



Sotalol is a Vaugh Williams class III antiarrhythmic medication used for the treatment of supraventricular and ventricular arrhythmias. As Kpaeyeh and Wharton describe, sotalol is a competitive inhibitor of the rapid component of the delayed-rectifier potassium current. Its inhibition results in prolonged action potential and effective refractory period durations.Reference Kpaeyeh and Wharton 1 It also exhibits mild β-adrenergic-blocking properties as its l-isomer has non-specific β-adrenergic-receptor inhibition capacity, which is thought to be the primary driver of the bradycardia seen.Reference Blair, Burgess and Maxwell 2 Clinically, there is a slowing down of the heart rate and an increase in the QT interval.
Sotalol’s relatively rapid onset makes it a good choice for ICU settings where patients often require rapid titration of medications. Its use in the United States of America, however, has been limited, because, until recently, sotalol was available only as an enteral preparation. With an intravenous preparation now available (AltaThera Pharmaceuticals, Chicago, Illinois, United States of America), its use in medically complex children is now being described. We present the case of an adolescent with refractory atrial arrhythmias in whom intravenous sotalol was used.
Case description
An 18-year-old male patient with relapsed refractory Hodgkin’s lymphoma was hospitalised following a bone marrow transplant. His hospital course was complicated by pancytopaenia, septic shock, respiratory failure, and acute renal injury requiring continuous renal replacement therapy. He had graft-versus-host disease, primarily affecting his gastrointestinal tract, rendering him dependent on parenteral drug administration. He also had hepatic dysfunction from hepatic sinusoidal obstructive syndrome/veno-occlusive disease. His baseline electrocardiogram was significant for sinus tachycardia with a borderline prolonged corrected QT interval of 454 ms. During this admission, he was treated with known QT-prolonging medications such as voriconazole, tacrolimus, ondansetron, and citalopram.
Two weeks after transplant, he developed new-onset atrial flutter with 2:1 to 3:1 atrioventricular conduction (Fig 1). Before planned cardioversion, the arrhythmia terminated spontaneously. Within 48 hours, he again developed an atrial arrhythmia, although in this instance it was fibrillation with rapid ventricular response – ventricular rate of 145 beats per minute. This also self-resolved without treatment.

Figure 1 Atrial flutter with 2:1 to 3:1 conduction. The ventricular rate is 183 beats per minute.
Laboratory values showed normal serum sodium, potassium, chloride, magnesium, and phosphorous levels He, however had hypocalcaemia, requiring replacement therapy, and had hyperglycaemia. Renal studies were abnormal with a blood urea nitrogen level of 36 mg/dl and a creatinine concentration of 1.8 mg/dl. The estimated glomerular filtration rate on continuous renal replacement therapy was >60. Liver function tests were abnormal with a conjugated bilirubin concentration of 9.4 mg/dl and an unconjugated bilirubin concentration of 1 mg/dl. Aspartate aminotransferase and alanine aminotransferase values were 192 and 209 IU/L, respectively. Alkaline phosphatase was elevated at 264 IU/L and γ glutamyltransferase was 370 IU/L. He was pancytopenic with severe neutropaenia with an absolute neutrophil count of 210.
An echocardiogram was performed and revealed a circumferential pericardial effusion measuring ~1 cm in diastole. Both right and left ventricles were under-filled, with the left ventricle displaying hyperdynamic systolic function with mid-cavity obliteration – peak velocity of 3.2m/second. No thrombus was identified in the right atrium. Central-line tips were not visualised. Though the effusion was concerning based on echocardiographic measures, which showed mitral valve respiratory inflow variation of 19% and tricuspid valve respiratory inflow variation of 32% in addition to right atrial free-wall collapse and intermittent right ventricular diastolic collapse, it did not appear to be clinically haemodynamically significant, as the heart rate was 135, blood pressure was 135/85 mmHg, and the central venous pressure was 6 mmHg. The team did not consider pericardiocentesis as therapy for the arrhythmia and ultimately decided to observe.
Because of repeated episodes of atrial tachyarrhythmia and associated haemodynamic instability, a decision was made to initiate antiarrhythmic therapy. After discussion with the cardiology team, intravenous sotalol was selected as the first-line therapy. Secondary to chronic disease, the patient was small for age, more in line somatically with a 15–16-year-old boy. He was underweight, with muscle wasting from his prolonged hospitalisation. Establishing a safe but effective dose of sotalol was important, not only because of his renal failure but also because of his decreased body surface area: weight, 57 kg (11%); height, 172 cm (27%); body surface area, 1.64 m2. He received 30 mg of intravenous sotalol every 12 hours for five total doses for 2.5 days until he could be transitioned to enteral sotalol. The intravenous sotalol was dispensed to a final volume of 2 ml at a concentration of 15 mg/ml infused over 15 minutes with no significant hypotension or haemodynamic instability observed.
