Bilateral coronary ostial atresia, complicated with pulmonary atresia with an intact ventricular septum, is a very rare and critical anomaly. Here, we report an even rarer case of bilateral coronary ostial atresia in the setting of pulmonary atresia with ventricular septal defect.
Case
A 2148-g female infant was delivered vaginally at 38 weeks with a prenatal diagnosis of pulmonary atresia with ventricular septal defect and a hypoplastic right ventricle. Echocardiography revealed a large perimembranous ventricular septal defect, overriding of the bicuspid aorta, a hypoplastic dysplastic tricuspid valve (z-score, −2.9) opening into the right ventricle and the left ventricle (Fig 1), and pulmonary atresia. After prostaglandin E1 infusion was initiated, the initial decision was made to wait for Blalock–Taussig–Thomas shunt. The patient fed well and grew with minimal diuretics until 3 weeks there was ST-T change in the electrocardiography monitoring. Echocardiography could hardly delineate the origins of the coronary arteries. Subsequent cardiac catheterisation confirmed complete occlusion of the bilateral coronary ostia and a fistulous connection from the right ventricle to the coronary arteries (Fig 2a). The catheter easily passed through the ventricular septal defect from the right atrium to the left ventricular outflow tract (Fig 2b); nevertheless, both right and left ventriculography did not show significant interventricular shunt. The pressures were the same in both the ventricles. Balloon atrial septostomy was added at the end of the procedure. Additional echocardiography demonstrated the tricuspid valve was neither overriding nor straddling, though there was a right-to-left shunt both in systole and diastole through the ventricular septal defect and coronary artery fistulous communication (supplementary material 1). In order to improve oxygen saturation in the right ventricle and possibly coronary arteries other than balloon atrial septostomy, the aorta-to-right ventricular shunt was first discussed as an option; however, we decided to wait until she was 3 months old to create the bidirectional cavopulmonary connection because the shunt appeared to be unable to secure coronary perfusion for the patient in the presence of a large ventricular septal defect. However, she gradually developed left ventricular dilation and dysfunction, mitral regurgitation, and ventricular arrhythmia. She underwent urgent surgery on day 59 to maintain coronary perfusion by an aorta-to-right ventricular shunt. Cardioplegia was achieved from the right ventricle without a significant leak to the right atrium and left ventricle, implicating intraventricular connection between the right ventricular “apex” connecting to the coronary arteries and the left ventricle was effectively hampered by the complex tricuspid subvalvular apparatus. The operative finding revealed a dysplastic double-orifice tricuspid valve, presenting communication between the right atrium and both right ventricle and left ventricular outflow tract. We placed a shunt between the ascending aorta and the right ventricle apex, where cardioplegia was placed, using a 3.5-mm extended polytetrafluoroethylene tube and an aortopulmonary shunt using another 3.5-mm tube. She could not be weaned off cardiopulmonary bypass due to severe mitral regurgitation and left ventricular dysfunction and was therefore put on extracorporeal membranous oxygenator. Although additional mitral valvuloplasty on post-operative day 11 allowed her to be weaned off the mechanical support, mitral regurgitation rapidly worsened because of rupture of the sutured leaflets and she demised due to multiple organ failure 5 days later. Autopsy confirmed the diagnosis and revealed the presence of old localised infarction in the papillary muscle and fresh diffuse subendocardial ischemic lesion in the left ventricle but no significant transmural myocardial infarction.

Figure 1. Pre-operative apical four-chamber view demonstrating dysplastic tricuspid valve (TV) opening to both the hypoplastic right ventricle (RV) and left ventricle (LV) via ventricular septal defect (VSD). LA left atrium; RA right atrium.

