


Introduction
Korsakoff's syndrome is a neurological disorder, caused by chronic thiamine deficiency because of alcohol abuse, resulting in lesions in the diencephalon, particularly the mammillary bodies and the thalamus (Reference Visser, Krabbendam and Verhey1), and frontal lobe dysfunction (Reference Reed, Lasserson and Marsden2). Next to a severe anterograde and a substantial retrograde amnesia, these patients display neuropsychiatric symptoms and have impaired social cognitive functioning. For example, Korsakoff patients have difficulties in recognising emotional expressions in the faces of others (Reference Montagne, Kessels and Wester3), perform poorly on affective prosody recognition (Reference Snits, Hellinger and Daum4) and display impaired social inference ability (Reference Corcoran5). Other behavioural symptoms are apathy, disinterest, loss of initiative, lack of insight and a decreased social desirability (Reference Egger, Wester and De Mey6).
One important aspect of social cognition is the ability to understand and to consider other people's knowledge, thoughts and feelings, often referred to as perspective taking or mentalising, an important aspect of theory of mind (ToM) (7,8). It has been suggested that perspective taking is subserved by the prefrontal cortex (Reference D'Argembeau, Ruby and Collette9), but the underlying mechanisms are under debate. Also, perspective taking may be highly dependent on executive functions (Reference Samson, Apperly and Humphreys10). There is some evidence for deficits in perspective taking in chronic alcoholism (Reference Uekermann and Daum11). In Korsakoff patients, studies on perspective taking are lacking altogether, although impaired metaphoric processing in Korsakoff patients has been linked to the concept of perspective taking (Reference Corcoran5). A complicating factor is that in Korsakoff's syndrome, executive deficits are prominent as well (Reference Van Oort and Kessels12–Reference Kessels, Kortrijk and Wester14). Possibly, executive deficits may be directly related to the impaired performance reported on social inference tasks. The aim of this study was to examine perspective taking in Korsakoff patients, taking task complexity and executive functioning into account.
Methods
Participants
Twenty-three patients (17 males) fulfilling the DSM-IV–TR criteria (15) for alcohol-induced persisting amnestic disorder and the criteria for Korsakoff syndrome (Reference Kopelman16) were studied. All had been admitted to the Korsakoff Clinic of the Vincent van Gogh Institute for Psychiatry in Venray, The Netherlands, after having sustained an acute Wernicke's psychosis more than 2 months prior to the investigation. All patients were in the chronic, amnesic stage of the syndrome; none of the patients was in the confusional phase at the moment of testing. All patients were diagnosed by experienced neuropsychologists and psychiatrists on the basis of clinical, psychiatric and neuropsychological examinations (including signs such as confabulation behaviour and anterograde amnesia). All patients were alcohol-abstinent since their admittance to the clinic (i.e. more than 2 months). None of the patients fulfilled the clinical criteria for alcohol dementia (Reference Oslin, Atkinson and Smith17), i.e. all patients had preserved intellectual abilities as measured with the Wechsler Adult Intelligence Scales-third edition (WAIS-III) (Reference Wechsler18) or the abbreviated Groninger Intelligence Test (Reference Luteijn and Van der Ploeg19) that were administered as part of routine neuropsychological testing after admission to the clinic (Table 1).
Table 1 Demographic variables and performance on the neuropsychological tests (a higher score means a better performance; mean + SD) for the Korsakoff patients and the healthy controls
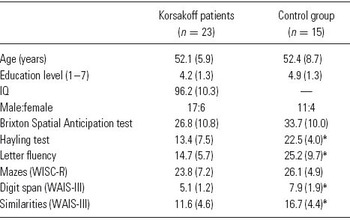
* p < 0.01.
Fifteen healthy control participants (11 males) were matched on age and educational level. Healthy controls were selected from a database of Utrecht University and were paid for their participation. The study was approved by the local ethics committee and written informed consent was obtained from all participants in accordance with the declaration of Helsinki. Education level was coded with an ordinal rating scale which consists of seven categories (1 being the lowest, less than primary school and 7 the highest, academic degree). Table 1 shows the demographic variables of both the patient group and the controls. Patients and controls did not differ in age (t(36) = −0.13, p = 0.90), educational level (Mann–Whitney U = 126.5, p = 0.17) and sex distribution (X 2(1) = 0.002, p = 0.97).
