The World Health Organization (WHO) defines a mass casualty incident (MCI) as “an event which generates more patients at one time than locally available resources can manage using routine procedures…it requires exceptional emergency arrangements and additional or extraordinary assistance.” 1 MCI preparedness at multiple levels of the health-care system significantly reduces morbidity and mortality. Reference Cooke, Chesters and Grier2 Data from high-income countries (HICs), particularly those with frequent MCI events, drove initial MCI management guidelines. These have been further refined through recent high-profile MCI events, including the 2013 Boston marathon bombing, 2015 Paris attacks, and 2005 London bombings. Reference Gates, Arabian and Biddinger3-Reference Aylwin, Konig and Brennan5 Successful MCI response requires multiple stakeholders and components, and strategic planning is required for proper execution.
While MCI protocols are critical to crisis response, to date, they have been mostly designed for HICs. At the community level, emergency responders trained in HIC MCI management are typically equipped with the infrastructure to communicate with hospitals, allowing for redirection of critical patients and management of surge capacity. Reference Gates, Arabian and Biddinger3,Reference Adini, Bodas and Nilsson6-Reference Perry and Lindell8 At the hospital level, key MCI management strategies include developing effective triage mechanisms, designating spaces to accommodate patient overflow, delineating a chain of command that can be activated during emergencies, Reference Gates, Arabian and Biddinger3,Reference Aylwin, Konig and Brennan5,Reference Adini, Goldberg and Laor9-Reference Halpern, Goldberg and Keng11 and ensuring safety and security measures to prevent secondary attacks on health-care providers. Reference Golabek-Goldman12 All of these require regular trainings with staff to ensure readiness. Reference Bin Shalhoub, Khan and Alaska13-Reference Zafar, Jawad and Shamim16
The absence of protocols for MCIs in resource-limited settings is not for lack of need. MCIs are more prevalent in low-income countries (LICs), where poor road traffic safety leads to frequent MCIs. 1 According to a 2004 WHO report, 1.2 million fatalities occur each year worldwide in traffic crashes, greatly exceeding the number of individuals killed in officially designated disasters. 1 It is estimated that up to 90% of road traffic collision (RTC) deaths occur in low- and middle-income countries (LMICs), and they often involve mass casualty situations. Reference Odero, Garner and Zwi17-Reference Peden19 In 2008, one study of trauma patients presenting to a tertiary hospital in Malawi noted 25 MCI incidents over a 5-mo period, 24 of which were from RTCs. Reference Samuel, Akinkuotu and Villaveces20 Another analysis showed that Kenya experienced a 4-fold increase in deaths from traffic injuries from 1973 to 2003, with the majority of deaths occurring from either motorcycle or bus crashes with multiple victims. Reference Odero, Khayesi and Heda21 The true toll is likely higher, as these incidents are also underreported. Reference Mock, Quansah and Kobusingye22,Reference Samuel, Sankhulani and Qureshi23
Despite great need, directly exporting MCI protocols from high- to low-resource settings would be inappropriate given baseline differences in resources and operating environment. Many LICs lack consistent, organized emergency medical services (EMS) entirely, with only one-third of countries on the African continent reporting any formal EMS programs. Reference Zafar, Jawad and Shamim16,Reference Umer, Sepah and Shahpurwala24-Reference Mould-Millman, Dixon and Sefa26 Other countries have limited EMS, but lack standardized means of communication between first responders and nearby hospitals. Reference El Sayed, Chami and Hitti27 Furthermore, hospitals are not always easily accessible to emergency patients: an estimated 29% of people in Sub-Saharan Africa live over 2 h from a hospital, Reference Ouma, Maina and Thuranira28 and true access to emergency care is likely even more limited. Reference Marsh and Rouhani29 Last, many hospitals in LICs, especially in rural areas, lack the clinical capacity to accommodate even small patient surges, both due to ongoing shortages of personnel and supplies, as well as a lack of training on mass casualty response. Reference El Sayed, Chami and Hitti27,Reference Ozoilo, Kidmas and Nwadiaro30,Reference Abdallah, Heinzen and Burnham31 The combination of these factors, often exacerbated by a lack of funding, can negatively affect MCI outcomes. Low-cost, high-impact solutions are critically necessary in these settings.
