


The growing interest in mindfulness has been responsible for the origin of several definitions and descriptions of this construct (Sauer & Baer, Reference Sauer, Baer and Baer2010). It is usually defined as the awareness that emerges through bringing one’s complete attention to the experiences occurring in the present moment, on purpose, in a nonjudgmental and accepting way (Kabat-Zinn, Reference Kabat-Zinn1994). Similarly, in their definitions of a mindful state, Brown and Ryan (Reference Brown and Ryan2003), and Marlatt and Kristeller (Reference Marlatt, Kristeller and Miller1999) share emphasis on the power of attention and awareness of the present moment. This way of paying sustained attention to the internal or external experience is also usually characterized by curiosity, acceptance and openness (Bishop et al., Reference Bishop, Lau, Shapiro, Carlson, Anderson, Carmody and Devins2004; Segal, Williams, & Teasdale, Reference Segal, Williams and Teasdale2002).
Although several authors reclaim the importance of studying mindfulness as an individual difference characteristic (Brown & Ryan, Reference Brown and Ryan2003), mindfulness as a training tool has been widely studied and the benefits of mindfulness-based interventions have been largely documented. Over the past few years, mindfulness has been incorporated into numerous psychological treatment programs for distinct populations, such as Mindfulness-Based Stress Reduction (Kabat-Zinn, Reference Kabat-Zinn1982, Reference Kabat-Zinn1990) developed for populations with a wide range of chronic pain and stress-related disorders, Mindfulness-Based Cognitive Therapy (Segal, Williams, & Teasdale, Reference Segal, Williams and Teasdale2002) designed to prevent depressive relapse in formerly depressed individuals, Dialectical Behavior Therapy (Linehan, Reference Linehan1993) for the treatment of borderline personality disorder, Relapse Prevention (Marlatt & Kristeller, Reference Marlatt, Kristeller and Miller1999) designed to target relapses in individuals with substance abuse, and Acceptance and Commitment Therapy (Hayes, Strosahl, & Wilson, Reference Hayes, Strosahl and Wilson1999) not specifically based in mindfulness meditation but making use of several of its strategies for a wide variety of populations. The majority of these studies on mindfulness-based interventions and other approaches that incorporate mindfulness as a component offer promising results, but also present serious methodological problems. Among these we have the lack of well-validated measures of mindfulness (Baer, Reference Baer2003; Baer, Reference Baer and Baer2010).
In line with this need, and given the fact that until the present moment there are no objective tests for measuring mindfulness, in the last few years several assessment tools have been designed to measure mindfulness, either as a state or as trait. All these forms of self-report questionnaires not only differ in their underlying mindfulness conceptualization and operationalization, but also in their content and factor structure (Baer, Reference Baer2011; Sauer & Baer, Reference Sauer, Baer and Baer2010). Among others, we have the Mindful Attention and Awareness Scale (Brown & Ryan, Reference Brown and Ryan2003), the Freiburg Mindfulness Inventory (Buchheld, Grossman, & Walach, Reference Buchheld, Grossman and Walach2001), the Kentucky Inventory of Mindfulness Skills (Baer, Smith, & Allen, Reference Baer, Smith and Allen2004), the Five Facet Mindfulness Questionnaire (Baer, Smith, Hopkins, Krietemeyer, & Toney, Reference Baer, Hopkins, Krietmeyer, Smith and Toney2006), the Revised Cognitive and Affective Mindfulness Scale (Feldman et al., Reference Feldman, Hayes, Kumar, Kamholz, Greeson and Laurenceau2005), the Philadelphia Mindfulness Scale (Cardaciotto & Herbert, Reference Cardaciotto and Herbert2005), and the Toronto Mindfulness Scale (Lau et al., Reference Lau, Bishop, Segal, Buis, Anderson, Carlson and Carmody2006; Davis, Lau, & Cairns, Reference Davis, Lau and Cairns2009).
