



Chest pain is a common complaint in childhood and adolescence and causes concern in both the patient and their family.Reference Blake1,Reference Yeh and Yeh2 The most common causes of chest pain in children are non-cardiac and include musculoskeletal and idiopathic origins, and cardiac diseases are found in the aetiology of chest pain in a small portion of the cases ranging from less than 1 to 10%.Reference Friedman and Alexander3–Reference Mohan, Nandi, Stephens, M’Farrej, Vogel and Bonafide6 Careful evaluation of medical history, and physical examination should be performed due to high mortality of cardiac-related chest pain in cases without rapid diagnosis and treatment.Reference Friedman and Alexander3,Reference Chun, Kim, Han, Kim and Yoon5,Reference Sert, Aypar, Odabas and Gokcen7 However, there is a controversy about determining which child could be affected by a serious organic disease and which tests could be performed for an exact diagnosis.Reference Saleeb, McLaughlin, Graham, Friedman and Fulton4 Aetiology of chest pain may show considerable variability based on the diagnostic approaches.
In young children, pain evaluation and ruling out cardiac diseases necessitate the use of resource-intensive procedures as their description and localisation of chest pain are generally not very accurate.Reference Gesuete, Fregolent, Contorno, Tamaro, Barbi and Cozzi8 In addition to the admission of children with chest pain to paediatric cardiology departments, prompt referral to a paediatric cardiologist is usually needed in patients who are evaluated at emergency departments or primary-care facilities.Reference Sert, Aypar, Odabas and Gokcen7,Reference Gesuete, Fregolent, Contorno, Tamaro, Barbi and Cozzi8 However, there have been few studies that investigated the outcome in patients with chest pain who were admitted or referred to a paediatric cardiology unit.Reference Sert, Aypar, Odabas and Gokcen7,Reference Evangelista, Parsons and Renneburg9
In this study, we aimed to investigate the distribution of diseases underlying chest pain in children and adolescents to understand the clinical characteristics of children with chest pain referred to a paediatric cardiology outpatient clinic.
Materials and methods
Study
A prospective cohort study of children with chest pain between the ages of 3 and 18 were admitted or referred to the Paediatric Cardiology Outpatient Clinic in Okmeydanı Training and Research Hospital at Health Sciences University between April 2017 and March 2018. Ethics committee approval was obtained for this study (Approval #: 2017:754). Written informed consent was taken from the parents of the patients. The study was performed in accordance with the declaration of Helsinki.
Patients
All consecutive patients who were admitted or referred to the paediatric cardiology outpatient clinic with the complaint of chest pain were evaluated using a prospective database. Patients with prior chronic cardiac diseases, including previous cardiac surgery, dysrhythmias and CHD or acquired heart disease and the patients and parents who refused to participate in the study were excluded.
Variables
Demographic characteristics and clinical features of the patients such as age, sex and body mass index (kg/m2) were recorded. They were grouped based on age (<12 and ≥12 years) and body mass index (<18.5 kg/m2 underweight, 18.5–24.9 kg/m2 normal and ≥25 kg/m2 overweight). Medical and family history and the clinical features of chest pain such as onset, duration, frequency, localisation, quality, association with effort, seasonal and monthly distribution, and radiation patterns were also questioned. Presence of sudden onset, well-localised pain, predominantly at rest and aggravated by deep breathing, lasting from 30 seconds to 3 minutes, was diagnosed as precordial catch syndrome.Reference Collins, Griksaitis and Legg10 Presence of a diagnosed cardiac disease in a first-degree relative was regarded as the positive family history.
Pathological findings in the physical examination were recorded, including any deformity or tenderness on the chondrosternal or costochondral junctions, murmur, gallop, pericardial rub, abnormal heart sounds on cardiac auscultation, hepatomegaly, decreased peripheral pulses, peripheral oedema and painful or swollen extremities.
All patients underwent 12-channel electrocardiography and transthoracic echocardiography. Abnormal electrocardiography findings included ventricular hypertrophy, early repolarisation, atrial enlargement, bundle branch or atrioventricular blocks and abnormal ST, T or PR waves. Echocardiography results were based on the paediatric cardiologist’s notes.
Diagnostic categories
After a detailed evaluation of the patients, diagnostic categories in the aetiology of chest pain were grouped as cardiac, musculoskeletal, precordial catch syndrome, respiratory, gastrointestinal, psychogenic, idiopathic and miscellaneous.