At Hôpital Universitaire de Mirebalais (HUM), an academic referral hospital in central Haiti, the emergency department (ED) has managed multiple MCI events since opening in 2013 and developed MCI protocols through an iterative process over time. Here, we describe the development of and current MCI protocols at HUM and offer suggestions for hospitals and practitioners in other resource-limited settings.
Methods
Setting
HUM is a 300-bed academic teaching hospital in central Haiti. Haiti is an LIC with limited health service infrastructure, particularly for emergency care. Reference Marsh, Rouhani and Pierre32 There is virtually no formal prehospital care outside of the capital. HUM opened in 2013 with 24-h emergency and surgical care capacity, a rarity in Haiti. In 2014, HUM opened Haiti’s only emergency medicine residency-training program, which graduated its first class in 2017. The ED at HUM is currently a 21-bed unit; patients are also seen in an additional 14 chairs in the center of the room. The ED sees all nonobstetric emergency patients. The central plateau, where HUM is located, has no formal prehospital system. HUM has ambulances that are used for interfacility transport; occasionally, they transport patients from the scene of accidents. Ambulances are staffed by a driver but no medical staff.
Initial MCI Event
On October 10, 2014, a large truck filled with people heading to a market overturned off a small cliff 30 min from HUM. Initial notification for the event occurred when a hospital physician driving by the event called the ED director to report a RTC with multiple apparent injuries and deaths at the scene; the initial patients from the incident arrived at the HUM ED within 1 min of this call. At the time, the HUM ED was already fully occupied with other patients. Within 30 min, 45 new patients with traumatic injuries from the incident had arrived. In the absence of formal MCI protocols, the response was ad hoc. Resources from other services and hospital administration were mobilized. Within 60-90 min, all patients received an initial trauma evaluation and any critical intervention required. Additional planned treatments and diagnostics were prioritized by these initial evaluations. Due to limitations in data and record keeping, the final number of admissions from the ED was unknown, but mortality was limited: 3 patients died in the ED shortly after arrival and 2 more in the operating room. Final mortality at the scene is unknown due to lack of a formal prehospital system; the only available source lists 23 total deaths. 33
Since this event, the HUM ED has continued to have frequent MCIs. Typically, the ED receives 10-12 patients from a single RTC 3-4 times a year and 30 or more patients from a single RTC every 2 years.
Lessons Learned and Protocol Development
After this first large MCI and during subsequent incidents, we developed a process for structured debriefs to review strengths and areas for improvement and to inform response protocols. Debriefs were typically held the same day as an MCI incident; all staff who participated in the event were invited. Most debriefs were multi-sectoral and included clinical and nonclinical staff. Participants discussed the strengths of the response, followed by the weaknesses and ideas for improvement. Through this process, we identified several key areas of focus, notably: (1) communication and notification, (2) organization of patients and physical space, (3) organization of human resources, (4) patient identification, (5) supplies, (6) security, and (7) staff training.
While these areas are similar to challenges identified in high-resource settings, unique approaches were needed given local resource availability. Since 2014, we have successfully implemented a series of solutions, which we have continued to adapt over time based on feedback after subsequent MCIs. These approaches were developed and further refined with involvement from multiple stakeholders, including physician and nursing staff, facilities staff, security, ancillary service staff (laboratory, radiology, pharmacy/warehouse staff), and hospital leadership.
Results
Communications and Notification
One priority area for improvement identified in early MCIs was prehospital notification. In the absence of a formal prehospital system, all notification of trauma events in Haiti is ad hoc. After our initial MCIs, we determined the hospital vehicles (both interfacility ambulances and regular cars) had been summoned to transport patients from the scene by bystanders who called the security and transportation departments at HUM. However, notification had not reached the ED or hospital administration. Since this time, the hospital fleet management teams ensure the ED chief is notified if any hospital vehicles are sent to a scene of a large accident. In addition, the HUM ED has an assigned cell phone that stays in the department, which is also notified in these circumstances (landlines are not common in Haiti). This is handed off to the physician leader on each shift.
