



Introduction
Emotion regulation (ER) strategies are defined as ‘processes individuals engage in to initiate, maintain, intensify, or eliminate mood states’ (Gross, Reference Gross1998; p. 275). Inability to effectively regulate mood is a common deficit present among individuals at high risk for developing affective disorders, such as bipolar disorder (Critchley, Reference Critchley2003). Staging models of mania risk (risk of developing bipolar disorder; e.g. Scott et al., Reference Scott, Marwaha, Ratheesh, Macmillan, Yung, Morriss and Bechdolf2016) highlight a number of cumulative risk factors. These include genetic factors (having a first-degree relative with bipolar disorder), age (peak age of onset for bipolar disorder is 18–25 years) and behavioural indices, such as emerging symptoms or elevated hypomanic personality traits. Hypomanic personality traits are characterised by extremes of confidence and energetic behaviours, frequently resulting in feelings of grandiosity and euphoria. Much of the literature investigating mania risk in non-clinical populations utilises behavioural measures of trait mania risk, such as the Hypomanic Personality Scale (HPS; Eckblad and Chapman, Reference Eckblad and Chapman1986).
Psychological models of mood swings and bipolar disorder (e.g. the integrative cognitive model; Mansell et al., Reference Mansell, Morrison, Reid, Lowens and Tai2007; Fig. 1) posit that the disturbances in mood regulation central to mania risk and bipolar disorder are exacerbated by the ways in which people think about and respond to how they are feeling (i.e. how they regulate their emotions). The link between putatively maladaptive emotion regulation strategies and both mania risk and bipolar disorder have been supported by research (for reviews of emotion regulation in mania risk and bipolar disorder, see Dodd et al., Reference Dodd, Lockwood, Mansell and Palmier-Claus2019; McGrogan et al., Reference McGrogan, Dodd and Smith2019). Emotion regulation strategies are often conceptualised as being either adaptive or maladaptive, in light of the association between the latter and psychopathology (not just bipolar disorder; Aldao, Reference Aldao2013). However, this distinction has been questioned in recent literature, with some suggesting that the (mal)adaptive value of a given strategy is dependent upon a number of moderating or mediating factors, such as situational demands (e.g. Aldao, Reference Aldao2013) and the desired outcomes and motivations behind a regulatory attempt (e.g. Mansell et al., Reference Mansell, Morrison, Reid, Lowens and Tai2007). Bonanno and Burton (Reference Bonanno and Burton2013) describe the tendency to categorise emotion regulation strategies as adaptive or maladaptive as the fallacy of uniform efficacy.

Figure 1. Integrative cognitive model of mood swing (Mansell et al., Reference Mansell, Morrison, Reid, Lowens and Tai2007).
To date, research investigating emotion regulation strategies and mania risk continues to produce mixed findings, particularly in relation to regulation of positive affect. For example, numerous studies with non-clinical samples have suggested that tendencies to dampen positive affect (i.e. engaging in mental strategies to reduce the duration and intensity of positive mood states; Feldman et al., Reference Feldman, Joormann and Johnson2008) are positively associated with high mood symptoms (e.g. increased feelings of happiness and elevated self-confidence; Kelly et al., Reference Kelly, Smith, Leigh and Mansell2016; Olofsson et al., Reference Olofsson, Boersma, Engh and Wurm2014; Verstraeten et al., Reference Verstraeten, Vasey, Raes and Bijttebier2012), whereas others have found a negative association (e.g. Feldman et al., Reference Feldman, Joormann and Johnson2008). Similarly, a number of studies have identified strong associations between positive rumination, defined as recurrent thoughts about positive self-qualities, affect experiences and favourable life circumstances (Feldman et al., Reference Feldman, Joormann and Johnson2008) and hypomanic personality (e.g. Dempsey et al., Reference Dempsey, Gooding and Jones2011; Steel, Reference Steel2016) while others have found no association (Raes et al., Reference Raes, Daems, Feldman, Johnson and Van Gucht2009). Dampening and positive rumination are also positively related to low mood symptoms (e.g. feelings of sadness and loss of interest) within non-clinical populations (e.g. Olofsson et al., Reference Olofsson, Boersma, Engh and Wurm2014; Thomas and Bentall, Reference Thomas and Bentall2002).