Potential cardiac causes of chest pain, including anomalies of the coronary arteries, cardiomyopathies, myocarditis, pulmonary hypertension, aortic dissection, valve anomalies and left ventricular outflow obstruction were noted. Musculoskeletal origin was diagnosed in the presence of tenderness on the chest wall, aggravation of pain during inspiration, muscle strain, development of pain with movement and tenderness on palpation over the costochondral junctions.Reference Chun, Kim, Han, Kim and Yoon5 Patients with predominantly respiratory symptoms (i.e., presence of chest pain secondary to acute onset of cough or asthma with recent wheezing) and gastrointestinal symptoms (i.e., an association of pain with indigestion, heartburn or vomiting) were referred to the paediatric pulmonary diseases and gastroenterology outpatient clinics, respectively. Diagnoses in these clinics were regarded as the final diagnostic category. Consultation of paediatric psychiatry was requested in the absence of any diagnostic category or at the discretion of the attending physician considering the history of psychological findings. Diagnostic and Statistical Manual of Mental Disorders-5 diagnostic criteria were used in the psychiatric evaluation. Beck Anxiety Inventory and the Beck Depression Inventory were applied to the patients at the discretion of the paediatric psychiatrist.Reference Irak and Albayrak11,Reference Khairandish, Jamali and Haghbin12 After a detailed clinical evaluation, patients without any causes to explain chest pain were considered as idiopathic.
Expectations of the parents and patients
To investigate their expectations about the diagnoses, attending physicians questioned the patients and their parents, who were blinded to the possible diagnosis, about the cause of chest pain. The responses of children who were able to make a fair assessment, as judged by their age, were considered. For a comparison of the expectations of the parents and the patients, we grouped the diagnostic categories as cardiac and non-cardiac (including musculoskeletal, precordial catch syndrome, respiratory, gastrointestinal, psychogenic, idiopathic and miscellaneous).
Statistical analysis
Descriptive statistics were given as mean ± standard deviation for continuous variables or as numbers and percentages for categorical variables. Normality of the numerical variables was checked with the Kolmogorov–Smirnov test. In the comparison of two independent groups, independent samples t-test was used where numerical variables had a normal distribution. One-way analysis of variance was used for comparisons of more than two independent groups where numerical variables had a normal distribution. The Tukey test was used to detect differences between the groups. For comparison of differences between categorical variables, Pearson chi-square test was used in 2 × 2 tables and Fisher–Freeman–Halton test was used in R×C tables. For statistical analysis, Jamovi (Version 1.0.7), JASP (Version 0.11.1) and the Statistical Package for Social Sciences (SPSS Statistics for Windows, Version 22.0; IBM Corp., Armonk, NY, USA) were used. The significance level (p value) was set at 0.05 in all statistical analyses.
Results
Patients
The study included a total of 782 patients with a mean age of 12.02 ± 3.16 years. Although there were more female patients (53.6%) presenting with chest pain in the study group and age of female patients was higher than that of male patients (12.25 ± 3.2 years and 11.75 ± 3.1 years, respectively), other demographic features were similar in both female and male patients (p > 0.05 for all). Demographic features of the patients were shown in Table 1. Positive family history for any type of chronic cardiac diseases was found in 100 patients (12.8%).
Table 1. Demographic features of the patients

BMI = body mass index.
Description of the pain
Features of the chest pain were summarised in Table 2. One to six months before admission was the most common time interval for the onset of chest pain (386 patients, 49.4%). The frequency of visits was almost similar throughout the year except for fewer admissions in the summer. The highest number of admissions in the 12-month period was in October (n = 128, 16.4%). Duration of chest pain varied from 0–1 minute to >60 minutes; it lasted 1–10 minutes in 370 patients (47.3%). Location of the pain was at the left side of the chest in more than half of the patients (66.1%). Stabbing (stitch) pain was detected in 328 patients (41.8%). In almost more than 95% of the cases, the pain was developed during resting. There were 104 patients (13.3%) with the diagnosis of precordial catch syndrome based on the clinical features of the chest pain.
Table 2. Characteristics of the patients’ chest pain

Medical history
There was a previous diagnosis of asthma in 52 patients (6.6%). Other chronic diseases such as gastroesophageal reflux disease/peptic ulcer/gastritis and familial Mediterranean fever were reported in 27 (3.5%) and 11 patients (1.4%), respectively.