In addition, internal hospital communications were identified as an area for improvement. HUM does not use pager technology, which is prohibitively expensive in Haiti and many resource-limited settings. Because MCIs require a hospital-wide response, initial assistance was requested by means of cell phone and/or in person runners, which are inefficient ways to notify large numbers of people. Now, notification protocols initially alert the ED chief, HUM Chief Medical Officer, and HUM Chief Operating Officer. WhatsApp groups for collective text messaging also solve other communication challenges and assist with further notification: 1 group links the ED chair, hospital leadership, and chairs of other departments, while another group links the nurse managers of all departments. Reference Rouhani, Marsh and Rimpel34 In the event of an MCI, ED or hospital leadership on these groups alert all parties, request resources or staff when needed, and communicate patient transfer needs. Ancillary departments, including lab and radiology, are also alerted by means of these systems so they can shift their focus to emergent studies.
Organization of Patients and Physical Space
After an MCI alert, staff from other departments (eg, internal medicine, surgery, pediatrics, pharmacy, and facilities) focus on moving existing patients out of the ED, fulfilling facility and supply needs, identifying back-up staffing for the operating rooms and inpatient wards in anticipation of patient surges, and facilitating communication back to the community. To create space for arriving patients, senior hospital staff create inpatient capacity and postanesthesia care unit (PACU) space through 3 strategies: (1) working with inpatient services to facilitate discharges and move patients awaiting discharge out of their inpatient beds, (2) contacting nearby facilities to arrange transfers of stable HUM inpatients to other facilities, and (3) working with inpatient services to move patients from the PACU to inpatient beds. This quickly creates space for arriving MCI patients.
To manage arriving patients, we had to address 3 key differences from high resource settings. First, scene triage is not feasible in our setting. MCI patients arrive to HUM primarily through informal transport mechanisms, such as in the back of pick-up trucks or on motorcycles, and a large number of patients with minor injuries arrive simultaneously with critically injured patients. Second, HUM is the only large hospital for the region, so patients cannot be distributed among multiple hospitals. Third, upon arrival to HUM, triage back to the waiting room is difficult, as it causes the perception of delayed or denied care.
To accommodate these challenges, we use a system of “quick look triage” on arrival accompanied by designated ED zones (Figure 1). As above, the ED is cleared of most existing patients as quickly as possible. Any remaining existing patients are moved into a separate portion of the ED containing 6 beds and/or zone 4 if needed. The 15 beds in the main ED are divided into 3 zones for new patients. An experienced emergency provider stands at the door as patients arrive and performs “quick look triage,” rapidly assessing likely acuity based on the patient appearance, perceived level of consciousness, and ability to ambulate. This provider assigns arriving patients to zones, trying to distribute moderate to high acuity patients evenly across zones 1-3. Less acute patients are triaged to chairs in the center of the ED or to zone 4 in the hallway outside the ED, which is turned into a patient care area using benches and stretchers provided by the central facilities team. Further triage is completed within the zones with mobile vital signs teams and ultrasound teams, as described below.

Figure 1. Schematic of HUM Emergency Department during MCI situations. During an MCI, pre-existing patients are preferentially admitted or transferred to the six gray beds. If there are too many patients for this area, patients too ill to sit in chairs are prioritized for these beds, and remaining patients moved to benches in zone 4. MCI patients enter at the red arrow, where eyeball triage is performed. High acuity MCI patients are triaged to Zones 1-3 (15 beds), and lower acuity patients to the central chairs or Zone 4. The area within the dark black lines is the normal emergency department patient care space. HUM = Hôpital Universitaire de Mirebalais; MCI = mass casualty incident.