Contextual factors could explain mixed findings. Given that emotions are dynamic and often occur in response to external triggers, attempting to assess them in isolation of the contexts in which they occur significantly reduces the ecological validity of findings and limits understanding of ‘real life’ regulation processes (Aldao, Reference Aldao2013). Gratz and Roemer (Reference Gratz and Roemer2004) also state that ‘knowledge of the specific emotion regulation strategies used by an individual, in the absence of information about the contexts in which they are used, may provide little information about the individual’s ability to regulate her or his emotions effectively’ (p. 42). The integrative cognitive model of mood swings (Mansell et al., Reference Mansell, Morrison, Reid, Lowens and Tai2007), often applied to mania risk and bipolar disorder, suggests that factors such as life experiences influence how individuals respond to their internal states (see Fig. 1), this could also include an individual’s current environment. Several contextual factors have been highlighted as relevant to emotion regulation, such as the situational (e.g. what they are doing) and social (e.g. who they are with) settings an individual is in. The type and intensity of the emotion should also be considered as an influential factor in both the selection of the emotion regulation strategy (e.g. purportedly adaptive strategies are generally employed in response to less intense emotions while maladaptive strategies are typically used in response to more intense emotions; Sheppes et al., Reference Sheppes, Scheibe, Suri, Radu, Blechert and Gross2014) and the regulatory effort required, i.e. more intense emotions require more effort to regulate than less intense emotions (e.g. Barrett et al., Reference Barrett, Gross, Christensen and Benvenuto2001). A study by Dixon-Gordon et al. (Reference Dixon-Gordon, Aldao and De Los Reyes2015) assessed the use of emotion regulation strategies in response to high- and moderate-intensity negative emotions (i.e. sadness, anger and anxiety) across a range of stressful situations. Findings suggest that higher intensity emotions were associated with greater overall emotion regulation efforts, as well as greater endorsement of putatively maladaptive strategies, although this has yet to be explored in relation to the regulation of positive affect. Context should also be a key consideration when attributing adaptive and maladaptive value to emotion regulation strategies. For example, engaging in positive rumination may be considered appropriate and adaptive in situations where the desired effect is to increase positive emotions; however, where it would be more appropriate to downregulate mood (e.g. when attending a funeral or other sombre occasion), use of this strategy would be considered maladaptive.
A number of contexts have been highlighted as having particular relevance to bipolar disorder and mania risk. For example, heightened goal pursuit has been found to predict high mood symptoms in individuals with diagnosed bipolar disorder (Lozano and Johnson, Reference Lozano and Johnson2001). Gruber and Johnson (Reference Gruber and Johnson2009) also found that individuals high in hypomanic personality traits reported elevated levels of positive affect in relation to reward and goal attainment but displayed deficits in socially relevant positive emotions. This could suggest that individuals engage in different types of emotion regulation, depending on situational demands. It is therefore anticipated that use of purportedly maladaptive emotion regulation strategies in these contexts would be predictive of greater mood symptoms in those higher in mania risk.
Similarly, as mania risk is characterised by more intense positive and negative emotions, it is unsurprising that individuals with greater hypomanic personality traits report greater use of maladaptive strategies to upregulate (e.g. positive rumination) and downregulate (e.g. dampening) positive affect, whereas more passive and purportedly adaptive strategies such as savouring (i.e. attending to and appreciating positive experiences; Bryant and Veroff, Reference Bryant and Veroff2017) are less often reported. It is of particular theoretical relevance to assess this range of strategies as the negative emotion regulation literature frequently investigates use of both putatively adaptive (e.g. reappraisal) and maladaptive (e.g. catastrophising) strategies. However, the strategies used to regulate positive affect, particularly in relation to mania risk, are typically considered maladaptive, while savouring offers a more adaptive alternative.
To date, the associations between emotion regulation and context remains widely under-researched, despite suggestions that investigating them together offers the most valid insight into everyday emotion regulation processes (Aldao, Reference Aldao2013). Greater consideration of context could be useful in delineating if mood difficulties arise as a result of trait tendencies to use maladaptive emotion regulation strategies or if use of certain strategies in specific contexts are more unhelpful for those at risk. Such insight could help in identifying targeted areas for early intervention for individuals experiencing mood regulation difficulties. The proposed research therefore aimed to explore whether (i) tendencies to use specific emotion regulation strategies in response to moderate and high intensities of positive affect across different contexts (i.e. social and goal-related) were associated with mood symptoms (see Fig. 2), and (ii) whether tendencies to engage in these emotion regulation strategies across different contexts moderates the associations between mania risk and mood symptoms. To do this, this moderating role was tested for where both mania risk and trait use of emotion regulation strategies or context-specific use of strategies were related to mood outcomes.

