



Coronary sinus ostial atresia associated with persistent left superior vena cava is an extremely rare anomaly in univentricular heart. A 4-month-old boy with L-transposition of the great arteries with left atrioventricular valve atresia and hypoplastic left-sided morphologic right ventricle status post pulmonary artery banding, underwent a pre-cavopulmonary anastomosis diagnostic catheterization. Left innominate vein injection showed a tiny veno-venous collateral from left innominate vein to accessory hemiazygos vein (Fig 1a and b, Supplemental video 1). The patient underwent successful right-sided cavopulmonary anastomosis. At 5 years of age, left innominate vein injection during his pre-Fontan catheterization showed a dilated left superior vena cava (previously seen tiny veno-venous collateral) connected to dilated coronary sinus. The pre-Fontan haemodynamics were mean superior vena cava/pulmonary artery pressure 9 mmHg, left atrium pressure 6 mmHg, right atrium pressure 5 mmHg, cardiac index 3.8 L/min/m2, Qp:Qs = 0.53:1, and pulmonary vascular resistance (indexed) 1.5 WU × m2. Selective left superior vena cava angiography newly revealed coronary sinus ostial atresia with retrograde decompression of coronary sinus flow into now significantly dilated accessory hemiazygos vein (Fig 2a and b, Supplemental video 2). The raised venous pressure in the left innominate vein after cavopulmonary anastomosis had redirected coronary sinus flow into relatively lower pressure accessory hemiazygos vein draining to inferior vena cava. Retrospective review of prior echocardiograms confirmed coronary sinus ostial atresia (Fig 3a and b, Supplemental video 3). The device/coil occlusion or surgical