


Hydatid disease is a parasitic infection that is endemic in certain parts of the world. Hydatid cysts commonly affect the liver and lungs, although any part of the body can get affected. Cardiac involvement is rare, with an incidence of 0.5% to 2%.Reference Heyat, Mokhtari, Hajaliloo and Shakibi 1
Case presentation
A 17-year-old male was referred to our emergency department with a history of acute retrosternal discomfort of/for 2-hour duration. He had no history of dyspnoea, fever, palpitation, or syncope. Past history was not suggestive of any cardiac or respiratory illness. On physical examination, his blood pressure was 140/70 millimetres of mercury and heart rate was 102 per minute. Cardiovascular examination was unremarkable. Abdominal examination was within normal limits. Electrocardiography showed sinus tachycardia with T inversion in leads I, aVL, and V5–V6. Chest X-ray showed a normal cardiothoracic ratio with a bulge in the left heart border. Routine blood investigations were within the normal range. ESR was 35 millimetres at 1 hour. CRP was 2.2 milligrams per decilitre. Serial cardiac biomarkers were within normal limits.
Two-dimensional transthoracic echocardiography demonstrated a cystic mass measuring 20 × 22 millimetres within the posterolateral wall of the left ventricle (Fig 1; Supplementary Video: 1–3). Within the cyst, multiple daughter cysts were visible. No other abnormality was detected on echocardiography. Magnetic resonance in T2-weighted imaging of the heart showed multiple cystic spaces embedded within a large solitary cyst situated in the posterolateral wall of the left ventricle (Fig 2a and b). There was no pericardial effusion or other lesions in the lungs. Blood serology – indirect haemagglutination, indirect fluorescent antibody tests – were positive for hydatidosis. However, enzyme-linked immunosorbent assay was negative.
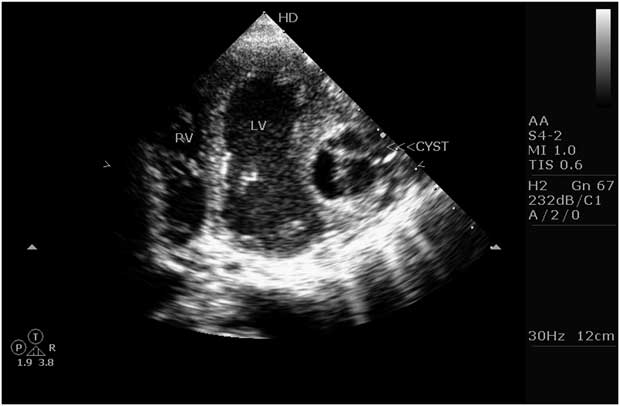
Figure 1 Transthoracic echocardiography in an apical four-chamber view showing a large cystic mass with multiple daughter cysts within the lateral wall of the left ventricle (arrow). LV = left ventricle; RV = right ventricle.

Figure 2 ( a and b ) Magnetic resonance imaging showing a large cystic mass with multiple daughter cysts within the posterolateral wall of the left ventricle.
Surgical excision of the mass was offered to the patient but he refused. He was started on high-dose oral albendazole (2400 milligrams per day in three divided doses). There was a dramatic improvement in chest pain at 3 months of follow-up with a partial regression of the cyst on echocardiography.
Discussion
Human hydatidosis is typically due to infection with the canine tapeworm Echinococcus granulosus. Cardiac hydatidosis is uncommon, with the left ventricle being the most common site, accounting for 77% of all cases of cardiac hydatidosis, whereas the left atrium is the least affected site, with an incidence of 3.7%.Reference Heyat, Mokhtari, Hajaliloo and Shakibi 1 The clinical picture of cardiac echinococcosis is dependent on the location of the cyst and its degree of interference with the function of the surrounding structures. It can act as a space-occupying lesion causing low cardiac output, ventricular outflow obstruction, or constrictive pericarditis. Cardiac hydatidosis may present with non-specific features such as weight loss, dyspnoea, and fever.Reference Di Bello 2 The presentation can be more dramatic if the cyst ruptures, resulting in anaphylactic shock, and/or rarely cardiac hydatidosis may present as acute coronary syndrome as seen in our patient. Our patient had non-specific ST–T changes in the representative electrocardiographic leads of the posterolateral surface of the heart. Hence, cardiac hydatid disease should be considered among differentials of chest pain in young individuals.
Patients who have a history of echinococcosis and who are admitted with these symptoms and signs must be evaluated for cardiac involvement. Owing to the fact that the condition can mimic a number of cardiac diseases, the differential diagnosis includes all other cardiac tumours and cysts, mediastinal tumour, pericardial cyst, ventricular aneurysm, etc. The growth of hydatid cysts is usually slow and asymptomatic. However, if not detected, the cyst may become life threatening. Without prompt surgical treatment, rupture of the cyst or compression of vital structures may occur. Initially, the cyst grows slowly between the cardiac fibres and causes no signs or symptoms. Later, it may cause precordial pain, dyspnoea, and palpitations when it becomes large enough to compress, displace, or invade the surrounding structures. The most important major complication is the rupture of the cyst, which can trigger anaphylactic shock or tamponade. Other major complications are systemic or pulmonary embolisation, compression of coronary branches with subsequent angina, conduction defect, or complete atrioventricular block owing to compression of the bundle of His, intermittent valvular block causing syncope, and arrhythmia.Reference Ameli, Mobarhan and Nouraii 3 – Reference Lund, Ehman, Julsrud, Sinak and Tajik 6
The diagnosis of uncomplicated hydatid cyst of the heart is difficult because clinical and radiographic findings are lacking or non-specific. Two-dimensional echocardiograms can show the cystic nature of the mass and its relationship to the cardiac chambers.Reference Shakibi, Safavian, Azar and Siassi 7 Magnetic resonance images show the anatomic extent and position of the mass and its relationship to the cardiac chambers. The mass in our case had the characteristic signal intensity of a cystic lesion and typical low-signal-intensity rim from the cystic wall.
Surgical treatment is the only option for cardiac hydatid disease, as medical therapy does not offer insurance against rupture of the cyst and its potential complications.Reference Di Bello 2 , Reference Ameli, Mobarhan and Nouraii 3 Resection of an intracardiac cyst is recommended to avoid the grave complication of rupture, which is as common as 39%. During excision, it is important to avoid spilling the cyst content, which may trigger an anaphylactic reaction. Reported results of surgical resection have been very encouraging with low mortality.Reference Shakibi, Safavian, Azar and Siassi 7 Owing to the fact that our patient refused surgery, he was given a trial of high-dose oral albendazole, which gave gradual symptomatic relief with partial resolution of the cyst.
Conclusion
Hydatid cyst of the heart is a rare disease and has varied manifestations ranging from asymptomatic to cardiac tamponade and sudden death. It should be considered in the differential diagnosis of acute chest pain especially in young adults without conventional risk factors of atherosclerosis.
Supplementary materials
For supplementary material referred to in this article, please visit http://dx.doi.org/doi:10.1017/S1047951112001230