The Mindful Attention and Awareness Scale (MAAS) is one of the earliest self-report instruments measuring the extent to which one acts with awareness in daily life. It was developed by Brown and Ryan (Reference Brown and Ryan2003) to assess individual differences in the dispositional quality of mindfulness, in particular the attention and awareness in the daily life present moment experience of individuals without meditation experience. This 15-item instrument addresses cognitive, emotional, physical, interpersonal and general domains with a single total score, where higher scores reflect greater mindfulness. In their definition of the construct, they intended to assess the “presence or absence of attention to, and awareness of, what is occurring in the present moment” (Brown & Ryan, Reference Brown and Ryan2003, p. 824). In contrast with the remaining measures, mindfulness at this trait-level is indirectly assessed on MAAS and individuals are asked to rate the items by answering how mindlessly they do things and behave in their daily life (in opposition to being mindful of the present moment).
The first studies of MAAS confirmed a single factor structure through factor analyses. The authors also found that this scale has strong psychometric properties, that it allows to differentiate between general population and highly experienced Zen Buddhist practitioners and, finally, that scores on MAAS improved over time during an 8-week mindfulness-based stress reduction program (Brown & Ryan, Reference Brown and Ryan2003). Besides that, mindfulness trait measured by MAAS is related to a variety of emotion regulation, behavior regulation, interpersonal and well-being phenomena (Brown & Ryan, Reference Brown and Ryan2003; Carlson & Brown, Reference Carlson and Brown2005).
Assessing the receptive awareness and attention to the present moment as a core characteristic of dispositional mindfulness, this scale has been validated with college and community samples (Brown & Ryan, Reference Brown and Ryan2003), as well as for cancer patients (Carlson & Brown, Reference Carlson and Brown2005). In an attempt to further validate the psychometric properties of the scale, MacKillop and Anderson (Reference MacKillop and Anderson2007) found that mindfulness trait measured by the MAAS is not related to gender; even though they could not confirm the single factor structure of the scale in men, supposedly as a function of their men sample size.
The MAAS has already been adapted and validated into Swedish (Hansen, Lunch, Hommam, & Wangby-Lundh, Reference Hansen, Lunch, Homman and Wangby-Lundh2009), French (Jermann et al., Reference Jermann, Billieux, Larøi, d’Argembeau, Bondolfi, Zermatten and van der Linden2009), and Spanish populations (Araya-Vargas, Gapper-Morrow, Moncada-Jiménez, & Buckworth Reference Araya-Vargas, Gapper-Morrow, Moncada-Jiménez and Buckworth2009). In the particular case of the Portuguese population, there is only one adapted mindfulness self-report measure, namely the Five Facet Mindfulness Questionnaire (Gregório & Pinto-Gouveia, Reference Gregório and Pinto-Gouveia2011). Given the importance of having adequate instruments to measure the construct of mindfulness for the Portuguese population, the benefits of comparing data for one mindfulness instrument across countries through cross-cultural research, and the fact that MAAS is one of the most frequently applied mindfulness measures, apart from its unidimensional nature and the fact of being a short instrument, the aim of this investigation was the study of the psychometric properties of the Portuguese version of the MAAS, namely the “Escala de Atenção e Consciência Plena”.
In the first study we describe the Portuguese version of the scale and replicate the original authors’ statistical procedures, through the analysis of the scale factor structure, with a confirmatory factor analysis. Then, in the second study, in a totally new sample with subjects also from the general population, we opted for briefly exploring if the same factor structure could be found. Also, we conducted cross-validation between both samples and also reliability’ analysis. Lastly in our third study, we investigate the convergent and discriminant validities of the Portuguese version of MAAS through its correlations with measures of several psychopathological constructs. More specifically we were interested in exploring the relationships between mindfulness and psychopathology and also some emotion regulation strategies.
Study 1: Confirmatory Factor Analysis (CFA)
Method
Participants
Participants in this study were 530 subjects from general population, with 306 (57.7%) undergraduate students recruited from the University of Coimbra (Portugal) and 224 (42.3%) subjects recruited from the general population in several institutions and corporations in the district of Coimbra, in Portugal. Eighty four per cent (84%) were females (n = 445), mean age 28.28 (SD = 13.37) and 16% (n = 85) males, mean age 35.37 (SD = 15.75). Seventy per cent (70%) of the subjects are single (n = 371). Three hundred and six (n = 306) were students (57.7%) and 21.3% of the general population subjects had middle class professions (n = 113). The participants years of educations mean was 15 (SD = 2.72).