Figure 2. Associations between trait and context-specific tendencies to use emotion regulation strategies and mood outcomes.
It was hypothesised that (H1) hypomanic personality would be positively associated with (a) trait-like and (b) context-specific tendencies to use maladaptive emotion regulation strategies (i.e. dampening and positive rumination) and not associated with use of adaptive strategies (i.e. savouring), (H2) high mood symptoms would be positively associated with (a) trait-like and (b) context-specific tendencies to engage in dampening and positive rumination but not savouring, (H3) low mood symptoms would be positively associated with (a) trait-like and (b) context-specific tendencies to engage in dampening and positive rumination but not savouring, (H4) hypomanic personality would be positively associated with (a) high mood symptoms and (b) low mood symptoms, and (H5) tendencies to use positive rumination and dampening would moderate the associations between hypomanic personality and mood, such that greater use of these strategies by those with more hypomanic personality traits would predict greater mood symptoms. The moderating role of dampening and positive rumination on the association between hypomanic personality and mood outcomes were tested for trait use of these ER strategies plus their self-reported use in the each of the four contexts.
Method
Participants
Based on 20 predictor variables (including hypomanic personality, mood symptoms and repeated administration of emotion regulation strategy use in different contexts), G*Power (Faul et al., Reference Faul, Erdfelder, Lang and Buchner2007) recommended a minimum sample size of n = 157 to detect a medium effect with an alpha level of .05. This sample size also surpassed the minimum requirement for sufficient power for moderation analysis (n = 77). Participants were drawn from a self-selected sample of respondents to social media advertisements and recruitment posters displayed around Northumbria University campus stating the following inclusion criteria: aged 18–25 years, no current diagnosis of mood disorder, and good understanding of written English. Psychology undergraduate students received course credits as compensation for their time and all participants were entered into a prize draw.
Three hundred and nine participants accessed the survey, and 135 participants were removed due to incomplete responses; 174 participants (mean age 20.77 years, SD = 2.2) provided sufficient data for analysis. Of this sample, 80.5% reported their gender as female, 18.4% male, 0.6% as other, and 0.6% preferred not to say. Eighty-one per cent were students (151 full time, four part time), 10.4% were employed and 0.6% unemployed. Eighty per cent of the sample described their ethnicity as White (n = 153), 1% as Black, 13% as Asian, 4% as mixed, and 2% as other.
Design
This study employed a correlational design, collecting data via an online self-report survey. Predictor variables include hypomanic personality and measures of emotion regulation in context (social- and goal-focused scenarios where participants have experienced moderate or high levels of positive affect). Outcome variables include current affect, and high and low mood symptoms.
Materials
An online survey hosted by Qualtrics included the following self-report measures.
Demographics
Demographic information (age, gender, occupation and ethnicity) was recorded using an in-house questionnaire.
Individual Difference measures
Hypomanic Personality Scale
Mania risk was quantified using the 20-item Hypomanic Personality Scale (HPS-20; Meads and Bentall, Reference Meads and Bentall2008). Items such as ‘I frequently find that my thoughts are racing’ and ‘When I feel an emotion, I usually feel it with extreme intensity’ are rated true (1) or false (0). The scale is valid for use in young adults (aged 18–25 years) as a useful indicator of mania risk, with high scores predicting future transition to bipolar disorder (Kwapil et al., Reference Kwapil, Miller, Zinser, Chapman, Chapman and Eckblad2000) and has demonstrated good internal reliability (α = .80; Meads and Bentall, Reference Meads and Bentall2008).
Affect
Positive and Negative Affect Scale
Current affect was measured using the 10-item international Positive and Negative Affect Schedule – Short Form (I-PANAS-SF; Thompson, Reference Thompson2007). Five positive affect words (e.g. inspired and determined) and five negative affect words (e.g. upset and afraid) are rated on a 5-point scale, from 1 (very slightly or not at all) to 5 (extremely) based upon the extent to which participants have experienced the emotions within the past few hours. Scores for the positive and negative subscales are totalled separately, with higher scores indicating higher levels of positive or negative affect.
Both subscales have been shown to have adequate internal reliability (positive affect = .78; negative affect = .76) and the whole measure shows good test–re-test reliability (.84; Thompson, Reference Thompson2007).
