggarwal3,Reference Subirana, de Leval and Somerville4 to our knowledge this is the first reported case diagnosed solely using echocardiography, and the first such case where diagnosis was particularly important to surgical planning.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflict of interest
None.