



Case description
A 10-day-old neonate presented to our paediatric emergency department with respiratory distress. The chest x-ray showed homogenous opacification of the entire left lung. The child had an oxygen saturation of 90% in room air. She was started with intravenous antibiotics. She was referred for echocardiography to rule out CHD. Echocardiography showed a bipartite right ventricle. The inlet and outlet portions of the right ventricle were well formed, whereas the trabecular part was absent (Fig 1; Videos 1 and 2). The z score of the tricuspid annulus was more than +2, suggestive of a normal-sized annulus. The tricuspid valve morphology was normal, and there was no regurgitation. There was no right ventricular outflow obstruction. The child had a well-formed pulmonary trunk, which fed confluent pulmonary arteries. There was a large ostium secundum atrial septal defect with bidirectional shunting. On detailed evaluation, there was a diminutive right ventricular apex which was communicating with the left ventricle through a ventricular septal defect. There was no flow between the inlet portion of the right ventricle and diminutive apical portion of the right ventricle. Bubble contrast echocardiography also showed a lack of opacification of the right ventricular apex, whilst the right atrium and right ventricular inlet were densely opacified (Fig 2). There was a massive left-sided pleural effusion with consolidation of the left lung. The child did not have any features of congestive heart failure. The child was managed by the paediatric medicine team and was advised to follow up in the paediatric cardiology clinic after a month.
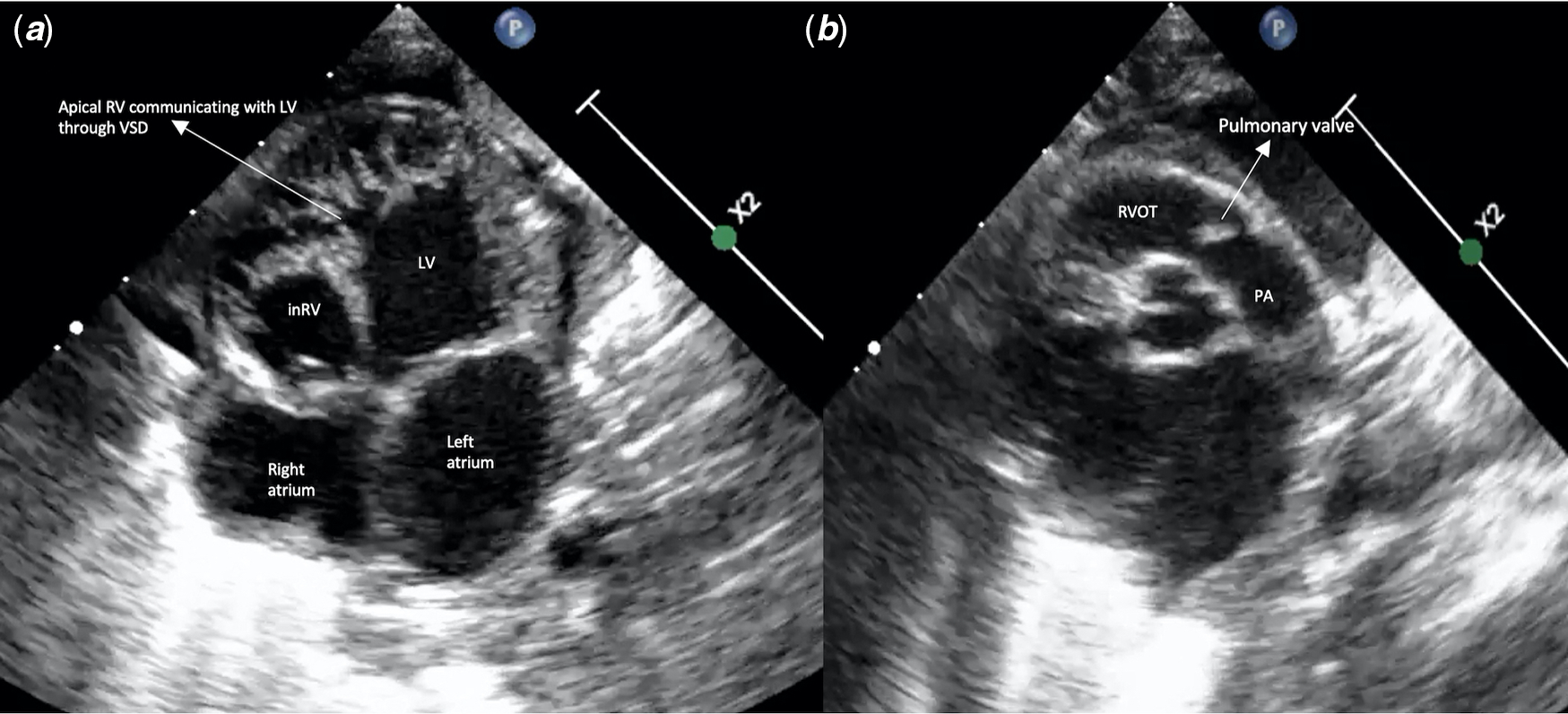
Figure 1. ( a ) Echocardiography in apical 4 chamber review showing a bipartite right ventricle (RV) with the apical trabecular portion communicating with the left ventricle (LV) through a ventricular septal defect (VSD). ( b ) Parasternal short axis view showing normal right ventricular outflow tract (RVOT) and pulmonary artery (PA). (inRV = inlet portion of right ventricle; apRV = apical trabecular portion of right ventricle).
