


Rheumatoid arthritis (RA) is an autoimmune disease characterized by chronic joint inflammation which can lead, in untreated patients, to bony erosion, joint destruction, and disability. Moreover, it can produce several important extra-articular manifestations such as lung and cardiovascular diseases, among others (Reference Patel and Moreland1). Patients with RA have an increased mortality rate compared with the general population, having also a reduced life expectancy by 3 to 10 years (Reference Carmona, Cross, Williams, Lassere and March2). The disease prevalence is 0.5 to 1.0 percent in Caucasian population, with women being affected up to three times more often than men, and with a peak onset at 30–55 years (Reference Silman and Pearson3).
The main treatment goal is to achieve remission or low disease activity, being the first-line treatment synthetic disease-modifying anti-rheumatic drugs (DMARDs). Methotrexate is the cornerstone of first-line treatment, but in not responding or intolerant patients it is possible to use leflunomide, sulfasalazine, or injectable gold. When treatment target is not achieved with synthetic DMARDs with or without glucocorticoids, the addition of biological DMARDs is recommended (Reference Smolen, Landewé and Breedveld4).
Alpha tumor necrosis factor antagonists (anti-TNF), adalimumab, etanercept, and infliximab, are the most used in clinical practice, and are currently included in the National Medicines Formulary (NMF) of Uruguay. On the other hand, rituximab and tocilizumab were subjected to evaluation for admission to the NMF. These drugs are monoclonal antibodies against the phosphoprotein CD20 and the interleukin 6, respectively.
The aim of this study was to evaluate the efficacy and safety of rituximab and tocilizumab compared with adalimumab, etanercept, and infliximab, in patients not responding to first-line treatment, and to compare the efficacy and safety of rituximab versus tocilizumab in patients not responding to anti-TNF therapy. At the time of conducting this health technology assessment report, we do not identify any systematic review answering these questions.
METHODS
A literature search of randomized controlled trials (RCTs), controlled clinical trials (CCTs) and Cochrane systematic reviews (SRs) was performed to evaluate efficacy and safety of rituximab and tocilizumab in patients not responding to first-line treatment (evaluating a second-line treatment), and in patients not responding to at least one anti-TNF (third-line treatment). When a Cochrane systematic review met the inclusion criteria it was updated, and when no studies comparing head to head biologic DMARDs were found, indirect comparisons including RCT with a placebo arm were performed.
Inclusion criteria for the studies included in the review are detailed above.
Type of Studies
We included all completed/updated/available Cochrane systematic reviews of biologic DMARDs for RA. RCTs or CCTs comparing rituximab or tocilizumab versus anti-TNFs, rituximab versus tocilizumab, biologic DMARD to placebo, biologic DMARD to methotrexate, or biologic DMARD plus methotrexate to methotrexate alone. The studies should have a follow-up period of at least 6 months. Studies with patients receiving another DMARDs treatment, nonsteroidal anti-inflammatory drugs, or corticosteroids provided on stable doses in both arms were included.
Types of Participants
Adult patients meeting the American College of Rheumatology (ACR) 1987 revised criteria for RA (Reference Arnett, Edworthy and Bloch5). Patients had to have evidence of being not responders to first-line treatment or to at least one anti-TNF.
Types of Interventions
Dosages considered for DMARDs and glucocorticoids were those specified at the full prescribing information of each drug. Specifically, for biologic DMARDs were considered the following dosages: (i) adalimumab, 40 mg every other week or 20 mg every week; (ii) etanercept, 25 mg twice a week or 50 mg every week; (iii) infliximab, 3–5 mg per kg of body weight every 8 weeks; (iv) rituximab, 2 doses of 1,000 mg each on days 1 and 15; (v) tocilizumab, 8 mg per kg of body weight every 4 weeks.
Types of Outcome Measures
The primary efficacy outcome was the proportion of patients achieving an ACR50 response. An ACR50 response represents a 50 percent improvement in tender and swollen joint counts plus a 50 percent improvement in three of the five following remaining core measures: patient and physical global assessments, pain, functional status, and an acute phase reactant. ACR20 and ACR70 were also included as outcome of efficacy and are defined analogously (Reference Felson, Anderson and Boers6).
