


Introduction
Public health and emergency management agencies play a critical role in addressing the needs of vulnerable populations in preparation for and response to emergencies. Identifying and leveraging community assets are a way to address such needs. Community assets consist of existing resources that vulnerable populations rely upon and engage with at the local level. Public health agencies have used community health assets (a subset of such assets that relate to the health of the community) identification to promote community health in a variety of circumstances. Reference Morgan1,Reference Morgan and Ziglio2 Community health assets include physical, financial, social, and environmental or human resources. Reference Harrison, Ziglio, Levin and Morgan3 These assets can operate as protective and promoting factors to buffer against life’s stresses. Reference Morgan and Ziglio2 We believe that local knowledge, the comprehensive system of concepts, beliefs, and perceptions generated by community members in a given setting, is 1 type of community asset that can be leveraged in preparedness efforts. While practitioners commonly recognize the value of local knowledge in emergency preparedness, Reference Roth4 there has been limited research on how to define such knowledge and how to collect local knowledge-related data. To address this gap, we interviewed community leaders to explore this construct and subsequently pilot tested a mobile technology-based tool to facilitate the collection and mapping of local knowledge of community health assets. As such, the objective of this study was twofold: (1) Explore and define what type of local knowledge community leaders can contribute to in preparedness planning, and (2) develop and pilot test a mobile technology tool to facilitate the integration of community leaders’ local knowledge into preparedness planning.
In this study, we first describe the 2 conceptual pillars of our study rationale: community-based planning (CBP) for vulnerable populations and the health asset-based model. Next, we elaborate on the concept of local knowledge and continue by describing study methods and results.
Background
Community-Based Planning (CBP) for Vulnerable Populations
The Centers for Disease Control and Prevention (CDC) highlights a variety of factors that may influence a person’s vulnerability to an emergency, including socioeconomic status, age, gender, race and ethnicity, English language proficiency, immigration status, medical conditions, and access and functional needs. 5 CBP is 1 strategy employed by disaster management professionals to build local-level capacity and address some of these vulnerabilities. Reference Kheir6 The strategy includes leveraging the knowledge, capabilities, and resources of local communities. Successful implementation of CBP requires an understanding of the communities involved and how these communities function. 7,Reference Allen8 CBP can be particularly helpful when working with marginalized or insular communities that may lack trust in the government due to their immigration status or prior negative experiences. Reference Cordero-Guzmán9-Reference Beard and Sarmiento11 To date, CBP efforts have mainly focused on identifying community needs and vulnerabilities using a deficit-based model where problems in a community are identified solutions and developed relying on resources outside of the community. In our study, we examined the use of a health asset-based model.
The Health Asset-Based Model
The health asset-based model was originally developed for the public health workforce to re-orient their thinking on community planning and intervention development. This model is built upon the concept of salutogenesis, a term drawn from medical sociology. Salutogenesis emphasizes factors that support human health and well-being, rather than those causing disease (pathogenesis). Reference Lindström and Salutogenesis12 The World Health Organization (WHO) defines health assets as the resources that individuals and communities have at their disposal that protect against negative health outcomes and/or promote health status. Reference Van Bortel, Wickramasinghe, Morgan and Martin13 Health assets can operate at the individual, community, or institutional level. In contrast to a deficit-based model, the health asset-based model entails assessing what communities have to offer in building and developing local capacities for reaching their health goals. Reference Morgan and Ziglio2 Community planning and asset mapping are part of the application of a health asset-based model, which focuses on both tangible and intangible community assets. Reference Kramer, Amos, Lazarus and Seedat14 Use of a health assets model can eventually lead to the creation of inventories (or asset maps) of the resources and skills available at the community level before intervention development. Reference Kerka15 This model has been applied by public health agencies in a variety of contexts, such as engaging faith-based leaders to outreach the population, supporting anti-poverty campaigns, and leveraging citizens and institutions in rural communities to reduce barriers to access health care services. Reference Kerka15-Reference Beaulieu17
Local Knowledge in Emergency Preparedness