Altman Self-Rating Mania Scale
Current high mood symptoms were recorded using the 5-item Altman Self-Rating Mania Scale (ASRM; Altman et al., Reference Altman, Hedeker, Peterson and Davis1997). Symptoms are rated on a 5-pont scale from 0 (e.g. I do not feel more self-confident than usual) to 4 (e.g. I feel extremely self-confident all of the time) based upon participants’ experience over the previous week. Possible scores range from 0 to 20, with scores of 6 or higher indicating high probability of manic or hypomanic states.
The scale had demonstrated good validity and test–re-test reliability (Altman et al., Reference Altman, Hedeker, Peterson and Davis1997).
Center for Epidemiological Studies – Depression Scale
Current low mood symptoms were recorded using the Center for Epidemiological Studies – Depression Scale (CES-D; Radloff, Reference Radloff1977). Twenty items such as such as I could not get ‘going’ are rated on a 4 point scale from 0 (rarely or none of the time – less than 1 day) to 3 (most or all of the time – 5–7 days), based on the extent to which participants had experienced these symptoms over the past week. Possible scores range from 0 to 60, with higher scores indicating more low mood symptoms.
The CES-D is a reliable measure in populations with diagnosed depression (α = .64; Radloff, Reference Radloff1977) and is appropriate for use with young adults (Radloff, Reference Radloff1991).
Emotion regulation in context
Responses to Positive Affect Scale
Trait emotion regulation strategies were measured using items from the Response to Positive Affect Scale (RPA; Feldman et al., Reference Feldman, Joormann and Johnson2008). The original scale includes 17 items, such as ‘…think about how happy you feel’ and ‘…think I don’t deserve this’ which were rated on a 4-point scale from 1 (almost never) to 4 (almost always) based upon how frequently participants believe they respond to positive emotions in this way.
The RPA consists of three subscales: Dampening, Emotion-Focused Rumination, and Self-Focused Rumination. Further factor analysis recommends combining emotion-focused and self-focused subscales into a single construct of positive rumination, resulting in a two-dimensional measure (Nelis et al., Reference Nelis, Luyckx, Feldman, Bastin, Raes and Bijttebier2016). The scale is valid and has demonstrated acceptable internal consistency (α = .69–.79; Feldman et al., Reference Feldman, Joormann and Johnson2008).
In order to minimise participant burden, and following recommendations for the minimum number of items per subscale (Hair et al., Reference Hair, Anderson, Babin and Black2010), the top three loading items for each scale (Feldman et al., Reference Feldman, Joormann and Johnson2008) were used. Possible scores ranged from 9 to 36, with higher scores indicating greater use of ER strategies.
Ways of Savoring Checklist
Additional items were adapted from the Ways of Savoring Checklist (WOSC; Bryant and Veroff, Reference Bryant and Veroff2017). Items were taken from three subscales which represent the most passive form of savouring positive events: absorption (I thought only about the present – got absorbed in the moment), counting blessings (I reminded myself how lucky I was to have this good thing happen to me), and self-congratulating (I thought about what a good time I was having), resulting in a 3-item measure of savouring. Items were scored on a 5-item scale from 0 (strongly disagree) to 4 (strongly agree). Possible scores range from 0 to 12, with higher scores indicating greater endorsement of savouring.
Participants were then asked to provide brief descriptions of real-life social- and goal-relevant instances according to the following instructions:
Social context – ‘Please describe a time when you were in a social situation (e.g. with friends) and you felt moderate levels of positive emotion (e.g. happy, excited or enthused)’
Goal-relevant context – ‘Please describe a time when you were trying to achieve a goal or reward (e.g. pass a test) and you felt moderate levels of positive emotion (e.g. happy, excited or enthused)’
These instructions were also repeated for high-intensity positive affect in both contexts. Each combination of context and affect intensity were presented in a counter-balanced order. The same emotion regulation items from the RPA and WOSC were repeated for each of the four contexts thinking about the situation [you] described above, resulting in scores for dampening, positive rumination, and savouring in each context (high-intensity positive affect in a social situation, moderate-intensity positive affect in a social situation, high-intensity positive affect in a goal-focused situation, and moderate-intensity positive affect in a goal-focused situation).
Procedure
The survey was accessible on any internet-enabled device via a link contained in the recruitment adverts. Informed consent was obtained via an electronic consent form before participants were able to proceed with the survey. In order to ensure confidentiality, all participants were required to generate a unique code word, which was associated with their individual data set in place of any identifying information. Upon completion, participants were fully debriefed.