ligation of this decompressing accessory hemiazygos vein would have impeded coronary sinus drainage leading to raised coronary venous pressure with potentially fatal outcome from myocardial venous congestion, ischaemia, or thrombosis leading to myocardial dysfunction. Reference Yokota, Kyoku and Kitano1,Reference Fulton, Mas, Brizard and Karl2 The segment of left superior vena cava between left innominate vein and accessory hemiazygos vein was therefore selectively occluded using AMPLATZER Vascular Plug II allowing continuous alternative drainage of coronary sinus through accessory hemiazygos vein to inferior vena cava (Figs 4 and 5, Supplemental video 4). The patient tolerated the procedure well with no immediate complications with oxygen saturation in mid-80%. He continues on baby aspirin and will undergo unroofing/opening of coronary sinus to an atrium along with accessory hemiazygos vein ligation during his Fontan surgery to allow unobstructed coronary venous flow into the atria.

Figure 1. Selective angiogram of left innominate vein (LIV) in (A) frontal and (B) lateral planes prior to cavopulmonary anastomosis showed a tiny veno-venous collateral from LIV.
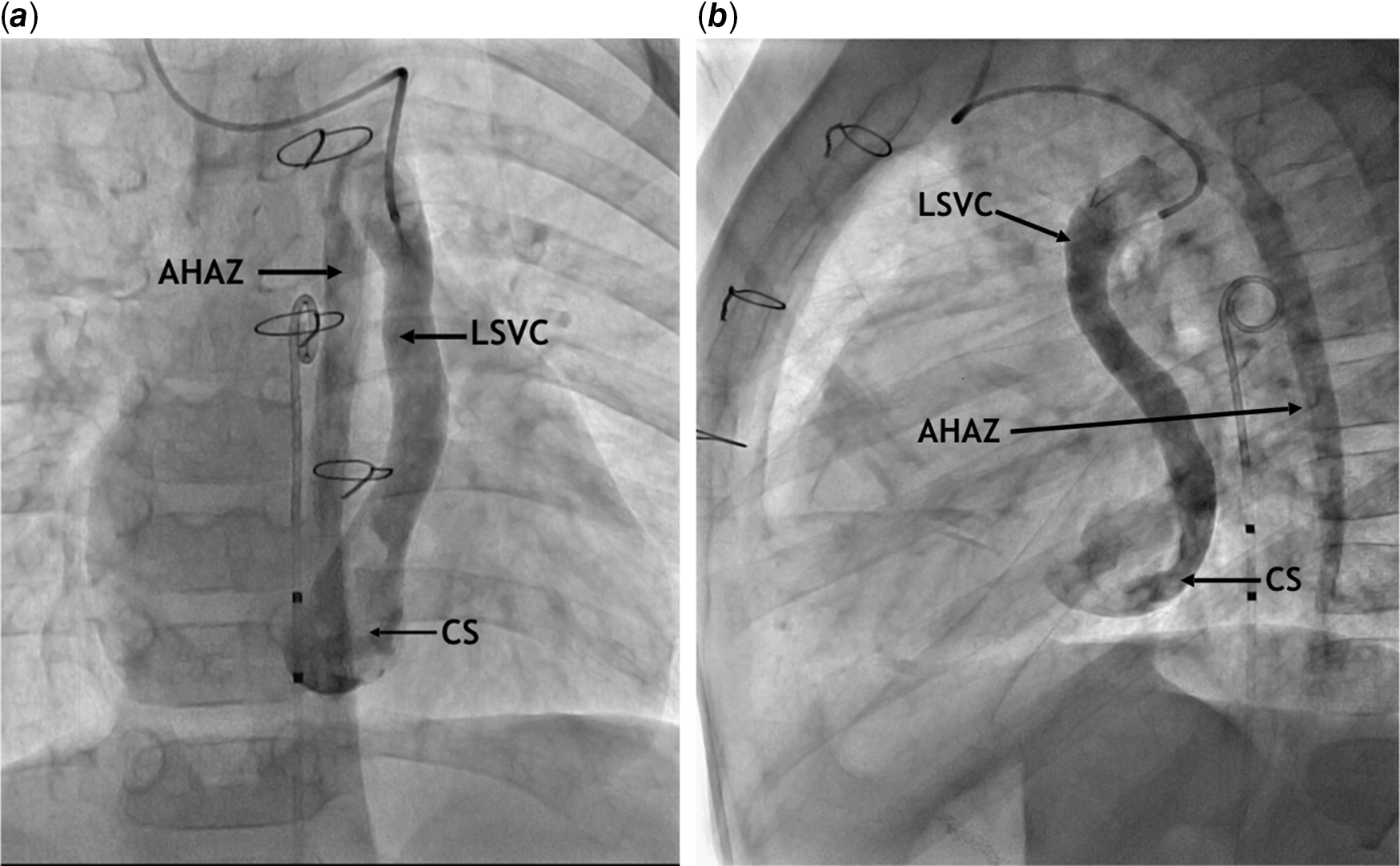
Figure 2. Selective angiogram of left superior vena cava (LSVC) in (A) frontal and (B) lateral planes prior to Fontan operation revealed coronary sinus (CS) ostial atresia with retrograde decompression of coronary sinus into dilated LSVC and accessory hemiazygos vein (AHAZ).

Figure 3. Transthoracic echocardiogram in subcostal (A) long-axis and (B) short-axis shows the atretic ostium of coronary sinus (CS) and its relation to interatrial septum (IAS), right atrium (RA) and left atrium (LA).