Local knowledge, 1 type of health asset, is a valuable and untapped resource that can facilitate community problem-solving. Local knowledge develops informally over time by individuals and communities, based on experience, and local culture. Local knowledge is iterative, cyclical, dynamic, and evolves with the community and its leaders. This may also include the way people observe and measure the environment around them, solve problems, validate new information, and establish the processes whereby knowledge is generated, stored, applied, and transmitted to others. Reference Srinivas18,Reference Cutter, Boruff and Shirley19 Many social problems have local origin, thus, local knowledge plays a key role in problem identification, definition, legitimization, and, most importantly, in finding solutions. The chances of successful policy implementation are low without the understanding and consensus of local actors. Reference Srinivas18 Resident involvement in both defining problems and finding solutions is needed to build the legitimacy required to implement policy in an effective manner. Reference Srinivas18 In this study, we seek to explore and define the concept of local knowledge in emergency preparedness and share our experience in creating and exploring the use of a mobile-based tool to facilitate the gathering of local knowledge by community leaders and sharing of such knowledge with preparedness planners. The aim of this study is to describe the process of developing this type of tool rather than the impact of the tool per se. As we could not address all types of vulnerabilities, based on the group of community-based organizations (CBOs) we had relationships with, we focused on immigrant and ethnic communities and sought to identify the ways in which local knowledge could be shared and contributed to emergency preparedness planning. Reference Lin, Savoia, Agboola and Viswanath20
Methods
We implemented this study in 3 phases: conceptualization, tool development, and field testing. We conducted an initial conceptualization phase by interviewing community leaders who helped us explore the concept of local knowledge in emergency preparedness and types of community assets they could point to as useful for preparedness planning efforts, followed by a tool development phase where we created a directory of community assets in the form of a mobile application. We then conducted a field-testing phase where the tool (a mobile application functioning as a directory) was pilot tested. See Figure 1 for a visual representation of the different phases. The details of the methods used in each phase are described in the following texts.

Figure 1. Study implementation phases (conceptualization, tool development, and field testing).
Conceptualization Phase: Interviews With Community Leaders
CBOs located in the states of Florida, Massachusetts, West Virginia, and the territory of Puerto Rico, partners in this project, identified an initial pool of community leaders to be interviewed. Such leaders were recruited at the local level, in the city or town where the CBO was based. The interviewees did not receive incentives to participate in the interviews. We then applied a snowball technique to recruit additional subjects and conducted the interviews up to the saturation of response content. We defined saturation as the point at which additional information was not adding new knowledge but confirming the information we had already received. Based on the type of CBOs we engaged, we recruited community leaders with experience serving communities with vulnerabilities due to poverty, limited English proficiency, ethnocultural and geographic isolation, and drug addiction. These leaders were selected because of their familiarity with emergency preparedness issues due to either personal experience as a disaster survivor or engagement as a preparedness volunteer (ie, Medical Reserve Corps volunteers) or as a government official engaged in local response efforts. These leaders could be categorized according to their position and type of interaction with the community in 3 non-mutually exclusive groups: (1) employees of governmental and health care organizations; (2) members of CBOs (ie, faith-based organizations, volunteer groups, etc.); and (3) citizens with substantial civic engagement at the community level. Interviews were conducted in person, followed an interview guide, and lasted between 45 and 90 minutes. The Harvard T.H. Chan School of Public Health Institutional Review Board deemed the study protocol as exempt.
Interviewing Technique
The interviews were conducted using the convergent interviewing technique. Reference Williams and Lewis21 This technique seeks to resolve the dilemma of broad versus specific questions. Using this technique, data, derived from an initial set of interviews, are analyzed to inform the development of more specific probe questions in subsequent interviews. Thus, the interview process becomes more and more structured with each subsequent interview. By applying this method, we were able to gather information about specific challenges experienced during emergencies, as well as examples of existing community assets to address such challenges. We started each interview by asking the interviewee to talk about the characteristics of her/his community followed by exploring how community members communicate, where they feel safe, and whom they trust during everyday life as well as in emergencies. Interviews were conducted from August to October 2017 in 4 languages – Somali, Spanish, Portuguese Creole, and English. The interview guide was first translated from English into the language spoken by the interviewee and then back-translated into English for validity purposes. Interviewers had experience in public health practice and were members of the community where the interviews were conducted. We trained interviewers on the use of the interview guide. All interviews were recorded, transcribed, and translated into English.