Participants who completed the survey were able to enter a prize draw for one of four £25 Amazon vouchers and undergraduate psychology students received participant credits as compensation for their time.
Analysis
Data were analysed using IBM SPSS Statistics 25. In instances where participants had two or fewer values missing on the HPS or CES-D, expectation maximisation was used to impute values.
Pearson’s correlations were conducted to investigate relationships between hypomanic personality, affect, mood symptoms and emotion regulation strategies.
A series of hierarchical multiple regressions were conducted using 1000 sample bootstrapping to assess whether predictor variables made unique contributions to outcome variables (i.e. high mood and low mood symptoms). Variables were added as potential predictors if they were significantly associated with the outcome being tested in that model (Fig. 2). Context-specific emotion regulation strategies were entered into Step 1, trait measures of emotion regulation and hypomanic personality were entered into Step 2, and current affect and mood symptoms were entered into Step 3 to assess whether context-specific and trait emotion regulation still predicted outcomes when controlling for these measures. For each model, the assumption of no multi-collinearity was satisfied, all tolerance statistics were >.02 and variance inflation factors were not substantially >1 (Field, Reference Field2013).
Where hypomanic personality and an emotion regulation strategy were both uniquely associated with high or low mood symptoms, moderation analyses were conducted using PROCESS (Hayes, Reference Hayes2012) model 1 to investigate if use of emotion regulation strategies moderate the relationship between mania risk and mood symptoms (see Fig. 3).

Figure 3. Moderation analysis between mania risk, emotion regulation and mood outcomes.
Results
Before analysis, the distributions of all scales were examined. All outcome variables were positively skewed: HPS (skewness statistic = .25, SE = .18), ASRM (skewness statistic = .53, SE = .18) and CES-D (skewness statistic = .89, SE = .18). This is consistent with expectation, as few participants from a non-clinical sample would be likely to be at high risk of mania, or exhibit clinically significant levels of both mania and depression symptoms. As the distribution of these variables reflected the expected population level distribution and correlational analyses are robust with respect to skew, variables were not transformed prior to analysis.
Descriptive statistics are shown in Table 1 (n = 174).
Table 1. Descriptive statistics for mania risk, mood symptoms and emotion regulation measures
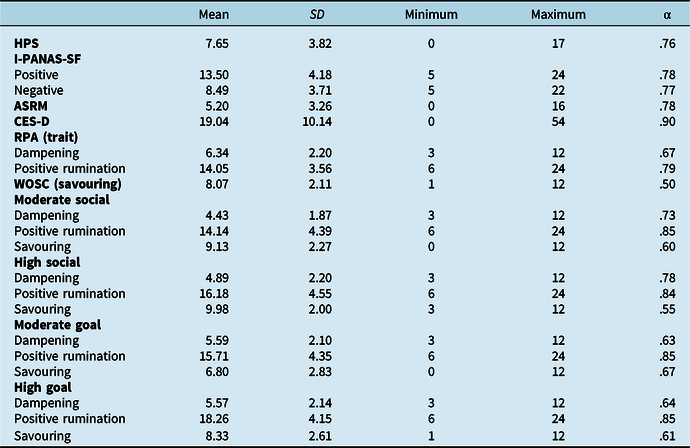
HPS, Hypomanic Personality Scale; I-PANAS-SF, International Positive And Negative Affect Schedule–short form; ASRM, Altman Self-Report Mania scale; CES-D, Center for Epidemiologic Studies Depression Scale; RPA, Responses to Positive Affect Scale; WOSC, Ways of Savoring Checklist.
Associations between hypomanic personality, affect, mood symptoms and emotion regulation strategies
Table 2 displays Pearson’s correlations for hypomanic personality, affect, mood symptoms and emotion regulation strategies.
Table 2. Correlations between hypomanic personality, emotion regulation strategies and current affect

HPS, Hypomanic Personality Scale; I-PANAS-SF, international Positive And Negative Affect Schedule–short form; ASRM, Altman Self-Report Mania scale; CES-D, Center for Epidemiologic Studies Depression Scale; WOSC, Ways of Savoring Checklist. *p < .05, **p < .001.
Hypomanic personality was positively associated with both current high and low mood symptoms. HPS was also positively related to trait dampening and savouring of high-intensity positive affect goal-focused contexts. Positive rumination was related to hypomanic personality across trait and all context measures.
Current high mood symptoms were positively associated with positive affect, and negatively associated with current negative affect and low mood symptoms. High mood symptoms were also associated with trait positive rumination as well as positive rumination on moderate- and high-intensity positive affect in social contexts and moderate intensity positive affect in goal-focused contexts.