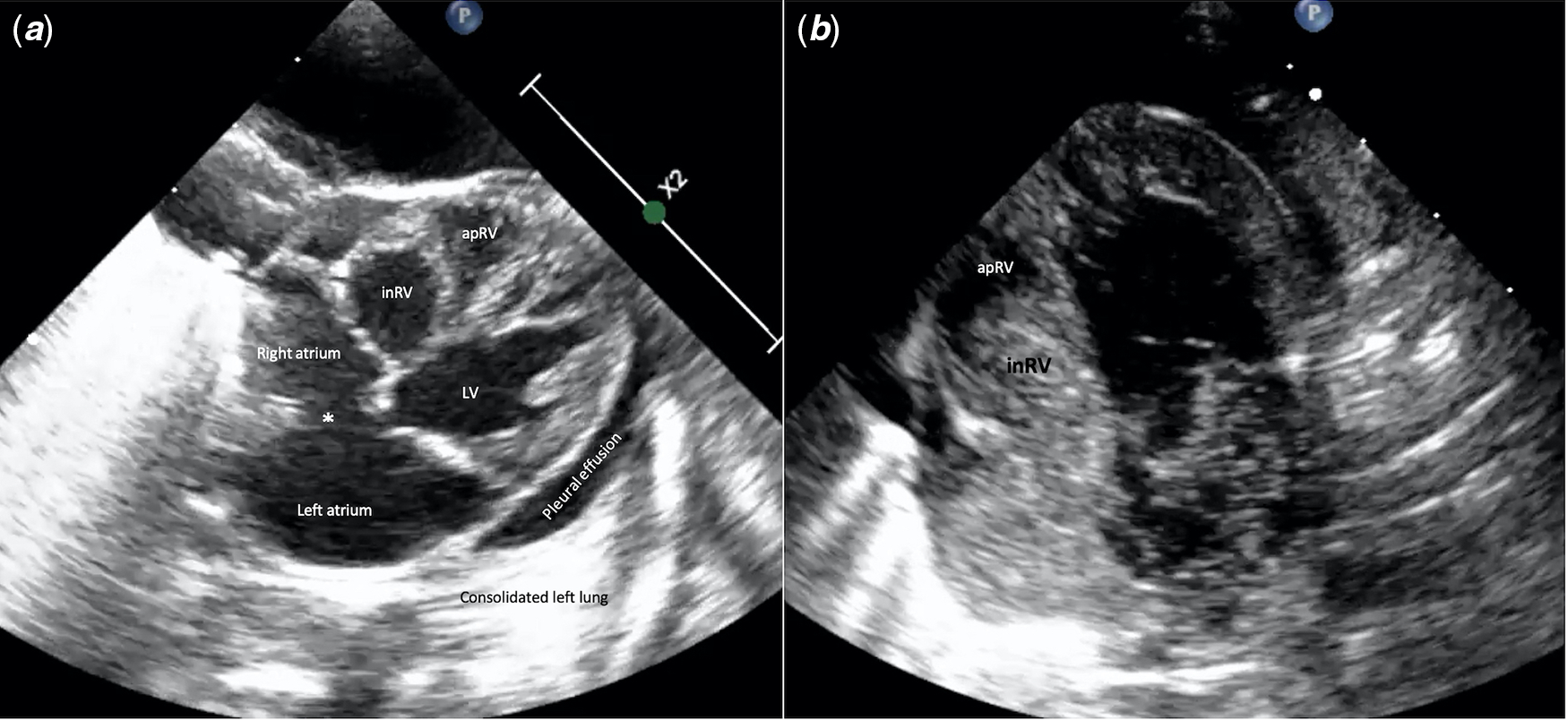
Figure 2. ( a ) Echocardiography in sub costal view showing large atrial septal defect (*) and separation of inlet and apical portions of the right ventricle (RV). LV = left ventricle. ( b ) Contrast echocardiography showing non opacification of right ventricular apex (apRV), whilst the right atrium, inlet portion of the RV and left atrium are opacified with bubble contrast.
Discussion
The right ventricle is classically divided into three components as initially proposed by Goor and Lillehei: inlet, outlet and apical trabecular components. Reference Ho and Nihoyannopoulos1 Embryologically, the apical trabecular component of the right ventricle is formed by ballooning from the inlet and outlet parts of the ventricular loop. It is the proximal part of the outflow tract that provides the ventricular outlets, while the inlets are also part of the primary heart tube. Reference Moorman, Webb, Brown, Lamers and Anderson2 The septomarginal trabeculation is an important component of the right ventricular septum. Along with septoparietal trabeculations and the papillary muscles of the tricuspid valve, the septomarginal trabeculation forms the trabecular component of the right ventricle. It is abnormal trabeculation that is responsible for the sequestration of the apical component from the inlet and outlet components of the right ventricle. Reference Moorman and Christoffels3,Reference Loukas, Housman, Blaak, Kralovic, Tubbs and Anderson4 The classically described double-chambered right ventricle occurs when an anomalous muscle bundle separates the outflow component from the rest of the right ventricle. There are multiple variants of double-chambered right ventricle described in the literature. Reference Restivo, Cameron, Anderson and Allwork5 The inlet portion of the right ventricle may be sequestered from the outlet and apical portions. Reference Zuberbuhler, Allwork and Anderson6 Other rare variants include the inlet and outlet components found in the absence of an apical component and a variant where the outlet component is committed to the left ventricle, simulating double-chambered left ventricle. Reference Beitzke, Anderson, Wilkinson and Shinebourne7,Reference Oldershaw, Ward and Anderson8 In our case, the apical component was sequestered from the outlet and inlet components, which in turn was committed to the left ventricle through a ventricular septal defect – to our knowledge a unique finding. On first look, the morphology appeared to be a bipartite right ventricle with a normal tricuspid and pulmonary valve. However, on detailed analysis, it was actually a unique variant of double-chambered right ventricle. This case is indeed a proof of the pudding that the ventricles are tripartite entities.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflict of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards as mentioned in the Helsinki Declaration of 1975, as revised in 2008.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951121002572