Interviews’ Data Analysis
We adopted systematic coding procedures to analyze the interviews’ data using a hybrid method of deductive (pre-set scheme) and inductive (derived from the data) coding. The interview guide included questions on means of communication, trust in organizations engaged in preparedness efforts, personal preparedness, and experience with evacuation and shelter operations. We also assigned codes to reflect both finer distinctions within thematic areas and relationships between topics. Two analysts coded each interview using QSR International’s NVivo v.11 software and achieved full agreement on the coding scheme through discussion. A third analyst analyzed the interviews’ transcripts in the language of origin to resolve any disagreements between coders and to review the final coding.
Tool Development and Field-Testing Phase
We reviewed the results of the interviews and focused on the examples of community assets named by the interviewees, and grouped them into categories. While the assets cited during the interviews were specific to the selected communities and geographic areas, our goal was to identify and name the categories they belong to in order to develop a directory that could be meaningful to any community (Table 1). When the categories and overall structure of the directory were created, we hosted feedback meetings in the same 5 communities where the interviews were conducted. Seventy-one community leaders, with experience in civic engagement, participated in these meetings and provided feedback on the structure of the directory, as well as suggestions on how to turn the directory into a user-friendly tool. Based on such feedback, we converted the directory into a mobile application with the use of the Appy Pie software. 22
Table 1. Directory categories of community assets

We then engaged 9 community leaders to pilot test the app and enter information about community assets that could be useful to emergency planners. We instructed the 9 testers via a webinar on the use of the mobile application, asked them to download it on their phone (Androids and iOS), and then asked them to use it for a month to enter information about assets in their community across the pre-identified categories and view the information entered by each other. Figure 2 describes the flow of information from the community leaders to emergency planners. Finally, we presented the app and data entered by the community leaders during the pilot test, to a group of preparedness planners in Massachusetts and in Puerto Rico in November 2019 and January 2020. The app presentation was embedded into a discussion-based exercise, and practitioners were asked to provide feedback on the usefulness of the application for emergency preparedness planning and recovery efforts. We presented practitioners with an emergency scenario, consisting of a hurricane in Massachusetts and an earthquake in Puerto Rico, and asked them to use the directory of community assets to identify resources that could enhance their public communication capabilities in recovery from these emergencies. We envisioned the tool to be more of a planning and recovery instrument rather than a response tool, and as such was presented.
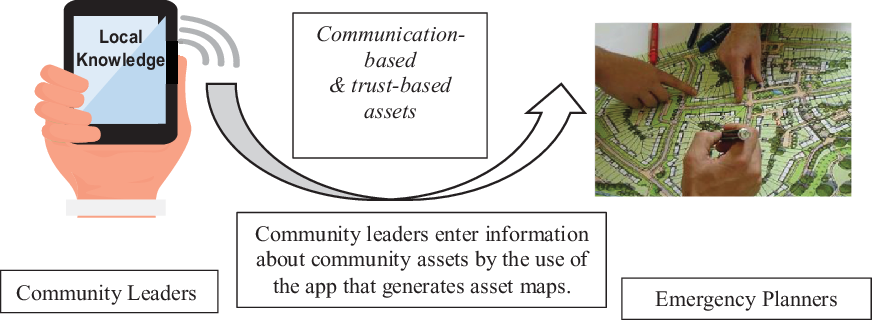
Figure 2. Flow of information between community leaders and emergency planners.