Current low mood symptoms were negatively associated with positive affect and positively associated with negative affect. Low mood symptoms were also positively related to trait dampening and dampening high- and moderate-intensity positive affect in social contexts. A negative correlation was present between low mood symptoms and positive rumination on both high- and moderate-intensity positive affect in goal-focused contexts.
Trait dampening was positively associated with use of dampening across all contexts. Trait positive rumination was positively associated with use of positive rumination across all context measures, as well as trait savouring and savouring of moderate-intensity positive affect in social contexts and high- and moderate-intensity positive affect in goal-focused contexts. Trait savouring was positively associated with use of savouring and positive rumination across all contexts, and dampening of moderate-intensity positive affect in goal-focused contexts.
Table 3 displays regression analysis between emotion regulation strategies, mania risk and mood symptoms.
Table 3. Regression analyses between hypomanic personality, emotion regulation strategies and current affect

HPS, Hypomanic Personality Scale; I-PANAS-SF, international Positive And Negative Affect Schedule–short form; ASRM, Altman Self-Report Mania Scale; CES-D, Center for Epidemiologic Studies Depression Scale; MS, moderate social; HS, high social; MG, moderate goal; HG, high goal. HPS R 2 = .069* for Step 1, ΔR 2 = .053* for Step 2, ΔR 2 = .166** for Step 3; ASRM R 2 = .066* for Step 1, ΔR 2 = .104** for Step 2, ΔR 2 = .133** for Step 3, CES-D R 2 = .144** for Step 1, ΔR 2 = .071* for Step 2, ΔR 2 = .254** for Step 3. *p < .05, **p < .001.
Is mania risk associated with trait and context-specific use of emotion regulation strategies and mood symptoms?
Hypomanic personality was entered as the outcome variable. Positive rumination on moderate- and high-intensity positive affect in social and goal-focused contexts and savouring high-intensity positive affect in goal-focused contexts were entered in Step 1 to test their unique association with mania risk prior to adding in trait dampening and positive rumination in Step 2. To control for current mood, high and low mood symptoms were entered in Step 3.
Step 1 produced a significant model (F 5,168 = 2.51, p = .03), accounting for 6.9% of variance in mania risk. Within this model, none of the context-specific emotion regulation strategies was a significant predictor. The model retained significance when trait measures of emotion regulation were added (F 7,166 = 3.31, p < .003) and accounted for a further 5.3% of variance, p = .008. In this model, trait dampening was the only significant positive predictor. Significance was also retained when controlling for mood symptoms (F 9,164 = 7.39, p < .001) and accounted for an additional 16.6% of variance, p < .001. In this model, current high and low mood symptoms were the only significant predictors, both of which were positively related with mania risk.
Does trait and context-specific use of emotion regulation strategies predict mood outcomes?
High mood symptoms
High mood symptoms were entered as the outcome variable. Positive rumination on moderate- and high-intensity positive affect in social contexts, and moderate-intensity positive affect in goal-focused contexts were entered into Step 1. Hypomanic personality and trait positive rumination were entered as predictors in Step 2. Current affect and low mood symptoms were entered into Step 3.
Step 1 produced a significant model (F 3,170 = 3.40, p = .009), accounting for 6.6% of variance in high mood symptoms. Within this model, none of the context-specific emotion regulation strategies was a significant predictor. The model retained significance when trait emotion regulation strategies and hypomanic personality were added (F 5,168 = 6.89, p < .001) and accounted for an additional 10.4% of variance, p < .001. In this model, hypomanic personality was the only significant positive predictor. Significance was also retained when accounting for current affect and low mood (F 8,165 = 8.88, p < .001), accounting for a further 13.3% of variance in high mood symptoms, p < .001. Within this model, hypomanic personality and positive affect were significant positive predictors, and low mood symptoms were significant negative predictors of high mood symptoms. As emotion regulation strategies were not significant predictors of high mood symptoms in this model, follow-up moderation analysis was not conducted.
Low mood symptoms
Low mood symptoms were entered as the outcome variable. Dampening of moderate- and high-intensity positive affect in social contexts, and positive rumination on moderate- and high-intensity positive affect in goal-focused contexts were entered as predictors in Step 1. Hypomanic personality and trait dampening were entered as predictors in Step 2. Current affect and high mood symptoms were entered as predictors in Step 3.