Safety outcomes included were serious adverse events, serious infections, total adverse events and withdrawals due to adverse events.
Search Methods for Identification of Studies
Electronic databases including MedLine, The Cochrane Central Register of Controlled Trials, Clincialtrials.gov, LILACS, and additional unpublished data provided by the manufacturers, were reviewed.
Search terms and strategy used for adalimumab in MedLine were: (“adalimumab” OR “D2E7 antibody” OR “Humira” OR “Abbott brand of adalimumab”) AND (“Rheumatoid Arthritis”). For adalimumab, the time frame of the search was limited from 01/08/2004 to 01/05/2011 in order to update a Cochrane review.
The search was limited in MedLine by publication type as follows: Clinical Trial, Meta-Analysis, Randomized Controlled Trial, Clinical Trial Phase I, Clinical Trial Phase II, Clinical Trial Phase III, Clinical Trial Phase IV, Controlled Clinical Trial. The same criteria were used for the remaining drugs.
Searches in the electronic databases were performed between May 1 and July 1, 2011. Additionally, we performed a manual search for relevant literature cited in the included manuscripts, and for some studies we contacted the sponsor to request additional information. The same search terms and criteria were used for other electronic databases and for the remaining drugs.
Data Extraction and Analysis
Each study was independently reviewed by two reviewers (N.G., A.A.) to determine if the study met the predefined inclusion criteria. Disagreements on study eligibility were solved by discussion with a third reviewer.
Data were extracted by one reviewer (N.G.), and then double-checked independently by another reviewer against the original data source. Any discrepancies were resolved through consensus by both reviewers, returning to the original data source to confirm which value was correct.
Data were analyzed using an intention to treat model with the software RevMan 5.1.2. Dichotomous data were reported as relative risk (RR) and 95 percent confidence interval (95%CI), through Mantel-Haenszel method. A fixed effects model was used to calculate a pooled estimate of effect, when the I2 was less than or equal to 50 percent, and random effect model was used for I2 greater than 50 percent (Reference Higgins, Thompson, Deeks and Altman7).
Indirect treatment comparisons were reported as RR and 95%CI, using the ITC software from the Canadian Agency for Drugs and Technologies in Health (Reference Wells, Sultan, Chen, Khan and Coyle8), following the criteria specified in the guidance “Indirect Evidence: Indirect Treatment Comparison in Meta-Analysis” from the same Agency (Reference Wells, Sultan, Chen, Khan and Coyle9).
RESULTS
The search at the Cochrane Library identified four systematic reviews for adalimumab (Reference Navarro-Sarabia, Ariza-Ariza, Hernandez-Cruz and Villanueva10), etanercept (Reference Blumenauer, Cranney and Burls11), infliximab (Reference Blumenauer, Judd and Wells12), and tocilizumab (Reference Singh, Beg and Lopez-Olivo13). Therefore, each Cochrane reviews were updated and for rituximab was conducted a full systematic review.
The search identified 767 references from electronic databases that were evaluated for inclusion, based on title and/or abstract review. One hundred thirty nine potentially relevant references were included in the next stage and full texts were reviewed (Figure 1). The main reasons for exclusion were: non controlled trials, sub-analysis of RCTs and differences from the defined population. We also excluded trials that evaluate biologic DMARDs as first-line treatment, or recruited mixed population in first- and second-line treatment (Figure 1) (Reference Kremer, Blanco and Brzosko14 –Reference Maini, Clair and Breedveld27).

Figure 1. Flowchart of the trials selection process.
No head to head trials comparing biologic DMARDs meeting the inclusion criteria were found. Therefore, indirect treatment comparison method was used to compare rituximab and tocilizumab versus anti-TNFs in second line treatment, and rituximab versus tocilizumab in third line treatment.
Twenty-four RCTs were included in this systematic review with 6,357 participants; 3,450 treated with biological DMARD and 2,907 with standard care, with at least 6 months of follow-up (Reference Lipsky, van der Heijde and Clair28 –Reference Tak, Rigby and Rubbert-Roth46). With a follow-up of 12 months, a total of 1,000 and 926 patients were evaluated, for biologic DMARD and standard care, respectively (Reference Taylor, Steuer and Gruber29;Reference Ho-Youn, Soo-Kon and Yeong Wook40;Reference Quinn, Conaghan and O’Connor44;Reference Mease, Cohen and Gaylis47 –Reference Boers, Tugwell and Felson52).