Results
Interviews’ Results
We interviewed 106 community leaders belonging to 5 communities located in 3 states and 1 territory: 21 in Florida, 21 in Puerto Rico, 40 in Massachusetts, and 24 in West Virginia. Five were employees of governmental and health care organizations, 41 were members of CBOs (ie, faith-based organizations, volunteer groups, etc.), and 60 were citizens with substantial experience in civic engagement at the community level. The coding process led to the creation of 13 major codes, corresponding to categories of community assets that were consolidated into 2 main themes of local knowledge: communication-based and trust-based local knowledge. Presented in the following are the results of the interviews, providing some examples of what types of assets were identified by the community leaders. The examples are heavily focused on ethnic minorities (immigrants, in particular) and their specific needs/requirements for information transmission; this is due to our sample and is clearly reflective of the sub-communities we focused on. We still believe there is a value in presenting these results so that practitioners reading this paper concretely understand and see examples of local knowledge. We believe the process we adopted for data collection, and the categories identified and presented in Table 1 apply to any community.
Local Knowledge of Communication-Based Assets
We defined local knowledge of communication-based assets as knowledge of assets that relate to preferred means of communication by members of the community. Community leaders talked about how the communities they belong to, which are mostly ethnic communities, prefer to receive information through face-to-face interaction rather than by phone or other means. They reported that knowing about specific places where community members get together (ie, local churches, restaurants, and/or coffee shops) and times of the year during which they are more likely to convene (ie, religious or country of origin festivities) can be useful for hosting preparedness education venues or disseminating information using fliers. Interviewees also highlighted the importance of being aware of age, income, and gender differences in the use of specific means of communication. They reported that younger members of their community were more inclined to the use of social media, low-income individuals preferred to receive alerts by text message rather than by phone call, and, in some ethnic communities (ie, Somalia), women were more likely to receive information from family and friends rather than by attending public events. The interviewees named specific community assets related to the outreach and communication efforts: local translators, mass and social media channels (ie, ethnic TV and radio stations and community-oriented Facebook pages), places where community groups regularly get together or visit (ie, worship places, building management offices, barbershops, and beauty salons), names of organizations that have created text alerts or automated phone call trees, and names of organizations with experience in conducting door-to-door informational campaigns. Community leaders also talked about the need of raising awareness at the community level on the importance of personal preparedness. They reported that the availability of 72-hour food supplies was unlikely for many community members, mainly due to their low purchasing power, which could be supplemented in preparation for an emergency. They also suggested that the best time to get the attention of immigrants on emergency preparedness is when they arrive for the first time in the country and get oriented about life in the United States.
Local Knowledge of Trust-Based Assets
We defined local knowledge of trust-based assets as knowledge of assets that relate to organizations, processes, and spaces that are trusted by the community. Community leaders talked about the need for the community to be educated about emergency preparedness and that an effective way to do so is by having representatives with subject matter expertise from government agencies or local academic institutions host community meetings in close collaboration with organizations and volunteer groups trusted by the community. Community leaders pointed to the following criteria as indicative of trusted figures: people/organizations with pre-existing relationships with community groups (defined by ethnicity or specific vulnerability, ie, substance abuse), cultural competency, and ability to maintain confidentiality regarding immigration status or illicit behaviors (ie, use of illegal drugs). Community leaders were also asked to describe how citizens experience spaces in the community based on a variety of circumstances. For example, where people do and do not feel physically or emotionally safe (ie, shelters located in areas affected by previous disasters, places associated with previous experience or symbols of discrimination), the type of transportation they have access to, and what basic characteristics “spaces” should have to address their needs. Community leaders talked about how lack of transportation, concerns with safety, privacy regarding medical conditions, and respect for personal and cultural traditions may affect compliance with evacuation orders and sheltering operations. Interviewees also reported several challenges community members could experience if asked to evacuate their homes and go to an emergency shelter, such as having limited access to transportation to reach the shelter site, feeling worried to leave their property because of burglary, feeling uncomfortable to stay in a location where there are people they do not know, feeling incapable to leave their home if the shelter site does not allow for pets, and that they would refuse to go to the shelter if they were unable to bring what they need to be able to practice their cultural and religious traditions (ie, a rug to pray). Interviewees then identified community “spaces” that could potentially address some of these challenges. For example, they listed facilities that are not currently named as a formal or municipal disaster shelter but that could serve for that purpose because they are recognized by the community as safe and culturally appropriate places, and local organizations with the availability of vans that could be used to fulfill transportation needs.