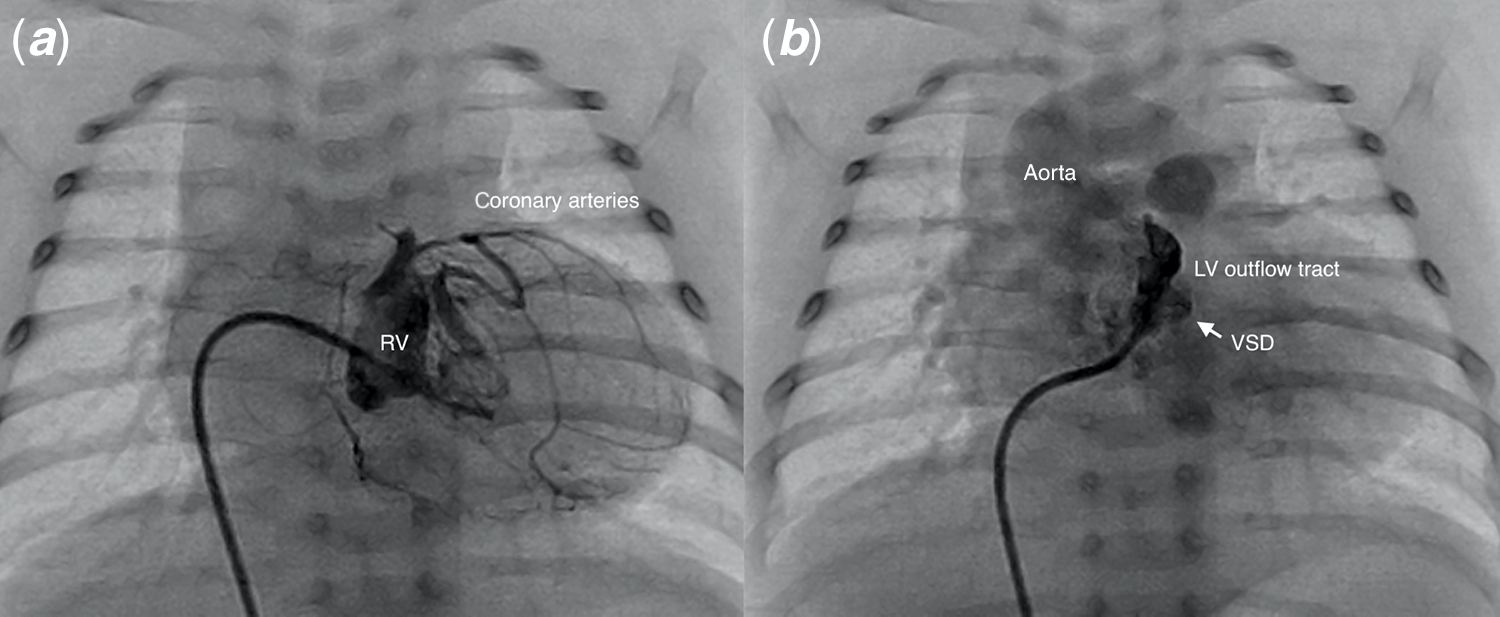
Figure 2. The right ventriculogram revealed bilateral coronary arteries originating from the right ventricle (RV), but no reflux of contrast was appreciated in the aortic root (a). The angiographic catheter easily passed from the right atrium to the left ventricular (LV) outflow tract through ventricular septal defect (VSD) (b).
Discussion
Bilateral coronary ostial atresia is known to be rarely associated with a hypoplastic RV in patients with pulmonary atresia with intact ventricular septum.Reference Wald, Juraszek, Pigula and Geva1,Reference Freedom, Anderson and Perrin2 While right ventricular hypertension is likely to be the main substrates of ventriculo-coronary arterial communication and right ventricle-dependent coronary circulation, our patient had a non-restrictive ventricular septal defect; hence, there was systemic systolic pressure in the right ventricle. To the best of our knowledge, this is the first case report on bilateral coronary ostial atresia complicated with pulmonary atresia with ventricular septal defect. It has been speculated that the double-orifice tricuspid valve creates a closed right ventricular apex where ventriculo-coronary communication develops, although right ventricular hypertension may not be a required factor for this type of coronary abnormality.Reference Olabiyi, Kearney, Krishnamurthy, Morales and Cabrera3
Heart transplantation would be the only option as a treatment in this cohort. Given the serious limitation of donor availability in Japan, it did not emerge as such. The coronary artery bypass or coronary artery transfer have been reported successful in neonates with coronary ostial occlusion after arterial switch operationReference Kitamura4; thus, it might have been another option although coronary perfusion is still unpredictable in the presence of significant coronary artery fistula to the right ventricle. Previously, we successfully saved a patient with bilateral coronary ostial atresia in the setting of pulmonary atresia with intact ventricular septum by creating an aorto-right ventricle shunt,Reference Sakurai, Sakurai, Ohashi and Nishikawa5 who has now reached Fontan completion. Even though there was a large ventricular septal defect, there was no significant interventricular shunt on ventriculography implying the possible establishment of coronary perfusion by an aorto-right ventricle shunt, which was also endorsed by the absence of transmural myocardial infarction at autopsy. The patient, however, was already experiencing significant ventricular dilation and dysfunction because of pulmonary overcirculation and low-oxygenated blood to the coronary circulation as well as mitral regurgitation because of inherent myocardial ischemia, all of which could have led to her death. The outcome may have been different if the surgery or decision to transplant had been undertaken earlier.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951121000779
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
None.