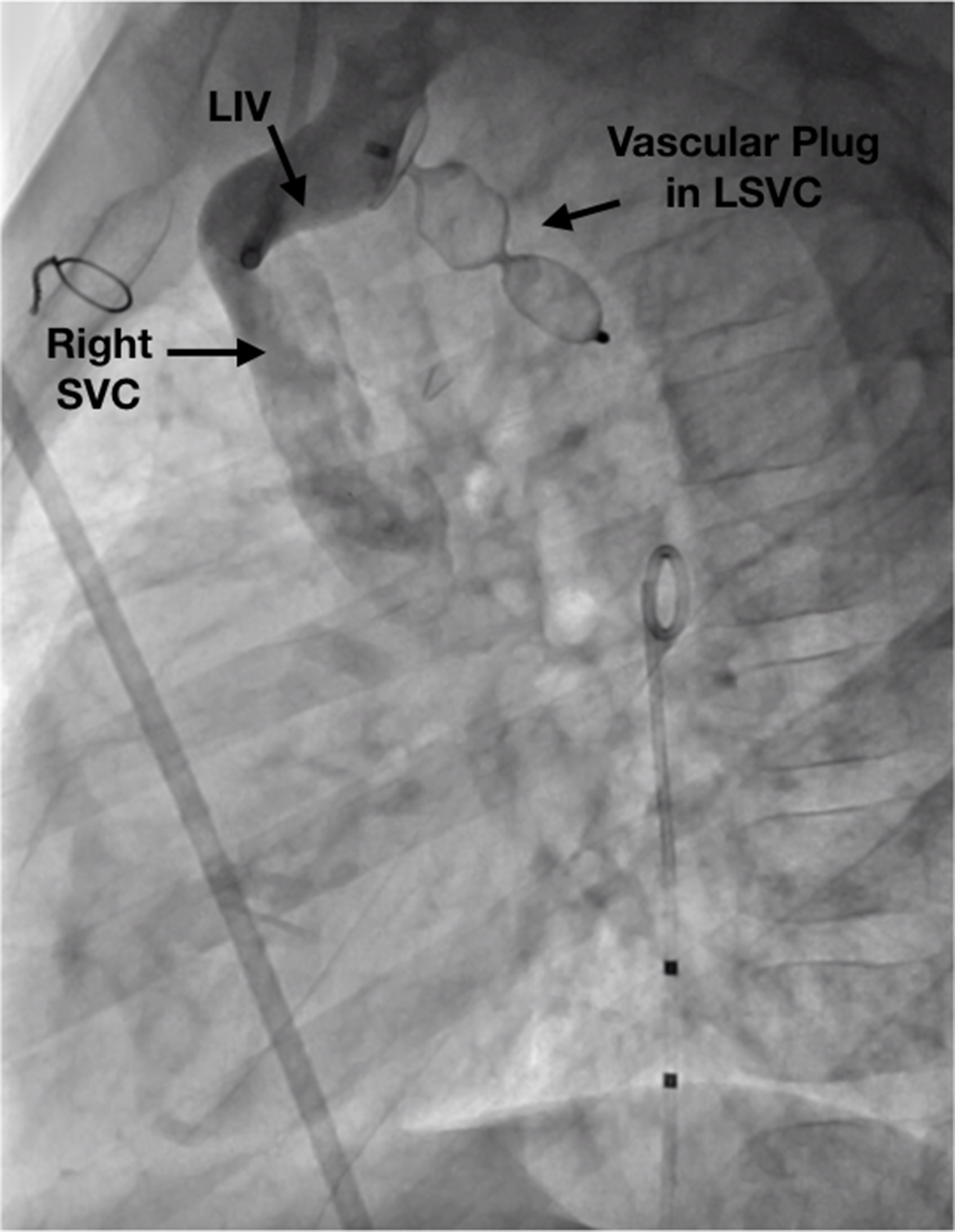
Figure 4. Fluoroscopic image of successful placement of AMPLATZER Vascular Plug II in the left superior vena cava (LSVC).

Figure 5. Diagram illustrating the blood flow before and after vascular plug placement in the left superior vena cava (LSVC) in the setting of coronary sinus ostial atresia (CSOA). AHAZ: accessory hemiazygos, IVC: inferior vena cava, LIV: left innominate vein, LPA: left pulmonary artery, RPA: right pulmonary artery, RSVC: right superior vena cava.
Coronary sinus ostial atresia can redirect the coronary venous flow into the inferior (our case) or superior vena cava (previous literature). Coronary sinus ostial atresia needs correction to allow drainage of coronary veins into a low-pressure atrium in univentricular hearts. Accidental blockage of this drainage during surgery or catheterization could have detrimental outcome due to myocardial hypoperfusion from coronary venous hypertension.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1047951121000767
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of interest
None.
Ethical standards
Not applicable.