Measures
All individuals completed a questionnaire that included demographic data and the Mindful Attention and Awareness Scale (MAAS: Brown & Ryan, Reference Brown and Ryan2003). The MAAS is designed to measure mindfulness as a trait, specifically the open and receptive attention to the present moment. The 15 items introduced by the following sentences: Below is a collection of statements about your everyday experience. Please answer according to what really reflects your experience rather than what you think your experience should be; are rated on a 6-point Likert scale ranging from 1 (almost always) to 6 (almost never). The total score can range from 15 to 90, and higher scores indicate more mindfulness.
MAAS was translated into Portuguese by a Psychologist and researcher experienced in translating English psychological literature. To help improve the content validity of the Portuguese version a Psychiatrist expert on mindfulness, both in research and training, reviewed the items translation and, finally, a bilingual translator back-translated it to English. At the end adjustments were made to the translation into Portuguese.
Procedure
As the original authors, in order to test for construct validity we conducted a Confirmatory Factor Analysis (CFA) of the internal structure of the Portuguese version of MAAS, with Maximum Likelihood (ML) estimator, through AMOS 17.0.
Results
The model tested in the CFA was defined as a single-factor model, according to the only factor found through the original author’s factor analyses. In the diagram, mindfulness was the hypothesized factor (latent variable) with its 15 variables (measured indicators) corresponding to all the MAAS original items. ML was the estimation method chosen in this statistical procedure, just as in the original study and since it is the most commonly used model-fitting procedure in CFA (Brown, Reference Brown2006).
A large class of omnibus tests exist for assessing how well models match the observed data. Chi-Square is a classic goodness-of-fit measure to determine overall model adequacy (Brown, Reference Brown2006), and in this first factor solution the Chi-Square was significant at p < .001, χ2(90) = 368,417. The Chi-Square test is widely recognized to be problematic (Jöreskog, Reference Jöreskog1969), because of being affected by several factors, especially by sample size (DeCoster, Reference DeCoster1998). For this reason it was expected that this test could lead to the rejection of the null hypothesis in a sample of 530 subjects, even in the presence of a possible appropriate factor model. However, the Normed Chi-Square of the solution, χ2/df = 4.09, designated to minimize the impact of sample size on the model Chi-Square, was in-between the author’s recommendations, which range from 2.0 (Tabachnick & Fidell, Reference Tabachnick and Fidell2007) to 5 (Wheaton, Muthen, Alwin, & Summers, Reference Wheaton, Muthen, Alwin and Summers1977).
The following fit index cut-off values were also used by the investigators to help determining overall goodness of fit: Comparative Fit Index [CFI] and Tucker Lewis Index [TLI] ≥ .90, which indicate a reasonable fit of the model (Bentler, Reference Bentler1990; Brown, Reference Brown2006; Kline, Reference Kline2005; Schumacker & Lomax, Reference Schumacker and Lomax1996); and Root-Mean Square Error of Approximation [RMSEA], which values ≤ .05 indicate close model fit and which values between .05 and .08 indicate reasonable error and an acceptable fit (Brown, Reference Brown2006; Browne & Cudeck, Reference Browne, Cudeck, Bollen and Long1993; Hu & Bentler, Reference Hu and Bentler1999). The model fit summary showed that the indicators of global adjustment of this model were at an acceptable level, more specifically: CFI = .92, TLI = .90 and RMSEA = .08 [CI90 ranges from .07 to .09].
A closer look to the indicators for local adjustment allowed us to identify one item (MAAS 13) with the lowest standardized regression weight or factor loading (.26); the higher residual error (.93) indicative of being the item with the largest unexplained part by the factor; and also the lowest value of R 2 (.07), indicating very low explained variance by the proposed model (Kline, Reference Kline2005). Accordingly, we decided to eliminate item 13 from the model, considering statistical motives as follows: it was the item with the lowest factor loading and the lowest value on R2, therefore acting as an item without the essential qualities for being kept in the scale structure of the Portuguese version of MAAS.