Physical examination
Physical examination revealed costochondral tenderness leading to a diagnosis of costochondritis, thelarche/gynaecomastia and scoliosis in 27 (3.5%), 14 (1.8%) and 1 (0.1%) patients, respectively. There were two chest-wall deformities: pectus excavatum and pectus carinatum, each in one patient. Wheezing and crackle breathing sounds were auscultated in 65 patients (8.5%). Pathological murmur was detected only in one patient.
Diagnostic tests
Electrocardiographic and echocardiographic evaluations revealed abnormal findings in 9 (1.2%) and 60 patients (7.7%), respectively (Table 3). Mitral insufficiency (trace and mild) was the most common pathological echocardiography finding detected in 46 patients.
Table 3. Pathological electrocardiographic and echocardiographic findings

* 72 pathologies in 60 patients.
Diagnostic categories
Musculoskeletal chest pain and psychogenic causes were the most commonly detected aetiological categories in 258 (33%) and 222 (28.4%) patients, respectively. There were non-cardiac causes in 99% of the cases (n = 774). Eight patients (1%) had chest pain due to cardiac causes including mitral valve prolapse (n = 4), dissection of the aorta (n = 1), mitral valve prolapse and mitral failure (n = 1), pulmonary hypertension (n = 1) and rheumatic stenosis of the mitral valve (n = 1). Other disease categories were detailed in Table 4.
Table 4. Aetiological classification of the causes of chest pain and comparison based on sex
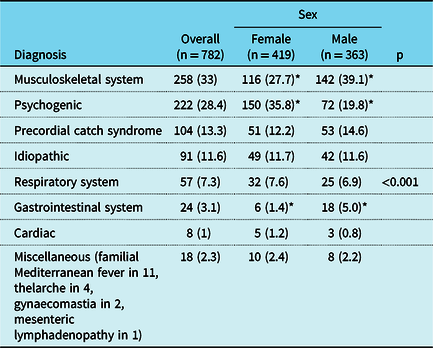
* Significant.
Beck Depression and Anxiety Scales were applied to 63 of 222 patients with a psychogenic origin of pain (28.4%). Among psychogenic causes, generalised anxiety disorder and depression of any severity were the most common disorders in 117 (52.7%) and 83 (37.4%) patients, respectively. Other psychogenic causes were panic disorder (n = 8, 3.6%), phobia (n = 7, 3.2%), post-traumatic stress disorder (n = 3, 1.3%), obsessive-compulsive disorder (n = 2, 0.9%) and attention deficit and hyperactivity disorder (n = 2, 0.9%).
Although the diseases of musculoskeletal and gastrointestinal systems were more commonly seen in male patients, there were more psychogenic disorders in female patients (p < 0.001 for all) (Table 4). For cardiac diseases, there was no significant difference between female and male patients. There was also no significant difference between the diagnostic categories in patients with (n = 100) and without (n = 682) positive cardiac family history (p = 0.371).
Significant differences were found between the total seasonal number of admissions and the number of admissions by age (p < 0.001) (Table 5). The average age of the patients admitted in winter and the number of patients ≥12 years of age admitted in winter were higher than those in the other seasons (p < 0.001 for both).
Table 5. Seasonal distribution of the cases
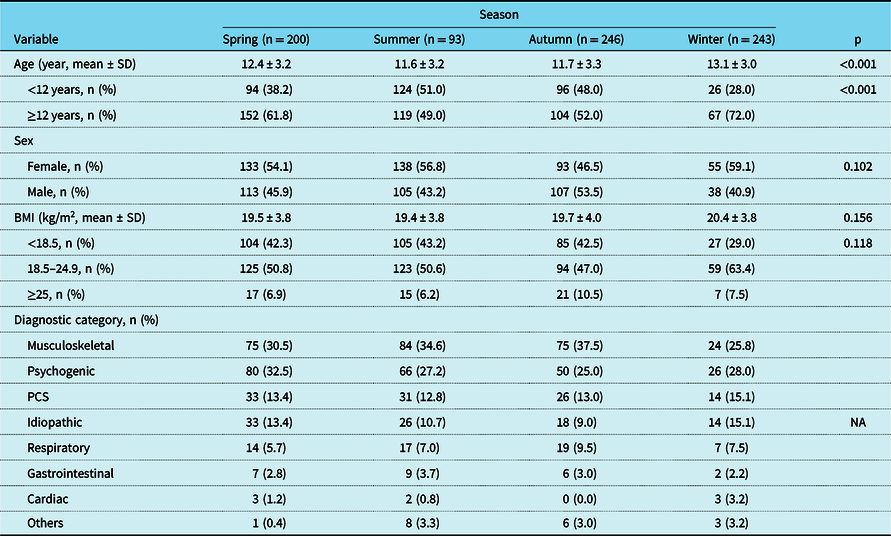
BMI = body mass index; PCS = precordial catch syndrome; NA = not applicable.