Step 1 analysis produced a significant model (F 4,169 = 7.11, p < .001), accounting for 14.4% of variation in low mood symptoms. Within this model, ruminating on high-intensity positive affect in social contexts was the only significant predictor and was positively associated with low mood. The model retained significance when trait emotion regulation strategies and hypomanic personality were added (F 4,167 = 7.61, p < .001) and accounted for a further 7.1% of variation in low mood symptoms, p = .001. Within this model, both hypomanic personality and trait dampening were significant positive predictors. Significance was also retained when controlling for current affect and high mood symptoms (F 9,164 = 16.05, p < .001), accounting for an additional 25.4% of variation in low mood symptoms, p < .001. Within this model, hypomanic personality, negative affect and trait dampening were significant positive predictors, while positive affect and high mood symptoms were significant negative predictors. As positive rumination was not a significant predictor of low mood in this model, follow-up moderation analysis was not conducted for this strategy.
Does use of emotion regulation strategies moderate between mania risk and mood symptoms?
Trait dampening
Table 4 displays moderation analysis between trait dampening, mania risk and low mood symptoms.
Table 4. Moderation analysis between trait dampening, hypomanic personality and low mood symptoms

HPS, Hypomanic Personality Scale; CES-D, Center for Epidemiologic Studies Depression Scale.
Trait dampening was investigated as a moderator between hypomanic personality and low mood symptoms (Fig. 3). Both hypomanic personality (t 3,170 = 2.27, p = .03) and trait dampening (t 3,170 = 4.07, p < .001) were significant positive predictors of low mood symptoms. The interaction between hypomanic personality and trait dampening was non-significant (t 3,170 = 1.22, p = .22), suggesting that the relationship between mania risk and low mood symptoms is not moderated by trait use of dampening.
Discussion
Investigations of emotion regulation in relation to mania risk have frequently examined only trait use of strategies, omitting the potential influence of context. This study aimed to examine whether (i) tendencies to use specific emotion regulation strategies across situational contexts predict mood symptoms and (ii) use of emotion regulation strategies moderate the relationship between mania risk and mood symptoms.
Correlations mostly displayed anticipated relationships between use of emotion regulation strategies, mania risk and mood symptoms. For example, use of positive rumination positively correlated with both mania risk and current high mood symptoms, providing further support for conclusions drawn by Feldman et al. (Reference Feldman, Joormann and Johnson2008) that individuals higher in hypomanic personality traits show tendencies to amplify positive affect, which in turn is also linked with increased high mood symptoms. Trait dampening was associated with both mania risk and low mood symptoms, consistent with previous research that has attributed dampening to the development of both high and low valence mood symptoms (e.g. Olofsson et al., Reference Olofsson, Boersma, Engh and Wurm2014). Also in line with previous findings, savouring, a more adaptive response to positive affect, was not associated with mania risk or mood symptoms. This was true for tendencies to use emotion regulation in general, as well as tendencies to use these strategies in response to differing intensities of positive emotion elicited in social and goal-relevant situational contexts.
Within regression analyses, mania risk and mood symptoms were predicted by trait measures of emotion regulation over and above context specific measures. However, for mania risk and high mood symptoms, trait emotion regulation strategies were no longer significant predictors of these outcomes when accounting for current affect and mood symptoms, contrary to H1 and H2. In partial support of H3, trait dampening remained a significant predictor for low mood symptoms, along with mania risk, current affect and high mood symptoms. Furthermore, in partial support of H4, mania risk was positively associated with both high and low mood symptoms. The relationship between mania risk and low mood symptoms was not moderated by trait dampening, contrary to H5, suggesting that both of these trait variables (personality style and propensity to use dampening) are potentially separate pathways to low mood.