In summary, given the low adjustment indices obtained in the CFA, our first hypothesis that the model of the 15-items version would fit the data was not supported and so we removed item 13 (“I get so focused on the goal I want to achieve that I lose touch with what I’m doing right now to get there”) from the model based on the assumption of improving the adjustment and validity of the model. Consequently, item 13 was not considered vital for the Portuguese version of MAAS, and we calculated the model once again with 14 items of the MAAS, as is shown in Figure 1.

Figure 1. Path diagram of the single-factor model of the Portuguese version of MAAS found in Study 1 (N = 530).
The elimination of item 13 allowed a reduction to some extent on the Chi-Square value and also a slight improvement on one of the other adjustment indices. The Chi-Square fit of the model to the covariance matrix was poor, χ2(77) = 335.466, p < .001. However, we continued our analysis given that, as said, the Chi-Square is highly sensitive to the sample sizes and very readily reaches significance with large sample sizes (such as the one in this study), even when all other indices indicate a good fit (Jöreskog, Reference Jöreskog1969; DeCoster, Reference DeCoster1998). The Normed Chi-Square for this solution was 4.36, again located in the already cited recommended range (Tabachnick & Fidell, Reference Tabachnick and Fidell2007; Wheaton et al., Reference Wheaton, Muthen, Alwin and Summers1977).
The overview of the global adjustment indices for this second solution maintained an acceptable global model fit, CFI = .92; TLI = .91; RMSEA = .08; CI= .07 to .09, since all are above the recommended cut points (Bentler, Reference Bentler1990; Brown, Reference Brown2006; Browne & Cudeck, Reference Browne, Cudeck, Bollen and Long1993; Hu & Bentler, Reference Hu and Bentler1999; Kline, Reference Kline2005; Schumacker & Lomax, Reference Schumacker and Lomax1996). Hair, Black, Babin, Anderson, and Tatham (Reference Hair, Black, Babin, Anderson and Tatham2005) acknowledge the fact that, in recent years, several authors recommended the use of higher cut-off values for relative fit indices (.95), but they provide some guidelines for using different fit indices in different model situations. Specifically, for a sample with more than 250 subjects and observed variables between 12 and 30 (the case of this study with 530 participants and 14 variables), the authors point that: significant p-values are expected; either one of CFI or TLI should be equal or above .92; and finally, that RMSEA scores should be less than .07 (what is met for the lower CI of RMSEA). Since all these criteria are met in the results of the CFA of our model, we can conclude about the acceptability of values obtained in the performed statistic.
Since the above cited goodness-of-fit indices provided a global descriptive summary of the ability of the model in study, to support the conclusion of a good-fitting model Table 2 presents more specific information about the acceptability and utility of this solution. First, all the items factor loadings situate in a range from .42 to .84, around Tabachnick and Fidell’s criteria for a fair correlation (2007). Regarding the local adjustment indices (Figure 1; Table 1) we also observed that the coefficients of determination (R 2 ) of all the items have acceptable values, all between .17 and .69. Additionally, the corrected item-total correlations showed adequate values (all above .42), confirming the adequacy of the items to the measure and its internal consistency.
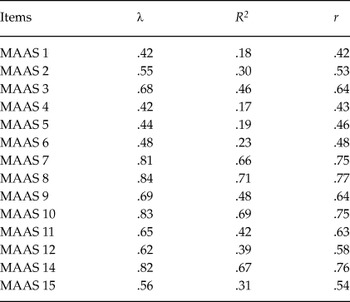
Table 2. Standardized Regression Weights (λ), Squared Multiple Correlations (R2), and Item-Total correlations (r) for the 14-items MAAS Portuguese version considered on the analysed model in Study 2 (N = 614)

Table 1. Standardized Regression Weights (λ), Squared Multiple Correlations (R2), and Item-Total correlations (r) for the 14-items MAAS Portuguese version considered on the analysed model in Study 1 (N = 530)
The Cronbach’s alpha coefficient for this 14-item version of the Portuguese MAAS was calculated and was of .90, which points once more to an excellent level of internal consistency (Nunnally, Reference Nunnally1978).