Tool and Field-Testing Results
A total of 71 community leaders participated in the community meetings across the 5 study sites. Attendees included representatives from public health agencies, youth groups, elderly services, faith-based, health care and educational organizations, and volunteer groups. They provided general feedback on the categories included in the directory in terms of content and face validity and specific feedback on how the categories were named. Revisions to the tool were made accordingly. Participants solicited and discussed the idea of turning the directory into a mobile application. As a result of these discussions, we created a prototype for the app version of the directory. A demo of the prototype of the app implemented during the project can be found using the weblink, https://www.youtube.com/watch?v=OovghRosc4s. 23 A field-testing phase of the app was implemented by engaging 9 community leaders. Reference Agarwal, LeFevre and Lee24 The 9 leaders were surveyed using a qualitative form to rate the usability of the tool, its features, and likelihood of use, after the pilot phase to report on their experience in using the app. They reported that viewing information about the community assets in the app was either easy or very easy, that they did not experience any technical difficulties but that adding information using the crowdsourcing tool was challenging for half of them. Subsequently, we gathered feedback on the usefulness of the directory from 20 practitioners (including public health officials, preparedness coordinators, and emergency managers) attending the tabletop exercise in Massachusetts and 10 in Puerto Rico, 83% of whom had disaster planning responsibilities within their job duties. Overall, 63% of respondents were working in a public health or governmental agency, 17% in a health care organization, and the rest for CBOs. All respondents found the data on community assets entered in the directory as valuable information for emergency planning, in particular, about communication planning for vulnerable populations. Respondents reported that they could use the directory for emergencies, such as pandemic influenza, foodborne illness, severe weather, or any type of emergency planning affecting infrastructures (ie, water contamination, power outage). In Massachusetts, only 3 out of 20 respondents did not see themselves using the directory in any emergency scenario; in Puerto Rico, none. When asked to provide feedback on the usefulness of the directory and its mobile version in an open response question, respondents reported that they believed the app technology could be a friendly instrument “to raise awareness about the need to outreach vulnerable populations, especially among agencies not used to plan for the needs of vulnerable segments of the population.” They also thought the app could be particularly useful for small communities to help them have better access to resources in nearby towns so that community assets could be stored in the same directory and be accessible to all users with the use of a common platform. Some liked the fact that the app could function as a portable data set of information – “much better than flipping through the pages of a plan.” The data could be downloaded and be accessible offline. Most interestingly, practitioners mentioned that this tool could help develop new lines of communication and prompt emergency planners to “take a different look at their community, do things differently and plan in advance to reach vulnerable groups.” Regarding constructive considerations, participants also pointed out the need for a gatekeeper for the information entered in the directory to “ensure the information is up to date and accurate” and that it would be important to be able to download the directory data in anticipation of situations of a power outage.
Discussion
Existing literature shows that people affected by disasters may play a crucial role in preparedness and mitigation efforts, but their knowledge is often ignored by the organizations in charge of the response or recovery efforts. Reference Dekens25 Prior studies have focused on developing tools to assess how inter-organizational coordination, including coordination with CBOs, helps in meeting needs that individual organizations cannot meet alone. Reference Glik, Eisenman and Donatello26 In our work, we sought to understand the types of local knowledge that could be integrated into preparedness efforts and whether an app could facilitate the sharing of knowledge between community leaders and preparedness planners. In this study, we explored and defined local knowledge in preparedness, and we provided results from the pilot testing of a mobile application designed to facilitate the integration of such knowledge into preparedness efforts. The mobile application represents a tool by which this information can be systematically shared by community leaders, who are those availing the knowledge and who have better access to vulnerable communities, with disaster planners, who are one of the users of such knowledge (agencies and community members themselves are both potential users who may find ultimate value in the information shared with this tool).