Materials and procedure
Neuropsychological assessment
The following executive function tests were used: letter fluency (Reference Luteijn and Van der Ploeg19) (naming of words beginning with ‘N' or ‘A', one minute for each letter), the Mazes subtest of the Wechsler Intelligence Scale for Children – Revised (WISC-R) (Reference Wechsler20), the Brixton Spatial Anticipation test (Reference Burgess and Shallice21) and a Dutch translation of the Hayling test (Reference Burgess and Shallice21), administered without time restriction, assessing response generation, planning, rule detection and response inhibition respectively. The Digit Span subtest of the WAIS-III (Reference Wechsler18) was administered as an index of working memory. Finally, the Similarities subtest of the WAIS-III was used to measure verbal comprehension (Reference Wechsler18,Reference Ward, Ryan and Axelrod22).
Story comprehension task
A story comprehension task was developed to assess perspective-taking abilities. By incorporating questions testing the ability to appreciate others' mental states, story comprehension tests have proven to be valid measures of ToM processes (23,24). Stories requiring perspective taking are commonly contrasted to physical stories that are matched on sentence length and complexity and that do not require the appreciation of others' mental states (Reference Mar24), in order to isolate the specific ToM functions. This approach was adopted in this study. The story comprehension task consisted of 21 textual stories, and each story was followed by questions (in total 51). Stories about everyday events, actions and concepts were developed. The mean story length was 50 words. The number of questions in connection with one story differed from two to four questions per story. The questions connected to one story were independent, meaning that the correct answer to one question was not part of the reasoning process with respect to the other questions. Fifteen perspective-taking questions and 15 non-perspective-taking questions were developed. For the perspective-taking questions, participants had to infer the feelings, ideas or knowledge of a character in the story. Non-perspective-taking questions required inferences about causes or consequences related to objects and concepts, or to feelings or ideas that were already defined in the text. To control for potential confounding factors such as difficulties in reading and memorisation of a story that may aversely affect inferential reasoning, one factual question was asked after every story. In these questions details were asked which could be literally abstracted from the text, requiring no inferential reasoning. Furthermore, both non-perspective-taking questions and perspective-taking questions were divided into three levels of complexity. Complexity was defined here as the minimum number of propositions (expressed in a sentence) and inferences together that are needed to correctly answer a question in connection with a written story (for examples see Appendix). To control for subjectivity in the determination of the number of elements to be integrated in answering a question, a pilot study was performed in which five healthy participants were asked independently to say aloud all steps they took when answering a question.
The stories were presented in front of the participants one by one. The stories and the questions were printed in a large typeface on separate papers. Next to the paper version that was presented, the experimenter also read the whole story aloud once. The story was visible during the question–answering phase as well. Participants were told that they were allowed to read the stories as often as they wanted in order to prevent a confounding effect of memory function on story comprehension performance. Subsequently, the questions about the story were presented one by one and were also read aloud once by the experimenter. The experimenter wrote down the answers of the participants. An answer was scored as correct (score 1) or incorrect (score 0). When the participants simply answered ‘yes' or ‘no', they were asked why they came to that conclusion to prevent correct answers by guessing.
Procedure and statistical analyses
Participants were tested individually. The tasks were presented to patients and controls in a fixed order. Each test session took between 1 and 1.5 h. Student t-tests were performed to examine potential group differences in neuropsychological test performance. For the subsequent analyses, the raw scores of all executive tasks were transformed into standardised z-scores based on the performance of the controls, and combined into one compound score for executive function.
To examine possible perspective-taking deficits in the Korsakoff patients, a repeated measures analysis of variance (ANOVA) was carried out with group (controls vs. patients) as between-subject factor, and complexity (three levels: two, three or four elements) and perspective taking (perspective taking vs. non-perspective taking) as within-subject factors. Next, Pearson correlations (one-sided) were calculated between the executive function, working memory (Digit Span) and verbal comprehension (Similarities) scores on one hand and the total story comprehension score on the other hand. To examine the association of perspective taking and complexity with executive functioning in the Korsakoff patients, a repeated measures ANOVA was carried out with group as between-subject, and complexity and perspective taking as within-subject factors and working memory, executive function and verbal comprehension as covariates.