The final scores for the Portuguese version of MAAS were 4.32 as the mean score for the general population sample (SD = .89) and a mean score of 4.08 (SD = .81) for the students sample, quite similar to those reported by the original authors of the instrument, since normative information on the mindfulness trait measured by MAAS shows that community samples have a mean score of 4.20 (SD = .69) and college students a mean score of 3.83; SD = .70 (Brown & Ryan, Reference Brown and Ryan2003).
Study 2: Confirmatory Factor Analysis (CFA) and Cross-Validation Statistics
Method
Participants
Six hundred and fourteen (N = 614) subjects, with 224 (36.59%) undergraduate students recruited from the University of Coimbra at Portugal and 390 (63.5%) subjects recruited from the general population participated in this study. Four hundred and thirty nine (n = 439; 71.5%) were females, and 175 (28.5%) were males. Sixty per cent of the subjects were single (n = 366). Two hundred and twenty four (n = 224; 36.5%) were students and 38.4% (n = 236) of the general population subjects had middle class professions. The participants mean years of education is 14 (SD = 3.05).
Measures
Mindful Attention and Awareness Scale (MAAS: Brown & Ryan, Reference Brown and Ryan2003) was already described in Study 1.
Procedure
In order to continue the investigation of the latent structure of the Portuguese version of the MAAS, in this study we performed another Confirmatory Factor Analysis (CFA) in a new sample, through AMOS 17.0, again with Maximum Likelihood (ML) estimator as the original authors did.
Results
Once more, with the same estimator (ML) we tested the same initial model in the CFA –a one-factor model comprising 15 items. The first indicator used to test for the global adjustment of the model under examination was the Chi-Square, that again showed to be statistically significant, χ2(90) = 371.989; p < .001, and an expected value given the size of our sample (N = 614). Nevertheless, the Normed Chi-Square for this solution (χ2/df = 4.13) was found to be an adequate value situating in the reference range above-mentioned (2 to 5; Tabachnik & Fidell, Reference Tabachnick and Fidell2007; Wheaton et al., Reference Wheaton, Muthen, Alwin and Summers1977).
Both the Comparative Fit Index, CFI = .92, and the Tucker-Lewis Index, TLI = .90, were found to be indicative of a good model fit accordingly to the minimum value of .90 suggested by several authors (Brown, Reference Brown2006; Hu & Bentler, Reference Hu and Bentler1999). Finally, the Root-Mean Square Error of Approximation, RMSEA = .07; CI = .06 to .08, and once more the value obtained confirmed the acceptable fit of the solution under study, according to the interval [.05 to .08] suggested as representing a reasonable error and acceptable fit (Browne & Cudeck, Reference Browne, Cudeck, Bollen and Long1993; Hu & Bentler, Reference Hu and Bentler1999).
Regarding the local adjustment indices we found similar results to those reported in Study 1: again item 13 does not reach the minimum criteria to be kept in the solution. More specifically, it has the lowest standardized regression weight (.30), the lowest squared multiple correlation value (.09) and the highest residual error (.91).
Although the solution obtained an acceptable level of global adjustment for the solution, these weaknesses presented by item 13 lead us to the decision of removing item 13 from the solution and conducting a new confirmatory factor analysis on a 14-items model to investigate if it was possible to get to a more robust model for the internal structure of the Portuguese version of MAAS (Figure 2).

Figure 2. Path diagram of the single-factor model of the Portuguese version of MAAS found in Study 2 (N = 614).