The expectations of the parents and patients
There were 663 patients (84.8%) who responded to the questions regarding their expectations about the outcome. While 70.8% of the parents thought that the chest pain in their children was caused by cardiac causes, this rate was 90.2% in children (Table 6). For both the patients and their parents, the rate of those suspecting a cardiac aetiology of chest pain was higher than the final diagnostic outcome.
Table 6. Comparison of the diagnostic outcome (cardiac versus non-cardiac) and the causes of chest pain suspected by the patients and their parents

Discussion
In the present study, we showed that non-cardiac causes, including musculoskeletal and psychogenic causes, were the most common diagnostic categories for children with chest pain. Although the patients and their parents thought that cardiac causes were responsible for chest pain in a majority of the cases, cardiac causes were involved in the aetiology of chest pain only in 1% of the patients.
In previous studies, the incidence of cardiac diseases in children with chest pain has varied between 0.6 and 9.27%.Reference Mohan, Nandi, Stephens, M’Farrej, Vogel and Bonafide6,Reference Gesuete, Fregolent, Contorno, Tamaro, Barbi and Cozzi8,Reference Khairandish, Jamali and Haghbin12–Reference Lin, Lin, Ho and Chang17 The incidence and the types of cardiac diseases vary greatly based on the type of centre (i.e., emergency department, primary care or paediatric cardiology outpatient clinic). Saleeb et al.Reference Saleeb, Li, Warren and Lock14 reported that there were only 37 cardiac causes in a cohort of 3700 patients from a children’s hospital, corresponding to a rate of 1%. In their study, unknown and musculoskeletal causes were detected in 52 and 36% of the cases, respectively. However, Cohn et al.Reference Cohn and Arnold15 reported an incidence of 2.5% for cardiac diagnoses in a study with 203 patients in a paediatric cardiology clinic. In this study, they demonstrated that arrhythmias and mitral valve prolapse were directly related to chest pain. However, myocarditis and pericarditis have also been shown as major causes of chest pain in children.Reference Kane, Friedman, Fulton, Geggel and Saleeb18 In Friedman’s study, 16 pericarditis and arrhythmias were the causes of chest pain. Drossner et al.Reference Drossner, Hirsh and Sturm13 reported their experience at an emergency department and found that arrhythmias, myocarditis, pericarditis and acute myocardial infarction were the cardiac causes. However, we detected mostly mitral valve pathologies, including mitral valve prolapse and rheumatic stenosis of the mitral valve. In addition, we found aortic dissection and pulmonary hypertension each in one patient only. Sert et al.Reference Sert, Aypar, Odabas and Gokcen7 also reported similar incidental cardiac findings. Concerning the absence of serious, life-threatening cardiac pathologies such as arrhythmias, myocarditis, pericarditis and acute myocardial infarction, the prospective data collection may be an important factor enhancing the reliability of the results. As we cannot explain the presence or absence of such pathologies in each study, there should be more observational studies about cardiac pathologies leading to chest pain in children. The use of different search methodologies (i.e., different diagnostic codes) might have led to a selection bias in the studies.
Significant differences were also found in the demographic features of children with chest pain. Although some studies have reported that children presenting with chest pain are usually female with a mean age of around 10 years,Reference Drossner, Hirsh and Sturm13,Reference Kim, Shin, Kim, Lee and Nam19 other studies indicated higher presentation in males or females over 12 years of age and in pubertal children.Reference Friedman and Alexander3,Reference Gesuete, Fregolent, Contorno, Tamaro, Barbi and Cozzi8,Reference Hanson and Hokanson20–Reference Geggel22 In the present study, there were more females and children >12 years of age. Such differences probably originate from the characteristics of different studies.
Several authors have investigated the association between exertion and chest pain.Reference Perry, Zha, Oster, Frias and Braunstein23 It has been reported that chest pain occurred predominantly during resting, ranging from 37 to 56%.Reference Saleeb, Li, Warren and Lock14,Reference Friedman, Kane and Rathod16 Cohn et al.Reference Cohn and Arnold15 reported that chest pain appeared during exertion in 22.7% of the patients and did not show an association between exertional chest pain and cardiac aetiology. Perry et al.Reference Perry, Zha, Oster, Frias and Braunstein23 showed that exertional chest pain was negatively associated with cardiac aetiology. In the present study, chest pain was reported to develop only at rest in 92.6% of the cases. Although this rate was higher than in other studies, several factors might be affecting this finding. Future prospective studies focusing on the perception of pain are needed to clarify this matter.