Results
Table 1 shows the results for the patients and controls on the tests of executive functioning, working memory and verbal comprehension. Patients performed significantly worse than controls on most executive function tests (p = 0.057 for the Brixton Spatial Anticipation test), as well as on the working memory and verbal comprehension tasks. Figure 1 shows the performance of the patients and the controls on the story comprehension task for the perspective-taking and non-perspective-taking questions at different levels of complexity.

Fig. 1. Mean scores (+SEM) for the Korsakoff patients (KS) and controls (CON) on the story comprehension task for perspective-taking and non-perspective-taking questions of three levels of complexity (2, 3 or 4 steps).
The repeated measures analysis revealed a main effect of group (F(1,36) = 39.91, p < 0.001, η p2 = 0.53), indicating overall worse performance of the patients compared to the controls. Furthermore, a main effect of complexity was found (F(2,72) = 40.44, p < 0.001, η p2 = 0.53). Post hoc comparisons revealed that, overall, performance decreased when complexity increased (two and three elements: p < 0.001, three and four elements: p < 0.01). The main effect of perspective taking just failed to reach significance (F(1,36) = 3.51, p = 0.07, η p2 = 0.09), indicating that, although performance was diminished on the perspective compared to the non-perspective-taking questions, this difference was not significant. A significant interaction effect between group and complexity was found (F(2,72) = 7.05, p < 0.01, η p2 = 0.16), revealing a more pronounced decline in story comprehension with increasing task complexity in the Korsakoff patients compared to the controls. Finally, a significant interaction was found between complexity and perspective taking (F(2,72) = 7.71, p < 0.001, η p2 = 0.18), indicating that an increase in complexity affected performance on the perspective-taking questions more than performance on the non-perspective-taking questions. Although performance did not differ between the perspective-taking and non-perspective-taking questions at the two- and three-element levels (t(37) = 1.07, p = 0.29 and t(37) = −1.66, p = 0.10, respectively), performance was significantly diminished on the four-element perspective compared to the non-perspective-taking questions (t(37) = 3.86, p < 0.001). This effect was found in both the control group (t(14) = 3.06, p < 0.01) and the Korsakoff patients (t(22) = 2.70, p = 0.013). No significant interaction effect was found between perspective taking and group (F(1,36) = 0.54, p = 0.47, η p2 = 0.01) or perspective taking, complexity and group (F(2,72) = 1.90, p = 0.16, η p2 = 0.05).
The patients performed worse than the controls on the factual knowledge questions of the story comprehension task (mean performance of the patients was 19.6, SD = 1.8 and of the controls 21.0, SD = 0.0; t(36) = −3.65, p < 0.01). Nonetheless, most patients (n = 21) performed very well on these questions (i.e. >85% correct). When we repeated the analysis while excluding two patients with diminished factual knowledge performance (i.e. 14 and 16 correct answers), the results did not change significantly.
Pearson correlations revealed that the total story comprehension score was significantly associated with executive function (r = 0.38, p < 0.05), working memory (r = 0.40, p < 0.05) and verbal comprehension (r = 0.67, p < 0.01) in the Korsakoff patients. In the control group, a similar trend was noted for the relationship with executive function (r = 0.37, p = 0.09) and verbal comprehension (r = 0.50, p < 0.05), but not for working memory (r = −0.04, p = 0.44). We, therefore, examined whether executive function and verbal comprehension (but not working memory, which would violate the parallelism assumption) could account for the interaction between group and complexity. This was accomplished by running an ANOVA with group as between-subject variable, and complexity and perspective taking as within-subject variables, while adjusting for executive function and verbal comprehension. In line with the previous results, significant main effects of group (F(1,32) = 10.11, p < 0.01, η p2 = 0.24) and of complexity (F(2,64) = 3.47, p < 0.05, η p2 = 0.10) were found. Furthermore, a significant effect of verbal comprehension was found (F(1,32) = 14.72, p < 0.01, η p2 = 0.32). A significant interaction was found between complexity and executive function (F(2,64) = 3.77, p < 0.05, η p2 = 0.11), but not between complexity and verbal comprehension (F(2,64) = 0.77, p = 0.47, η p2 = 0.02). The interactions between complexity and perspective taking (F(2,64) = 0.16, p = 0.86, η p2 = 0.00), and group and complexity (F(2,64) = 0.40, p = 0.67, η p2 = 0.01) were no longer significant. When we reran the analyses while controlling for either executive function or verbal comprehension, it became clear that executive function mediated the interaction between group and complexity (i.e. the interaction was still significant after controlling for verbal comprehension, but not after controlling for executive function). This implies that executive functions mediate the interaction in which the Korsakoff patients performed disproportionately worse with an increase in task complexity. No further significant effects were found.