The global adjustment indices after the elimination of item 13 from the solution under investigation come as follows: χ2(77) = 348,070; p < .001; Normed Chi-Square = 4.52; CFI = .92; TLI = .90; RMSEA = .08; RMSEA CI = .07 to .08. Having in consideration the author’s recommendations already mentioned for all the indices, it is possible to affirm the goodness of fit of the 14-items solution (Bentler, Reference Bentler1990; Brown, Reference Brown2006; Browne & Cudeck, Reference Browne, Cudeck, Bollen and Long1993; DeCoster, Reference DeCoster1998; Hair et al., Reference Hair, Black, Babin, Anderson and Tatham2005; Hu & Bentler, Reference Hu and Bentler1999; Jöreskog, Reference Jöreskog1969; Kline, Reference Kline2005; Schumacker & Lomax, Reference Schumacker and Lomax1996; Tabachnick & Fidell, Reference Tabachnick and Fidell2007; Wheaton et al., Reference Wheaton, Muthen, Alwin and Summers1977).
Regarding an item-level statistics (Figure 2; Table 2), the minimum standardized regression weight obtained was .42, once more close to a criteria for meaningful correlation considered fair (Tabachnick & Fidell, Reference Tabachnick and Fidell2007); and also the squared multiple correlations presented acceptable values (ranging from .18 a .67). To finish the corrected item-total correlations ranged from .43 to .74, indicating that all items are linked to the latent variable of mindfulness which MAAS is designed to measure.
The reliability analysis of the scale for this sample revealed an internal consistency coefficient of .89, similar to the one reported in Study 1 (.90) and stated by the original authors (.84), pointing to a very good level of internal consistency (Nunnally, Reference Nunnally1978).
After concluding about the factorial validity of the MAAS separately for two general population groups, and having two independent samples drawn from the same population, we were now interested in exploring whether or not the 14-items measurement model of mindfulness found in both studies could be considered group-invariant. In other words, we wanted to investigate if we could conclude about the equivalence of models found for the factorial structure of MAAS, this is, to cross-validate this structure.
Findings from the previous analyses yielded one prior model (with 14-items) identical for both samples, what is not the same that concluding about the equivalence of the underlying factor structure. When testing for the invariance it is possible to explore it in two different dimensions: at a structural level (if there is equivalence between factor correlations) and at a measurement level (that has to do with factor loadings equivalence) (Byrne, Reference Byrne2010).
Given that MAAS is a one-dimensional measure, we only tested for the measurement invariance, specifically for metric invariance, that allows investigating if the subjects from our two samples interpreted and used the scale in the same way (Hair et al., Reference Hair, Black, Babin, Anderson and Tatham2005). The hypothesized multigroup model is the same shown in Figures 1 and 2, representing the one to be tested for its invariance across both samples from general population (invariance tests conducted across groups simultaneously).The goodness-of-fit statistics found for this configural model were: χ2(154) = 683.536; p < .001; CFI = .92; TLI = .91; RMSEA = .06 and CI for RMSEA = .05 to .06. These results are indicative that the hypothesized multigroup model of MAAS structure adjusts across the two samples in study.
Study 3: Convergent and Divergent Correlations of the Portuguese version of the MAAS
Method
Participants
The sample of participants is the same used in Study 1.
Measures
Mindful Attention and Awareness Scale (MAAS: Brown & Ryan, Reference Brown and Ryan2003) is described in Study 1 and the mindfulness score was computed with the 14-item factor structure found in the previous studies.
Five Facet Mindfulness Questionnaire (FFMQ: Baer, Smith, Hopkins, Krietemeyer, & Toney, Reference Baer, Hopkins, Krietmeyer, Smith and Toney2006; Portuguese version: Gregório & Pinto-Gouveia, Reference Gregório and Pinto-Gouveia2011). This instrument is based on a factor analytic study of five independently developed mindfulness questionnaires, which yielded five factors that appear to represent elements of mindfulness as it is currently conceptualized: observing, describing, acting with awareness, non-judging of inner experience, and non-reactivity to inner experience. All 39 items are answered in a Likert scale from 1 (never or rarely true) to 5 (very often or always true). Alpha coefficients for each of the facets showed them as internally consistent in the original study, as well as in this version in study (respectively: α Observe = .83/.80; α Describe = .91/.87; α Actaware = .87/.89; α Nonjudge = .87/.82; α Nonreact = .75/.63).