The main demographic characteristics of participants included in the studies are shown in a Supplementary Table 1, which can be viewed online at http://dx.doi.org/10.1017/S0266462314000221. Some parameters like disease duration, number of swollen joints, number of tender joints and C-reactive protein, shows significant differences. Hence, results of the indirect comparison should be considered with caution.
The results for each biologic DMARD versus control treatment, in patients not responding to first-line therapy at 6 and 12 months of follow-up, are shown in Table 1. ACR20 meta-analysis at 6 months for adalimumab showed significant heterogeneity (I2 = 80 percent), apparently caused by the study performed by Weinblatt et al. (Reference Weinblatt, Keystone and Furst15). A similar situation was verified for ACR20 and ACR50 for infliximab, with I2 values of 70 percent and 61 percent, respectively. This heterogeneity could be produced by the study performed by Schiff et al. (Reference Schiff, Keiserman and Codding16), that recruited patients with higher disease activity. Although the meta-analysis presents a significant statistical heterogeneity, individual studies are consistent in showing an efficacy improvement. The same considerations could be made for ACR20 at 6 months for etanercept (I2 = 72 percent).
Table 1. Efficacy at 6 and 12 Months of Follow up, for Patients Not Responding to First-Line Treatment

Note. ACR20, percentage of patients achieving an ACR20 response; ACR50, percentage of patients achieving an ACR50 response; ACR70, percentage of patients achieving an ACR70 response; RR, relative risk; 95CI%, 95 percent confidence interval.
The indirect comparisons of rituximab and tocilizumab versus anti-TNFs are shown in Table 2 (second line treatment). Rituximab shows lower ACR50 and ACR70 response rate compared with etanercept, at 6 months of follow-up. Data for rituximab at 12 months follow-up were not considered, because only one study with eighty patients not responding to first-line treatment (forty in each arm) was found. Tocilizumab shows higher ACR70 response rate compared with infliximab, at 6 months of follow-up (Table 2).
Table 2. Indirect Comparisons between Rituximab and Tocilizumab versus Adalimumab, Etanercept, and Infliximab, in Patients Not Responding to First-Line Treatment
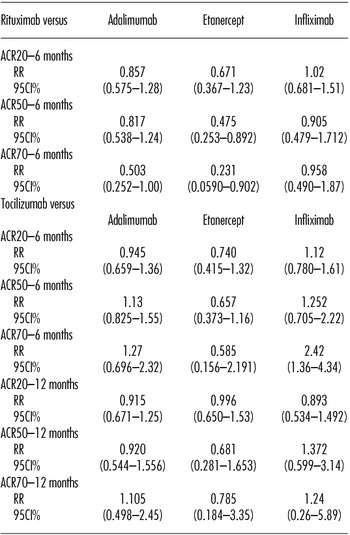
Note. ACR20, percentage of patients achieving an ACR20 response; ACR50, percentage of patients achieving an ACR50 response; ACR70, percentage of patients achieving an ACR70 response; RR, relative risk; 95CI%, 95 percent confidence interval.
Indirect comparisons between rituximab and tocilizumab in patients not responding for at least one anti-TNF (third line treatment), at 6 months follow-up were RR 1.79 (95%CI, 1.01 to 3.18), RR 1.49 (95%CI, 0.54 to 4.11), and RR 0.81 (95%CI, 0.11 to 6.05) for ACR20, ACR50, and ACR70, respectively.
Regarding safety, this review considers the results of a network meta-analysis of the Cochrane Collaboration that include RCTs, CCTs and open-label extension (Reference Singh, Wells and Christensen53). No significant differences were noted in serious adverse events according to whether the biologic drug was a TNF inhibitor or not, a TNF antibody or TNF receptor inhibitor or other kind of biologic drug, trial duration, or type of concomitant medication. For serious infections and total adverse events no significant findings were reported for the drugs evaluated. Adalimumab (OR 0.50; 95%CI, 0.32 to 0.78) and etanercept (OR 0.63; 95%CI, 0.41 to 0.95) were associated with significant fewer withdrawals due to adverse events compared with infliximab (Reference Grijalva, Chen and Delzell54).