To ensure success of this zone-based system, we identified physical surge space in the hallway adjacent to the ED (zone 4), then worked with our facilities team to ensure access to electricity, fans, benches, and beds to allow safe patient care in this area. Although such supplies may be accessed easily in higher resource settings, they frequently require advance planning in LICs.
Organization of Human Resources
We found organizing the influx of staff from other departments to be challenging, even though our MCI events necessitated a hospital-wide response. After the initial MCI events in which phone calls and runners were used to seek assistance, we restructured communications so requests for additional staff occur over WhatsApp groups, allowing real-time transmission of staffing needs and their fulfillment. In addition, we developed levels of MCI response depending on the anticipated number of patient arrivals. Each level corresponds with different standardized requests for human and other resources.
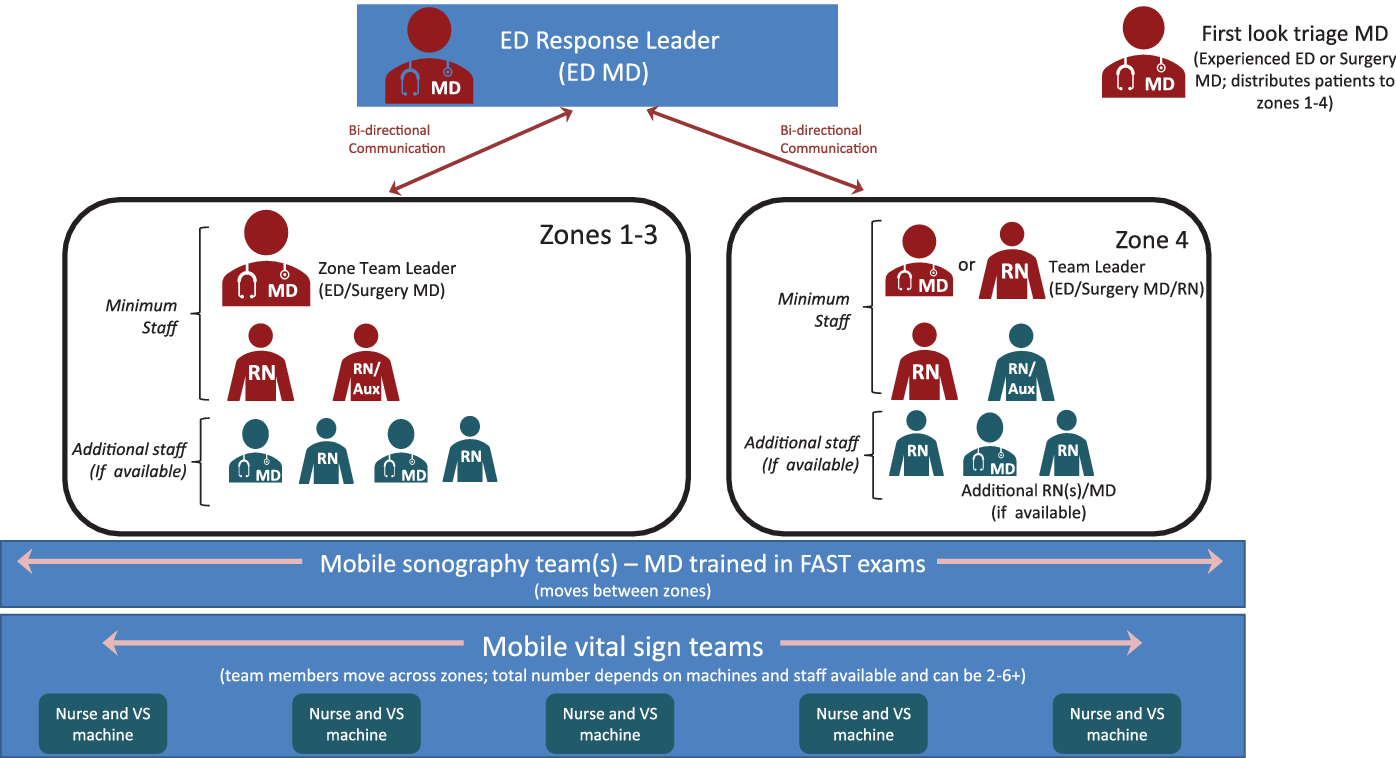
To organize staff in the ED, an overall response leader is designated. As above, the most experienced provider is assigned to quick look triage. All remaining staff are then distributed into zone teams (Figure 2). Although emergency staff are limited, we ensure each zone has an emergency physician or surgeon (resident or attending) to act as the “zone leader” and at least 1 ED nurse. We divide remaining staff, if any, as evenly as possible. We prefer ED or surgical staff familiar with trauma evaluations on the zone teams. Staff from the medical and pediatric services typically play 2 key roles: assisting with transfer of patients awaiting admission to other locations in the hospital and evaluating the continued arrival of routine nontrauma ED patients in the waiting room for stability. Zone leaders communicate with the overall response leader to prioritize patients for radiology, advanced interventions, and/or the operating room. Given limited staffing numbers that may be variable at different times of the day, we do not prescribe specific roles for staff on the zone teams. Depending on total staff in each zone, the zone leader may choose to assign staff to specific bed spaces or to designate roles across bed spaces such as primary assessment, medication administration, or IV access and labs.

Figure 2. Mass Casualty Staffing Diagram. Unless otherwise indicated, red icons represent ED or surgery staff; teal icons staff from any service. Staffing is the same in zones 1-3. If additional RN and/or MD staff are limited, ED and surgery staff are distributed preferentially to zones 1-3 for higher acuity patients. ED and surgery attending physicians and senior residents are prioritized for zone leaders, while junior residents and physicians from other services are distributed as needed within each team. When staffing does not permit a physician leader for zone 4 (lower acuity patients), an experienced ED RN is designated as the zone leader. RN = registered nurse; Aux = auxiliary nurse; MD = physician; ED = emergency department.