This study is the first to consider the role of context and emotional intensity when investigating use of positive emotion regulation strategies in relation to mania risk and mood. Many of the anticipated relationships were not observed, potentially as a result of methodological limitations outlined below; for example positive rumination was not a significant predictor of mania risk or mood symptoms, contrary to much of the literature which has found strong associations between use of positive rumination and these outcomes (e.g. Carver and Johnson, Reference Carver and Johnson2009; Dempsey et al., Reference Dempsey, Gooding and Jones2011; Feldman et al., Reference Feldman, Joormann and Johnson2008). Additionally, contextual factors did not add to the prediction of mood outcomes, as observed in other studies (e.g. Dixon-Gordon et al., Reference Dixon-Gordon, Aldao and De Los Reyes2015; Johnson and Jones, Reference Johnson and Jones2009). Although the assessment of emotion regulation in personally relevant contexts should be considered a strength of the design, as acknowledged by Dixon-Gordon et al. (Reference Dixon-Gordon, Aldao and De Los Reyes2015), this study is not without limitations. Firstly, the sample consisted primarily of White, female students, many of whom were likely to be psychology undergraduates given the participation incentives available to this cohort, and may therefore have been familiar with some of the measures used and biased towards recognising the purpose of the study. These factors limit the generalisability of findings to other populations. Previous research has also reported gender differences in use of emotion regulation strategies. For example, females have shown greater tendencies to engage in rumination in response to negative affect compared with males (e.g. Zlomke and Hahn, Reference Zlomke and Hahn2010) and use of rumination has been linked to more low mood symptoms in females than males (Nolen-Hoeksema, Reference Nolen-Hoeksema2012). Future research should consider the potential confounding effects of gender differences when investigating responses to both negative and positive affect.
Additionally, the cross-sectional design limits insight into which strategies in which contexts predict subsequent mood symptoms. It also does not allow for inference about the direction of causality of the relationship between mania risk and emotion regulation difficulties. Furthermore, the retrospective recall of emotional situations and the strategies used in these situations relies on the assumption that individuals can accurately recognise and articulate these processes (while emotion regulation can also be automatic; e.g. Gao et al., Reference Gao, Chen, Long, Yang and Yuan2018). However, as no time frame was suggested for the scenarios that participants described (e.g. within the past month), it is possible that responses to the emotion regulation measures associated with each context were more similar to trait-like responses rather than an accurate reflection of the strategies used in each situation. Similarly, the associations between use of regulation strategies and affect were based upon measures of how individuals were currently feeling. It is therefore unsurprising that there were no associations between these variables as the scenarios recalled are removed from the participant’s current experiences. For these reasons, future research should employ experience sampling methods (ESM) that capture ‘real-time’ emotion regulation in situations while they are happening, and the direct influence on subsequent mood. ESM would identify if there are discrepancies between the strategies individuals believe they use in response to positive emotion, and those they actually report using. This would remove the need to remember past scenarios and accurately recall the strategies used, as the individual is stating how they are regulating their emotions in that moment. This can determine whether emotion regulation strategies are problematic (or not) across the board (i.e. they are maladaptive), or whether their influence on mood depends on the context the person is in. Future research should also aim to investigate how combinations of factors, such as how individuals appraise their current mood, and the situational context they are in may influence the desired outcome of a regulation attempt (e.g. to sustain, upregulate or downregulate current affect) and the strategies they choose to achieve this.
Findings from this study and recommended future research could contribute to the development of targeted interventions for individuals experiencing difficulties with positive affect regulation. Given that staging models include a range of criteria to identify those who are bipolar-at-risk (including age, genetic risk, emerging mood symptoms, etc.), it is suggested that preventative interventions that recognise emotion regulation (and dysregulation) as universal experiences and promote better emotion regulation would offer non-pathologising ways of supporting individuals experiencing these difficulties, whereas interventions for those with bipolar disorder are typically relapse-prevention focused and therefore not appropriate for use with individuals who have not yet experienced a clinically significant mood episode. Additionally, these findings provide further support for use of transdiagnostic interventions that emphasise emotion regulation (e.g. the Unified Protocol; Barlow et al., Reference Barlow, Farchione, Sauer-Zavala, Latin, Ellard, Bullis and Cassiello-Robbins2017) as well as highlighting that emotion regulation difficulties, particularly relating to use of dampening and low mood, can be problematic for mental wellbeing outside of diagnostic boundaries.
In conclusion, trait measures of emotion regulation were more predictive of mania risk and mood symptoms than context-specific measures, although this relationship was no longer apparent for mania risk and high mood symptoms when controlling for current affect and mood symptoms. Low mood symptoms were also predicted by trait dampening in response to positive affect, but the relationship between mania risk and low mood symptoms was not moderated by trait dampening. Contextual factors did not add to the prediction of mania risk and mood symptoms; however, the possible influence of context should not be discounted due to a number of methodological limitations present within this study. Future research should use more ecologically valid assessments to test theoretically based predictions about relationships between mania risk, mood and emotion regulation strategies.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of interest
None.
Ethics statements
This study was conducted in compliance with the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. Ethical approval was also obtained from the Department of Psychology at Northumbria University.








Comments
No Comments have been published for this article.