Following sotalol administration, the arrhythmias became quiescent and the patient suffered no further sustained arrhythmias during this period of hospitalisation. His QT interval was monitored daily until five estimated half-lives had elapsed and the drug was presumed to be at steady state. His corrected QT interval prolonged from a baseline of 454–480 ms on therapy (Fig 2). His resting heart rate decreased from 133 beats per minute at baseline to 114 beats per minute on intravenous sotalol. He remained on telemetry while in the ICU and he suffered no proarrhythmic side effects related to sotalol therapy; specifically, he had no episodes of torsades de pointes. After further recovery, he was transitioned to oral sotalol. This was continued for an additional 4 weeks, after which it was felt that he was at low risk for recurrent arrhythmia, and the oral sotalol was discontinued. The patient was discharged after 3 months and has had no recurrence of atrial arrhythmia since.
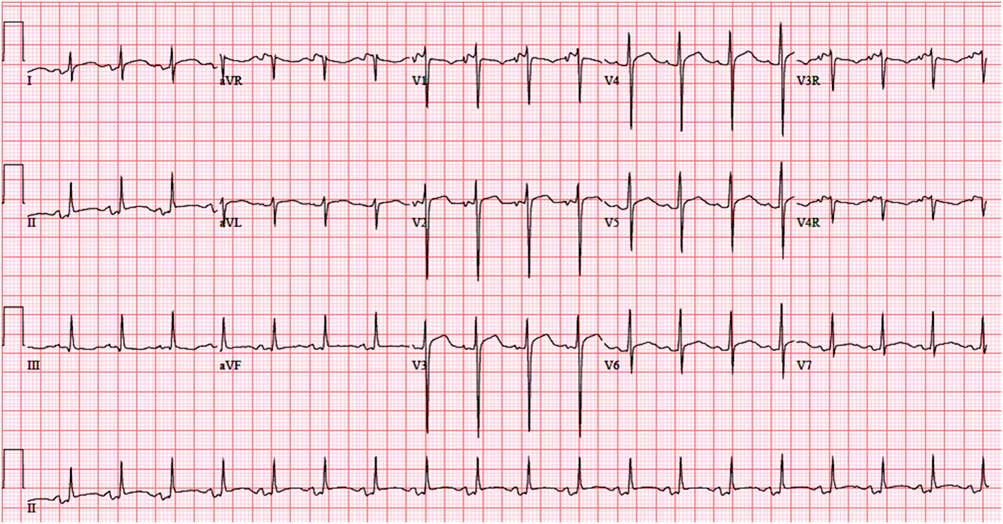
Figure 2 Electrocardiogram post intravenous sotalol, demonstrating sinus tachycardia at a rate of 114 beats per minute. There is a prolonged corrected QT interval of 480 ms.
Discussion
The decision tree for choosing antiarrhythmic medications in the ICU setting is complex and often constrained by multiple competing factors. This patient’s course was complicated by intestinal graft-versus-host disease precluding an enteral route of drug delivery. Choices of intravenous antiarrhythmic medications are limited.
The pharmacokinetics of enteral and parenteral sotalol are quite similar.Reference Somberg, Preston and Ranade 3 – Reference Pfammatter and Paul 5 Somberg et alReference Somberg, Preston and Ranade 3 found the bioavailability of enteral sotalol to be as high as 90–100% and recommended a conversion factor of 0.9375 of the enteral dose for the intravenous dose. Neither form requires hepatic first-pass metabolism nor does it bind to plasma proteins.Reference Kpaeyeh and Wharton 1 , Reference Somberg, Preston and Ranade 3 Peak serum concentration is reached ~2–3 hours after a single dose of sotalol.Reference Kpaeyeh and Wharton 1 , Reference Pfammatter and Paul 5 It is unchanged without metabolites and is dependent on renal function for clearance.Reference Kpaeyeh and Wharton 1 , Reference Pfammatter and Paul 5 In those patients with normal renal function, the half-life of sotalol is anywhere between 10 and 20 hours.Reference Kpaeyeh and Wharton 1 , Reference Somberg, Preston and Ranade 3 In those patients with renal failure requiring haemodialysis, the half-life can be as much as 30–70 hours.Reference Blair, Burgess and Maxwell 2 Care must also be taken in patients under 2 years of age as they exhibit prolonged drug half-life and increased time to steady state.Reference Blair, Burgess and Maxwell 2
There are limited studies defining standards in parenteral dosing in children, especially in those with renal dysfunction. We extrapolated our dosing on the basis of the enteral dosing schedule. We utilised the previously described enteral sotalol dosing schedules of 90 mg/m2/day and 2–4 mg/kg/day as starting points for creating a safe dose for our patient. He would have theoretically received between 38 and 50 mg of enteral sotalol every 8 hours if we had followed the standard enteral dosage schedules; however, taking into account his renal failure requiring continuous renal replacement therapy and acknowledging the prolonged half-life of sotalol in the setting of renal dysfunction, in addition to his haemodynamic lability and other organ dysfunction, the decision was made to use a lower dose that was closer to 1 mg/kg/day with a frequency of every 12 hours. In the literature, this is the recommended dosing frequency for adults with a creatinine clearance of >60 ml/minute,Reference Blair, Burgess and Maxwell 2 , Reference Tjandramaga, Verbeeck and Thomas 6 which was being achieved with continuous renal replacement therapy. Also, given his history of hypotension and multidrug QT prolongation, an administration frequency of every 12 hours was thought to be prudent, and we remained prepared to tailor the