In addition to the teams within zones, we use 3 groups of mobile personnel to assist with overall patient evaluation and triage. We have several vital signs nurses that move within and between zones to assess vital signs, as there are a limited number of monitors with which to take vital signs. As the ED has only 1 ultrasound, a physician is designated to be in charge of mobile Extended Focused Assessment with Sonography in Trauma (E-FAST) ultrasounds Reference Bloom and Gibbons35 for trauma patients in all zones. Finally, depending on burden of emergent imaging, a physician is sometimes assigned to the radiology area to read images as they are completed (clinicians interpret their own studies at HUM).
Patient Identification
Initial MCI events at HUM suffered from misidentification of patients and delays in registration as registration staff were challenged by the need to register and assign unique medical record numbers to multiple patients simultaneously. As a result, patient lab specimens and/or radiology orders were sometimes labeled with bed numbers or misspelled names, making it difficult to match results to patients, particularly when patients changed bed locations. In addition, we struggled to distinguish between unidentified patients even after registration, as they all appeared in our system as “unknown, unknown” with unique (but often similar) medical record numbers.
We undertook a series of attempts to improve patient identification: ranging from a paper taped to each bed, identifying a patient as “unknown #X”, to writing a number taped onto each patient on arrival, to “named” unknown preregistrations and prelabeled charts similar to those developed after the Boston Marathon bombing (eg, – “unknown, mango”). Reference Landman, Teich and Pruitt36 Each of these attempts had their limitations, and none proved adequate in subsequent MCI events. With continued revisions, we now use 2- × 3-inch prelabeled patient stickers (Figure 3) that also document and communicate vital signs and ultrasound results among providers. The stickers are placed directly on every patient and can be moved to the patient’s chart after registration. The unique numbers on each sticker allow patient identification; registration staff can also compile a list of patients linking their sticker number to their name and medical record number after registration. Standard orders on the sticker empower nurses to initiate critical labs and treatments without specific authorization; additional orders can be endorsed by physicians as needed. The numbers on the sticker can be used for lab and radiology tests until medical record numbers are assigned. Additionally, the stickers make the mobile ultrasound and vital sign teams more efficient by identifying which patients already had their vitals or E-FAST completed, reducing duplication of efforts.