A good anamnesis and physical examination are essential in revealing the aetiology in children and adolescents with chest pain.Reference Sert, Aypar, Odabas and Gokcen7,Reference Kim, Shin, Kim, Lee and Nam19,Reference Daşkapan, Şanlı, Aydoğan-Arslan, Çiledağ-Özdemir, Korkem and Kara24 If necessary, auxiliary investigations such as telecardiography, electrocardiography and echocardiography should be performed to exclude other possible causes. The patients are expected to have abnormal findings during the physical examination if the underlying cause of chest pain is a serious organic disease.Reference Mohan, Nandi, Stephens, M’Farrej, Vogel and Bonafide6 However, it has been reported that more than two-thirds of patients with coronary anomalies are without any pathological finding.Reference Kane, Friedman, Fulton, Geggel and Saleeb18 An echocardiographic evaluation has been recommended if the history, physical examination and electrocardiography are suggestive of a possible cardiac aetiology. However, it has been known that the use of echocardiogram in a patient with chest pain may help identify cardiac pathologies even if the history, physical examination and electrocardiography are negative for cardiac diseases.Reference Drossner, Hirsh and Sturm13,Reference Kane, Friedman, Fulton, Geggel and Saleeb18 In Cohn’s studyReference Cohn and Arnold15, the use of electrocardiography, echocardiography and 24-hour ambulatory electrocardiography monitoring confirmed the suspected cardiac diagnoses of five patients with chest pain. Although such an approach might be regarded as unnecessary, especially in silent cases, an echocardiographic evaluation may lead to a more accurate diagnosis. Similar to our results, they could not find the underlying cause of chest pain (idiopathic) in 12–73.6% of children and adolescents.Reference Chun, Kim, Han, Kim and Yoon5,Reference Saleeb, Li, Warren and Lock14,Reference Cohn and Arnold15,Reference Hanson and Hokanson20,Reference Rowe, Dulberg, Peterson, Vlad and Li25 In Lin’s study,Reference Lin, Lin, Ho and Chang17 idiopathic chest pain was found to be the most common diagnosis. In this study, additional diagnostic tests, including echocardiogram, were performed only in 64.1% of the cases, which might have led to such unexpectedly high rates in idiopathic cases. Several algorithms have been proposed for evaluation of children with chest pain to eliminate invasive testing and to save resources.Reference Saleeb, McLaughlin, Graham, Friedman and Fulton4,Reference Mohan, Nandi, Stephens, M’Farrej, Vogel and Bonafide6,Reference Friedman, Kane and Rathod16,Reference Kane, Friedman, Fulton, Geggel and Saleeb18 However, we believe that it is better to eliminate the concerns of the patient and the family that the pain is caused by cardiac problems. For that purpose, we used echocardiography in all children with chest pain as a policy of our paediatric cardiology clinic.
Musculoskeletal pathologies have been known as one of the major diagnostic categories for non-cardiac chest pain. In previous studies, up to half of the patients with chest pain have been shown to have musculoskeletal problems causing chest pain in childhood period in contrary to Lin’sReference Lin, Lin, Ho and Chang17 and Khairandish’sReference Khairandish, Jamali and Haghbin12 study in which musculoskeletal causes were found to be responsible for only 6.7 and 7.7% of the cases, respectively.Reference Khairandish, Jamali and Haghbin12–Reference Cohn and Arnold15 They explained this discrepancy with the exclusion of all trauma-associated chest pain cases. In our study, musculoskeletal system-related chest pain was detected in 33% of the patients. Precordial catch syndrome has been seen in up to 14.2% of the cases similar to the present study (13.3%).Reference Sert, Aypar, Odabas and Gokcen7,Reference Gumbiner26 However, some authors included precordial catch syndrome in musculoskeletal diagnostic category contrary to the approach in this and other studies.Reference Sert, Aypar, Odabas and Gokcen7,Reference Cohn and Arnold15 This differentiation may explain the differences in their studies. It has also been suggested that the evaluation of the musculoskeletal system with a focus on the pectoralis minor shortness, rounded shoulder and thoracic kyphosis was critical to differentiate cardiac and non-cardiac aetiologies.Reference Daşkapan, Şanlı, Aydoğan-Arslan, Çiledağ-Özdemir, Korkem and Kara24 Therefore, careful medical-history taking and detailed physical examination are essential factors to reach accurate diagnoses.