frequency should he show any adverse effects or toxicity. As an institution, we have adopted delivering intravenous sotalol at a rapid rate, over 10–20 minutes’ duration. As Somberg et alReference Somberg, Preston and Ranade 3 describe, rapid delivery may increase the risk for proarrhythmia. An infusion duration of 5 hours more closely mimics enteral sotalol’s peak serum concentrations; however, they found no differences in total drug exposure based on the duration of the infusion.Reference Somberg, Preston and Ranade 3 We continued to monitor the patient’s vital signs and telemetry for arrhythmias, as well as serial-corrected QT intervals based on electrocardiograms. We used this to tailor his dose while his continuous renal replacement therapy was titrated and weaned.
At first glance, given his known renal insufficiency and need for continuous renal replacement therapy, sotalol would seem to be an unlikely choice. This patient, however, also suffered from hepatic sinusoidal obstructive syndrome/veno-occlusive disease, affecting liver function; this, and the often prolonged loading time, made amiodarone a less than optimal choice. Procainamide also requires dose adjustment for renal dysfunction and has also been associated with blood dyscrasias. Although rare (0.5%), potentially fatal blood dyscrasias such as agranulocytosis, leucopaenia, neutropaenia, and aplastic anaemia have all been described. This complication has been observed within the first few months of therapy.Reference Danielly, DeJong and Radke-Mitchell 7 Though in the literature this is described with sustained-release enteral procainamide, it was a significant concern in the setting of the patient’s already severe concomitant marrow suppression.
Both amiodarone and procainamide are associated with hypotension during loading, which is concerning in a patient with shock and haemodynamic instability. Sotalol does exhibit β-adrenergic-blocking properties and can lower blood pressure in an unstable patient; however, the total effect of sotalol is approximately a third of that of propranolol.Reference Kpaeyeh and Wharton 1 Its effect on systemic vascular resistance is certainly less than that of amiodarone, which is advantageous in a patient with sepsis. Also, sotalol has a theoretical negative inotropic effect from its β-adrenergic blockade; however, the class III effect of increase in action potential duration as well as inward calcium-current flux counteracts this.Reference Kpaeyeh and Wharton 1 , Reference Pfammatter and Paul 5 Our patient had hyperdynamic systolic ventricular function, in the setting of septic shock requiring fluid and pressor support, and theoretically would have benefitted from balancing his heart rate and from adequate ventricular filling, thereby increasing cardiac output.
Despite dependence on renal clearance, sotalol’s pharmacokinetics are fairly well understood, allowing it to be safely adjusted.Reference Hanyok 4 , Reference Tjandramaga, Verbeeck and Thomas 6 It is also possible to monitor for potential sotalol toxicity through careful surveillance of the corrected QT on daily electrocardiograms. Unlike procainamide, which has no suitable oral equivalent, the transition from intravenous to oral sotalol is simple and makes this approach useful for patients who may require long-term antiarrhythmic treatment.
Conclusion
We present the case of a critically ill adolescent with haemodynamically significant atrial arrhythmia requiring intravenous pharmacological therapy. The patient’s multisystem complications directly affected the choice of antiarrhythmic medication. He was successfully managed with intravenous sotalol and then was easily transitioned to enteral sotalol. This illustrates the effective use of intravenous sotalol as a therapy in the paediatric critical-care setting.
Acknowledgement
The authors acknowledge the Seattle Children’s Hospital pediatric intensive care providers and pharmacists who contributed to the care of the patient and to this manuscript.
Financial Support
This research received no specific grant from any funding agency or from commercial or not-for-profit sectors.
Conflicts of Interest
None.