We recognize the limitations and challenges of our work. The types of knowledge that we identified are certainly not exhaustive of all types of local knowledge in emergency preparedness and reflective of the leaders we engaged, which were mainly from immigrant and ethnic communities. However, despite the fact that the 5 sites we engaged with had quite diverse community challenges, we were able to identify 2 common areas of local knowledge community leaders could contribute: communication and trust.
We then explored the possibility of using an app to systematically gather such knowledge. Yet, in and of itself, a mobile app for emergency preparedness is not novel. A review by Bachmann and colleagues identified 219 apps ranging in purpose and target users. Reference Bachmann, Jamison and Martin27 Most apps consist of alerting mechanisms, educational tools, and citizen-to-citizen apps designed for individuals in a given community who are looking to exchange resources during recovery efforts. However, despite the multitude of preparedness apps, there is currently no mobile application focused on information sharing by community leaders to emergency planners. The app development process we described is innovative, as it leads to the creation of a crowdsourcing tool to facilitate the sharing of information by community leaders with the public health practice and emergency management community with the scope of enhancing preparedness planning and recovery efforts.
We also recognize that there are technical limitations in using an app to capture local knowledge in preparedness planning. The strongest limitations are those related to security issues when entering the data into the application. It is important to identify who is entering, vetting, and using the data, which leads to 3 key processes in the development and implementation of this process: the identification of the community leaders who will be engaged in entering the data, the identification of the public health practitioners and emergency managers who will use the data, and the identification of a gatekeeper. Having a clear user vetting protocol for information entry and access could be a way to enhance security and ensure the functionality of the app. Our data also indicate that, while the app was easy to use to view the data, uploading information is still a task that requires technical skills that not all community leaders may have. Currently, the project team manages and vets the resources and information entered into the app by the community leaders, and future iterations will have to consider the right gatekeeper to sustain this process, which may differ according to the community using the application. Finally, the practitioners who provided feedback on the app and type of data that could be collected with this instrument showed enthusiasm and appreciation for the possibility of including information on local resources they may not be aware of into their planning efforts. In particular, they emphasized how technology can help them change how they think about their community and develop preparedness and recovery plans for vulnerable groups. Yet, integrating local knowledge into preparedness efforts requires a political will to do so. When community leaders are included in planning efforts and local knowledge is valued as much as traditional knowledge, practitioners need to be ready to implement flexible plans that allow for the integration of such knowledge into their decision-making processes.
Conclusion
Community leaders’ engagement in preparedness efforts is important to identify community assets that can be leveraged to address the needs of the most vulnerable segments of a community. The use of a directory of community assets embedded in a mobile application can facilitate the integration of community leaders’ knowledge of such assets in preparedness efforts and enhance information sharing between community leaders and preparedness planners.
Acknowledgments
We are thankful to many community leaders engaged in this study and community-based organizations (CBOs) supporting us with outreach to the community, in particular, the MRC Health Department, Santa Rosa County, FL; Somali Development Center in Boston, the Cape Verdean Association in Brockton, MA; and to Mr. Alberto Montrond for his work as diplomatic liaison between Academia and the CBOs.
Author contributions
RPL conducted data analysis, facilitated the exercises and community meetings, and developed the manuscript. DB conducted interviews, analyzed data, facilitated exercises and community meetings, and oversaw the development of the mobile application. BQ conducted data collection, facilitated community meetings in Puerto Rico, and provided comments to the manuscript. NH conducted interviews, facilitated community meetings, and analyzed the interview data. ES conceived the study and was in charge of the overall direction and planning of research activities.
Funding statement
This project was supported by Broad Agency Announcement award number 200-2016-92417 Public Health Emergency Preparedness and Response Applied Research (PHEPRAR), funded by the Centers for Disease Control and Prevention (CDC). The conclusions, findings, and opinions expressed by the authors do not necessarily reflect the official position of CDC or the authors’ affiliated institutions.
Conflict(s) of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this paper.