To summarise, the results indicate, first, that an increase in complexity affected perspective-taking more than non-perspective taking abilities in both controls and Korsakoff patients and, second, that executive function may be an important mediator of the decline in story comprehension with increasing task complexity. To examine the mediating role of executive function in the relationship between complexity and perspective taking in more detail, correlations were calculated between executive function and perspective-taking performance while distinguishing between the different complexity levels. As the effect of complexity on perspective-taking performance was similar in both groups, we combined the data of the control group and the Korsakoff patients. This analysis (Fig. 2) revealed a small non-significant association between executive function and the two-element questions (r = 0.25, p = 0.13), a medium correlation with the three-element questions (r = 0.40, p < 0.05) and a large correlation with the four-element questions (r = 0.60, p < 0.01). The correlations of the two- and three-element questions with executive function performance did not differ significantly from each other (z = −0.7, p = 0.24) and neither did the correlations of the three- and four-element questions (z = −1.1, p = 0.14); however, a significant difference was found between the correlations of the two- and four-element questions (z = −1.8, p < 0.05). Taken together, these correlations show a positive increase in the association between executive functioning and perspective-taking ability with increasing task complexity.

Fig. 2. Correlations between performance on the executive function tests and the perspective-taking questions.
Discussion
The aim of this study was to examine the performance of a group of Korsakoff patients on a task assessing perspective taking, in relation to task complexity and executive functioning. The most important finding of this study is that, in our sample of Korsakoff patients, no specific deficits in perspective taking were found. There was no overall difference in performance between perspective-taking and non-perspective-taking questions in either the Korsakoff group or the controls. Instead, the ability of Korsakoff patients to answer a question about a story correctly depends on task complexity, i.e. the number of inferential reasoning steps that have to be taken, in order to answer the question. This complexity-related decline in performance was more pronounced in Korsakoff patients than in healthy controls. Also, the disproportional complexity-related decrease in performance of the Korsakoff patients was clearly the result of an overall executive dysfunction; after controlling for the performance on a constellation of standardised neuropsychological executive function tests, the disproportional complexity-related decline in the Korsakoff group disappeared. The Korsakoff group performed worse on the factual questions of the stories, measuring reading ability and memorisation of a story, which may have potentially biased our results. However, the patients answered 93% correctly, compared to a 100% score of the control group on the factual knowledge questions. Thus, it is unlikely that this slightly worse performance in reading ability and memorisation of a story could explain the overall worse performance on the questions that relied on inferential reasoning.
In this study, executive functions mediated the finding that story comprehension decreased disproportionately with increasing task complexity in the Korsakoff patients. Although we cannot rule out the possibility that Korsakoff patients have deficient perspective-taking abilities, our findings clearly indicate that in our patient group executive functioning, instead of perspective taking, determines story comprehension performance. For one, the pattern of task performance on the story comprehension task was comparable between both groups. When comparing the perspective taking with the non-perspective-taking conditions, both groups performed significantly worse on the perspective-taking stories only at the highest level of complexity. Also, executive functions were strongly correlated with perspective-taking abilities at this highest level of complexity, but not with these abilities on the easiest condition, in which both groups revealed comparable performance on the perspective-taking and the non-perspective-taking tasks. If a genuine decline exists in perspective-taking abilities in the Korsakoff patients, which extends beyond deficits in executive functions, then one would expect a significant decline in performance on all perspective-taking questions regardless of the level of task complexity. More specifically, this decline should be present in the easiest condition (i.e. the two-step questions) in which performance on the perspective-taking questions was unrelated to executive functions. Such a pattern of performance was, however, not observed.
One could argue that, instead of a decline in executive functions, a general decline in cognitive abilities in the Korsakoff patients accounts for these findings. However, the intellectual abilities of the Korsakoff patients were in the average range, indicating that intellectual skills were still unimpaired. Also, the complexity-related decline in performance on the story comprehension task was unrelated to verbal comprehension. Thus, the pattern of decline, in which story comprehension performance became more impaired with increasing levels of task complexity, was not the result of a verbal comprehension deficit, but appears to be specifically related to executive dysfunction. Although this does not exclude the possibility of a more general cognitive decline underlying our findings, the results together are strongly in favour of executive function as an important determinant of complex story comprehension ability in Korsakoff patients.