Figure 3. Pre-labeled patient identification stickers. These are placed directly on patients during MCI situations at HUM, and consist of a unique identifier, vital signs, Glasgow coma scale (GCS), E-FAST results, and initial orders for labs, medications or imaging. French version is used at HUM (left); English translation provided for reference (right). Locally “E-FAST Abdominal” refers to the abdominal and cardiac components of the typical E-FAST, and “E-FAST Lung” refers to the pulmonary components. Due to high rates of baseline non-vaccination for tetanus, all patients are treated with 1500 units of tetanus antitoxin in the presence of wounds; the tetanus vaccine is not available in the ED. E-FAST: Extended Focused Assessment with Sonography in Trauma; HUM: Hôpital Universitaire de Mirebalais; GCS: glasgow coma scale; MCI: mass casualty incident.
Supplies
In large MCI events, the ED rapidly exhausted its normal stock of key items, including gauze, sutures, pain medication, and tetanus prophylaxis. Similar to many hospitals in LICs, HUM does not have 24-h pharmacy or warehouse staffing. To allow rapid delivery of supplies, a back-up mass casualty cart was created with an extra supply of essential consumables and medications. Kept in a central locked room, the lead ED nurse has a key for access in MCI situations. In addition, an on-call system for warehouse staff was created for high-risk events, such as festivals or during elections. These low-cost solutions ensure availability of back-up supplies without needing to overstock supplies in the ED during routine operations, which would be cost- and space-prohibitive.
Security
Security and crowd control were identified as high priority needs during multiple MCIs and were addressed with several inexpensive changes. First, keypad and bolt locks were installed on ED doors to be used if needed. Security staff are positioned at entrances to control the flow of visitors and volunteer staff into and out of the ED. As needed, additional security staff are dispatched to control crowds around the ED during MCIs. Windows on doors are currently covered with thin paper to limit visibility in, with plans to add an inexpensive 1-way film over them to turn them into 1-way windows.
Staff Training
Despite frequent MCI events, we have found regular MCI protocol training necessary, including training on the identification stickers, supply carts, and notification procedures. In addition to periodic reminders at staff meetings, MCI training is now built into the ED residency curriculum and offers an opportunity to train and/or re-train both physicians and nurses on the protocols. Whenever possible, trainings are done in an interdisciplinary manner. A need to train other hospital staff has also been identified and planning for this is ongoing.
Discussion
MCI preparedness reduces morbidity and mortality in emergency situations, Reference Cooke, Chesters and Grier2 but most MCI protocols are designed for HICs. Reference Gates, Arabian and Biddinger3-Reference Aylwin, Konig and Brennan5 Locally relevant, low-cost protocols have the potential to decrease morbidity and mortality in low-resource settings, Reference Halpern, Goldberg and Keng11 where MCIs frequently occur. 1,Reference Odero, Garner and Zwi17,Reference Hyder, Norton and Perez-Nunez18,Reference Samuel, Akinkuotu and Villaveces20,Reference Odero, Khayesi and Heda21 The adaptations we made at HUM showcase specific strategies to efficiently mobilize existing infrastructure and personnel to respond to MCIs in LICs.
Many of the themes identified in our iterative process to develop MCI protocols reflect those described in the literature from high-resource settings, including triage, Reference Gates, Arabian and Biddinger3,Reference Aylwin, Konig and Brennan5 organization of patients and volunteers, Reference Halpern, Goldberg and Keng11,Reference Hammond37,38 patient identification, Reference Halpern, Goldberg and Keng11,Reference Landman, Teich and Pruitt36,Reference Chan, Killeen and Griswold39 security, Reference Golabek-Goldman12 and continuing education. Reference Bin Shalhoub, Khan and Alaska13-Reference Vincent, Berg and Ikegami15 These reflect the common challenges faced by health facilities when their resources are acutely stretched, but are often exacerbated in LICs. For example, MCI protocols that advise scene triage have begun to be recognized as ineffective even in high-resource settings, Reference Tsai, Huang and Su40 but pose a particular problem in resource-limited settings without trained prehospital providers. Reference Ozoilo, Pam and Yiltok41 As a result, based on our iterative process, we rely on “quick look triage” to distribute patients to zones on arrival. This is similar to START field triage, 42 but adapted to the facility level and multiple methods of patient arrivals.