Positive and Negative Affect Schedule (PANAS: Watson, Clark, & Tellegen, Reference Watson, Clark and Tellegen1988; Portuguese version: Galinha & Pais-Ribeiro, Reference Galinha and Pais-Ribeiro2005). This instrument measures positive and negative constructs as both states and traits. Ten descriptors are used for each positive affect and negative affect scales to define their meanings. Participants are required to respond to a 20-item test using a 5-point scale that ranges from very slightly (1) to extremely (5). Cronbach’s alphas in the original and in this study were, .89 and .86, respectively for the positive affect subscale; and .85 and .90, respectively for the negative subscale.
Depression, Anxiety and Stress Scales – short version (DASS 21: Lovibond & Lovibond, Reference Lovibond and Lovibond1995; Portuguese version: Pais-Ribeiro, Honrado, & Leal, Reference Pais-Ribeiro, Honrado and Leal2004). The DASS is a quantitative measure of distress along the axes of depression, anxiety (symptoms of psychological arousal) and stress (the more cognitive, subjective symptoms of anxiety). It is a short form of the 42-item self-report measure of depression, anxiety, and stress (DASS), which comprises three 7-item self-report scales with adequate internal consistency (α Depression = .88, α Anxiety = .82 e α Stress = .90) either in the original version, or in the version used in this study (α Depression = .90, α Anxiety = .88 e α Stress = .88). Items are rated on a Likert scale from 0 (did not apply to me at all) to 3 (applied to me very much, or most of the time).
White Bear Suppression Inventory (WBSI: Wegner & Zanakos, Reference Wegner and Zanakos1994; Portuguese version: Pinto Gouveia & Albuquerque, Reference Pinto-Gouveia and Albuquerque2007). The WBSI is a 15-item questionnaire measuring people’s general tendency to suppress thoughts, on a 5-point scale from 1 (strongly disagree) to 5 (strongly agree), with a total score ranging from 15 to 75. Internal consistency of the WBSI in the original study was high across several student samples, with Cronbach’s alpha ranging from .87 to .89. In this study this coefficient was of .90.
Rumination-Reflection Questionnaire (RRQ-10: Treynor, Gonzales, & Nolen-Hoeksema, Reference Treynor, Gonzalez and Nolen-Hoeksema2003; Portuguese version: Pinto-Gouveia & Dinis, Reference Pinto-Gouveia and Dinis2006). Its 10 items are completed in a scale from 1 (almost never) to 4 (almost always) and the scale can be scored for two factors: brooding and reflective pondering. The original reliability analysis revealed coefficients of .72 for the subscale Reflection and of .77 for Brooding subscale (Treynor et al., Reference Treynor, Gonzalez and Nolen-Hoeksema2003), coefficients identical to this study analysis results (respectively, .72 and .78).
Brief Symptom Inventory (BSI: Derogatis, Reference Derogatis1975; Portuguese version: Canavarro, Reference Canavarro, Simões, Gonçalves and Almeida1999). This instrument consists of 53 items covering nine dimensions –Somatization, Obsession-Compulsion, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic anxiety, Paranoid ideation and Psychoticism– and three global indices of distress –Global Severity Index, Positive Symptom Distress Index, and Positive Symptom Total– which measure current or past level of symptomatology, intensity of symptoms, and number of reported symptoms, respectively. It allows the identification of self-reported clinically relevant psychological symptoms. The BSI showed its internal consistency (original study α: .71 to .85; the scale validation study α: .62 to .80).
Procedure
With the purpose of testing the convergent and discriminant validity, and ultimately construct validity, we correlated the Portuguese version of MAAS (the 14 items-version found) with other measures theoretically predicted to correlate with mindfulness and with measures of theoretically different concepts.
Results
Table 3 presents the correlations between the 14-item Portuguese version of MAAS and other variables measured through several scales.