Social dysfunction observed in patients with frontal lobe dysfunction is often attributed to deficits in perspective taking, i.e. an inability to interpret behaviour of others in terms of underlying mental states, such as intentions, beliefs and desires (Reference Happé, Malhi and Checkley25). These findings clearly show, however, that in Korsakoff patients it is the complexity of the stories that underlies the impaired performance these patients show on perspective-taking tasks. The inability of Korsakoff patients in making inferences based on the stories is also directly related to impairments in executive functioning. Our findings are in agreement with previous findings relating executive functioning to performance on ToM tasks in patients with frontal lobe lesions (Reference Rowe, Bullock and Polkey26). In that study, a correlation between perspective taking and executive functioning was present in patients with left frontal lobe lesions. These findings in combination with the results of this study indicate that perspective taking depends on executive functions, such as planning, integrating, rule detection and concept shifting. In Korsakoff patients, these deficits in executive functioning may underlie poor performance on social inference tasks and not necessarily point towards a deficit in perspective taking.
Impaired ToM processes may have a profound negative effect on daily life functioning. For example, ToM processes have been found to predict social competence (Reference Couture, Granholm and Fish27) and to be associated with functional outcome (Reference Couture, Penn and Roberts28). An important implication of this study with regard to the role of executive function deficits in story comprehension performance is that in daily life the occurrence of perspective-taking problems can be prevented, i.e. in complex situations Korsakoff patients seem impaired in perspective taking, but this impairment may be diminished or even eliminated by reducing the complexity of the situation. For example, as multiple input sources (e.g. visual and auditory information) increase complexity, restricting a situation to a single source may increase perspective taking in these patients. This might eventually result in an increased ability to cope up with the demands of daily life, in which situations that require perspective-taking ability are often encountered. Future studies, however, are needed that specifically address the effect of reduced complexity on perspective taking in daily life situations.
To summarise, executive function deficits account for the diminished story comprehension performance, including perspective-taking abilities, in Korsakoff patients. Both in future studies and in clinical practice, executive functions should always be examined in relation to the possible underlying neurocognitive mechanisms of ToM deficits in general and perspective taking in particular.
Appendix
Appendix: examples of perspective-taking stories and non-perspective-taking stories
Example of a non-perspective-taking story
Mrs. de Vries goes to the park today. She does that every morning, if the weather is fine. If the weather is bad, she stays at home. She likes watching the children play and feeding bread crusts to the ducks. The past 3 days, it rained, although it's summer.
• Where to does Mrs. de Vries go this morning? (factual question)
• Answer: To the park.
• Where was Mrs. de Vries yesterday morning? (non-perspective-taking question)
1 She always goes to the park if the weather is fine.
2 It rained the past 3 days.
3 It rained yesterday.
4 The weather was not fine yesterday.
Answer: She did not go to the park yesterday.
• What kind of weather is it today? (non-perspective-taking question)
1 She always goes to the park if the weather is fine.
2 She goes to the park today.
Answer: It is nice weather today.
Example of a perspective-taking story
Daan has asked Michiel to a cinema evening. A good action movie was on, something they both like very much. Daan finds out that he has been wrong about the time the movie starts. The movie does not start at 8.30 p.m. but half an hour earlier. He forgets to tell Michiel this.
• What kind of movie are they going to? (factual question)
• Answer: An action movie.
• Does Michiel arrive in time at the cinema? (perspective-taking question)
1 The movie starts earlier.
2 Daan forgets to tell Michiel this.
3 Michiel thinks that the movie starts earlier than that the movie really starts.
Answer: No, he probably arrives too late.
• At what time does Michiel think the movie starts? (perspective-taking question)
1 Daan en Michiel first think the movie starts at 8.30 p.m.
2 Daan finds out he has been wrong about the time the movie starts.
3 Daan forgets telling Michiel this.
Answer: Michiel still thinks the movie starts at 8.30 p.m.
• At what time does the movie start? (non-perspective-taking question)
1 They first thought the movie would start at 8.30 p.m.
2 The movie starts half an hour earlier.
Answer: 8.00 p.m.