CONCLUSIONS
All biologic DMARDs provide an improvement on efficacy outcomes in patients not responding to first-line treatment. However, rituximab showed a lower response at 6 months of follow-up for ACR50 (RR 0.48; 95%CI, 0.25 to 0.89), and ACR70 (RR 0.23; 95%CI, 0.06 to 0.90), compared with etanercept. Compared with adalimumab and infliximab, rituximab did not provide an improvement in efficacy. Moreover rituximab requires intravenous administration, which increases the patient´s risk and discomfort, in contrast to adalimumab and etanercept that are administered subcutaneously.
In patients not responding to first-line treatment, tocilizumab produces no additional benefit in efficacy compared with adalimumab and etanercept, however, an increase response in ACR70 at 6 months was verified compared with infliximab (RR 2.42; 95%CI, 1.36 to 4.34).
In patients not responding to at least one anti-TNF (third line), tocilizumab has a greater ACR20 response rate at 6 months compared with rituximab (RR 1.79; 95%CI, 1.01 to 2.18). The same comparisons for ACR50 and ACR70 were not statistically significant probably due to the low number of patients that achieved this kind of response, and therefore, reducing the number of patients available to compare these outcomes.
Regarding safety, infliximab seems to be less advantageous than adalimumab and etanercept, taking into account withdrawals due to adverse events. Additionally, a retrospective cohorts study that included 16,022 patients with rheumatoid arthritis, inflammatory bowel disease (IBD), and psoriasis, psoriatic arthritis, or ankylosing spondylitis, conclude that among patients with RA, infliximab was associated with a significant increase in serious infections compared with etanercept (adjusted hazard ratio, 1.26; 95%CI, 1.07 to 1.47) and adalimumab (adjusted hazard ratio, 1.23; 95%CI, 1.02 to 1.48) (Reference Grijalva, Chen and Delzell54). Besides, infliximab also require intravenous administration.
Taking into account efficacy, safety, route of administration and the availability of three anti-TNFs in the NMF, it seems appropriate to remove infliximab from the coverage.
Because tocilizumab showed a better efficacy with respect to infliximab at 6 months for ACR70, a possible reduction of withdrawals due to adverse events and a different mechanism of action compared with TNF inhibitors, we suggest the inclusion of tocilizumab for patients not responding to at least one anti-TNF. This suggestion is also supported by the indirect comparison between rituximab and tocilizumab, which shows superiority in ACR20 of the latter, with no differences in adverse events and route of administration. A possible use of rituximab would be to treat patients unresponsive to tocilizumab (fourth line treatment), however, no evidence support such prescription.
On the other hand, is important to note that the results obtained in this evaluation are based solely on indirect evidence, hence head to head trials are needed to determine the relative efficacy and safety between biologic DMARDs.
This evaluation proposes a different algorithm of treatment, taking into account a broad overview of efficacy and safety of biologic therapies available in the Eliminate the word “national” NMF for rheumatoid arthritis. However, this analysis does not include costs associated with the use of these drugs and, therefore, it is not possible to draw conclusions regarding the cost-benefit ratio of each strategy.
SUPPLEMENTARY MATERIAL
Supplementary Table 1: http://dx.doi.org/10.1017/S0266462314000221
CONTACT INFORMATION
Nicolás González-Vacarezza, MSc (gonzalezvacarezza@gmail.com), 18 de Julio 1892, PO box 11,200, Ministry of Public Health, Montevideo, Uruguay
Alicia Alemán, MD, 18 de Julio 1892, PO box 11,200, Ministry of Public Health, Montevideo, Uruguay
Graciela González, MD, Italia Avenue, PO box 11,600, National Institute of Rheumatology, Montevideo, Uruguay
Ana Pérez, MD, MSc, 18 de Julio 1892, PO box 11,200, Ministry of Public Health, Montevideo, Uruguay
CONFLICTS OF INTEREST
All authors declare no conflict of interest.