Psychogenic chest pain is thought to be another problematic issue in children and especially in adolescents. Several authors reported higher rates of psychogenic causes than organic causes as the aetiology of chest pain in children.Reference Eliacik, Kanik and Bolat27 KhairandishReference Khairandish, Jamali and Haghbin12 analysed the patients aged 11–18 years and found the psychological causes to be the second most common cause for chest pain. In McDonnell’s review,Reference McDonnell, White and Grady28 it has been reported that 2–19% of chest pain cases were categorised as psychological. In Achiam-Montal’s study,Reference Achiam-Montal, Tibi and Lipsitz29 panic disorders were found in 20.5% of the patients with chest pain. They reported that comorbid anxiety and depressive symptoms were also common. We detected psychogenic reasons only in 24.8% of the patients and found that depression and anxiety were major causes among psychogenic diseases. In other studies, however, depression and anxiety were found to be present in 45.9 and 67.5% of the patients who were aged 11–18 years, respectively.Reference Khairandish, Jamali and Haghbin12 Based on the higher incidences for psychogenic causes in adolescents, consultation of paediatric psychiatry is important to evaluate the patients who are suspected for psychological aetiology.Reference Kenar, Örün, Yoldaş, Kayalı, Bodur and Karademir30
It is logical to suspect that the diseases of the gastrointestinal system underlie the chest pain if the pain is related to eating, sleep and unfavourable dietary habits. It has also been found that epigastric pain and nausea/vomiting/regurgitation were the significant symptoms for children with erosive gastritis in association with non-cardiac chest pain.Reference Park, Choi and Jeong31 As the pain was related to eating and lying on the back, gastrointestinal aetiology was detected in 3.1% of the cases. Although similar incidences were reported for gastrointestinal system diseases in the aetiology of non-cardiac chest painReference Lin, Lin, Ho and Chang17, Kim et al.Reference Kim, Shin, Kim, Lee and Nam19 found that the oesophageal and gastric diseases were responsible for chest pain in 48 of 75 children (64%) with non-cardiac chest pain. In their series, reflux oesophagitis was the most common disease (27 out of 57 with endoscopy). Almost half of the patients improved with medicines; however, abnormalities in cardiac examinations were present in 35.1% of these cases, which necessitated further follow-up and additional testing. The results of this study should be considered with caution due to the impact of geographical variations and higher incidences of upper endoscopy. Therefore, careful history taking helps physicians to diagnose such diseases.
In the present study, we have shown a significant association between seasonal admissions and the age of the patients. However, we have difficulty in explaining the finding that patients with higher ages admitted more frequently in winter months. Anxiety for school success and exam stress may be an important factor for higher rates of admission, especially in prepubertal children and adolescents.
In this study, we also evaluated the anticipations of patients and their parents about the possible causes of chest pain. Most of the parents and the patients thought that cardiac reasons could underlie chest pain. However, diagnostic results indicated that a high level of anxiety was the most common underlying factor. Although it has been thought that protective and encouraging/monitoring behaviour of parents may magnify the impact of non-cardiac chest pain in children, further studies are needed to evaluate these expectations about the probable causes of chest pain.Reference Achiam-Montal and Lipsitz32
Prospective nature of the study was the main strength of the study. Evaluation of patients in a paediatric cardiology clinic was another advantage for our results. The questionnaire was used only as a collection tool for the responses of parents and patients, and it did not provide information about the cause-and-effect relationship. Such a situation prevented us from evaluating the possible factors to cause such outcomes far from the final diagnoses. In addition, the number of patients with cardiac aetiology was rather small to reach more refined conclusions. In this study, there were no data about the follow-up of these patients to be sure about our diagnoses and progression or regression of chest pain. Large-scale observational studies with more extended follow-up periods are needed to clarify contentious aspects.
In conclusion, chest pain due to cardiac diseases is rarely seen in childhood. Most of the diagnoses for chest pain are benign and include the musculoskeletal system and psychogenic diseases. However, a comprehensive analysis including thorough history-taking, detailed physical examination and cardiac imaging with echocardiography is needed to reach more accurate diagnoses.
Acknowledgements
None.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflict of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the institutional committees (Ethical Committee of Okmeydanı Training and Research Hospital, Health Sciences University, Approval # 2017:754).