Table 3. Pearson-product moment correlations between the MAAS and the mindfulness facets Observe, Describe, Act with Awareness, Nonjudge and Nonreact – FFMQ (N = 530), Positive and Negative Affect – PANAS (n = 347), Depression, Anxiety and Stress – DASS-21 (N = 530), Thought Suppression – WBSI (n = 350), Rumination – RRQ-10 (n = 350), Somatization, Obsessive-Compulsive, Interpersonal sensitivity, Depression, Anxiety, Hostility, Paranoid ideation e Psychoticism – BSI (n = 224)

Note:
*p < .050; **p < .010
On one side, we found some expected positive correlations between mindfulness as measured through MAAS and through FFMQ, specifically: Describe, Act with awareness and Nonjudge. Among these, the strongest positive correlation observed was between MAAS and Act with Awareness facet, most likely due to the fact that the content of this mindfulness facet overlaps considerably with the content of MAAS items. The construction of FFMQ results of an exploratory factor analysis of several mindfulness questionnaires and the majority of the items of this specific mindfulness facet come from MAAS. Baer et al. (Reference Baer, Hopkins, Krietmeyer, Smith and Toney2006) affirm that this facet and MAAS have been shown to measure the same construct.
Also we found a small positive correlation between positive affect (PANAS) and present-centered attention and awareness measured with MAAS.
On the other side, just as the original authors, our findings show that low mindfulness is associated to poor psychological health. Specifically, persons who demonstrate lower levels of present-centered awareness and attention, more often present higher levels of negative affect, depressive, anxious and stress symptomatology. These negative associations between mindfulness with both anxiety and depression were consistent across both measures (DASS and BSI).
Also, a smaller tendency for mindful attention and awareness was consistently associated with higher levels of psychopathological symptoms. Namely, lower mindfulness trait was moderately associated with more somatization, obsessive-compulsive symptoms, interpersonal sensitivity, hostility, phobic anxiety, paranoid ideation and psychoticism.
Rumination is defined by the authors of RRQ-10 as a method of coping with negative mood involving attention and reflection focused either on the self and one’s negative emotions. In this study we replicated the findings by the authors of MAAS that brooding, a clearly non-adaptive form of rumination, is reported less by persons who are more mindful toward their daily life experiences.
Finally, we also observed the same negative association for thought suppression, indicating that the chronic tendency to suppress thoughts, as a mental control strategy, is negatively related to the ability of staying with the present moment experience, independently on its classification as positive or negative. Altogether these results point to the fact that individuals with higher mindfulness use less emotion regulation strategies known to be negative and ineffective.
Discussion
In recent years mindfulness has been increasingly investigated and the lack of instruments with robust validations to measure it has been one of the major limitations pointed in the studies of its efficacy in respect to its application within several psychological treatment programs. To overcome this methodological problem some authors have developed distinct self-report measures of mindfulness. This research study was to validate the MAAS for the Portuguese population.
Two confirmatory factor analyses of the Portuguese version of MAAS yielded a single-factor solution attesting for the goodness of fit of a model with 14 items of this scale. Therefore, several standardized indicators have the required theoretical and statistical support for us to conclude about the plausibility of our version of this mindfulness trait measure. Also, cross-validation statistics confirmed the measurement invariance of this instrument through two different samples from the general population.
In line with previous findings, mindfulness as measured by MAAS showed positive correlations with mindfulness facets and positive affect. Also as expected, individuals with lower levels of mindful attention and awareness presented higher levels of emotional disturbance and psychopathological symptoms. Moreover, individuals higher in this dispositional trait of mindfulness reported less dysfunctional emotion regulation strategies. Results of this investigation are similar to the results found with the original version of the questionnaire.
Altogether, our findings largely support the psychometric validity of the MAAS as a reliable instrument for the measure of the general tendency to be mindful in daily life for the Portuguese population. We have enough evidence to believe that the best solution is the 14-item version, but we recommend more research on the Portuguese version with all its 15 items until more evidence of this finding. Also, it should be a task for further investigation the possibility of validating the Portuguese version of the MAAS in specific clinical populations.
To conclude, we hope that this paper will lead to a more widespread use of the Escala de Atenção e Consciência Plena in the assessment of mindfulness as a psychological construct for the Portuguese population.