Similarly, communication is a challenge in any MCI, but is further complicated by the lack of any prehospital system and the absence of pager systems and landlines. To address this, we engaged stakeholders to facilitate early hospital notification and use WhatsApp for group communication. These simple changes allow early involvement of hospital leadership and mid-level management and facilitate resource availability. In addition, WhatsApp groups assist with patient movements.
Our procedures rely on low-tech, low-cost planning and organization to address each of these issues. For example, the stickers we use for patient identification are an inexpensive way to reduce errors while also facilitating care through prepopulated orders and space for documentation of vital signs and ultrasound results. Some organizational changes, such as zone designation and planning for the staff surge are cost-neutral. In the absence of specific funding to build MCI systems, other hospitals in similar settings can use these procedures as the basis to improve their MCI responses without requiring additional resources.
Importantly, MCI protocol development at HUM required interdisciplinary input from varied stakeholders and multiple iterations before final protocols were adopted. For other institutions, as an initial step, we recommend early adoption of debriefs after MCI incidents and multi-disciplinary planning meetings with physician, nursing, and support staff, as well as with hospital administration. Protocol implementation requires communication with all ED staff and with other services, as MCIs can occur at any time.
Engagement of nonclinical services, such as security and facility teams, is particularly important. Some of our security improvements included inexpensive physical changes, such as bolt locks and window modifications, but many relied on re-organization and training of security staff. While our MCIs are rarely related to violence, we have continued to carefully evaluate security risks, particularly around national elections and ensuing political unrest. Through the debrief process, we have opted to preserve 1-way windows (rather than forgo windows entirely), as it allows for visibility of arriving patients and any evolving situation around the hospital.
There are several studies on development of disaster protocols in LICs. Reference Zafar, Jawad and Shamim16,Reference Umer, Sepah and Shahpurwala24-Reference Ouma, Maina and Thuranira28,Reference Ozoilo, Kidmas and Nwadiaro30-Reference Marsh, Rouhani and Pierre32 While MCI protocols can be a component of disaster preparedness, hospitals do not need to wait for the creation of a comprehensive disaster plan to implement MCI protocols. Similarly, an MCI protocol should usable even without all resources allocated under a disaster plan, given the frequency of MCIs from RTCs in LICs. If a hospital level disaster plan already exists, MCI protocols should be reviewed with it to ensure compatibility. For example, although we do not have sufficient staffing to implement a hospital incident command structure for all MCIs, a facility using an incident command structure for MCIs should ensure the systems are synergistic with any disaster plan incident command structure.
Several limitations of our protocols should be considered. Although our protocols have been successfully implemented, given limited resources and the unpredictable nature of MCIs we have not studied their impact on clinical outcomes. Second, our hospital is relatively well staffed compared with some in resource-limited settings. However, our solutions focus on the organization of staff and systems rather than an absolute number of human or material resources. Our approaches offer a starting point that facilities can adapt to their individual circumstances. Third, our guidelines focus only on the hospital-level response. Future projects should examine MCI protocols for communities and police in LICs in the absence of formal prehospital care. Finally, in our setting, MCIs are typically not due to violence. Different approaches may be required in environments with frequent MCIs from interpersonal violence.
Conclusions
Until road-traffic and other safety standards improve, MCIs will continue to occur with regularity in LICs. Context-specific MCI plans can alleviate the morbidity and mortality from these events and help health facilities function. We hope that our experience will help other hospitals to design cost-effective protocols to fit their operating environments.