


INTRODUCTION
Social Cognition in Clinical Neuropsychology: Value of a Model
Social cognition has recently received growing interest in clinical neuropsychology, given its reported impairments in a wide range of conditions from neurology to psychiatry and geriatrics (e.g., McDonald, Reference McDonald2013). It has been the topic of an increasing number of publications these past few years. Indeed, the number of published articles with the terms “social cognition” and “neuropsychology” in PsycINFO, Psycarticles and Psychology and Behavioral Sciences Collection databases has considerably increased from 1994 until today. Sixteen articles were published from 1994 to 1999, then 323 articles from 2000 to 2009, and finally 829 articles from 2010 to 2017.
The construct of social cognition originally emerged from social psychology. Initial research was performed in the 1940s with the experiment of Heider and Simmel (Reference Heider and Simmel1944). They reported that participants spontaneously interpreted movements of geometrical figures in terms of actions of persons, suggesting an automatic capacity to attribute mental states to others. This original research gave rise to various definitions of social cognition. One of the first was provided by Brothers (Reference Brothers1990) who stated that “social cognition is the processing of any information which culminates in the accurate perception of the dispositions and intentions of other individuals.”
Definitions were then further delineated around the notion of social information processing, from perception to processing of this specific information. One of most widely used is the definition of Adolphs (Reference Adolphs2009) for whom social cognition refers to the “psychological processes that allow us to make inferences about what is going on inside other people—their intentions, feelings, and thoughts.” These processes require several higher cognitive abilities, as social cognition is aimed at “constructing representations of the relations between oneself and others, and to use those representations flexibly to guide social behavior” (Adolphs, Reference Adolphs1999, Reference Adolphs2001).
Social cognition encompasses a wide range of components. Among these, theory of mind was the first and was originally studied in autism (Baron-Cohen, Leslie, & Frith, Reference Baron-Cohen, Leslie and Frith1985; Baron-Cohen, Reference Baron-Cohen2000). It refers to the ability to “impute mental states to oneself and others” (Premack & Woodruff, Reference Premack and Woodruff1978). This definition suggests that individuals should be aware of their own mental states (metacognition) and identify and understand mental states which can potentially contain emotions (emotional information processing). Since these first studies, other components have been included in studies of social cognition in neuropsychology (see Table 1 for the most frequently explored in the literature). It is worth noting that alexithymia has been included in the review just as other social cognition constructs. In the literature, alexithymia is recognized as a pathological state or as a continuous personality trait (Zackheim, Reference Zackheim2007), and both coexist without obvious controversy (Parker, Keefer, Taylor, & Bagby, Reference Parker, Keefer, Taylor and Bagby2008).
Table 1 The most frequent components of social cognition

In the present review, we consider alexithymia as a dimensional construct (i.e., a continuous personality trait), normally distributed in the general population (Bagby & Taylor, Reference Bagby and Taylor1997, Parker et al., Reference Parker, Keefer, Taylor and Bagby2008). Thus, alexithymia can be located along a continuum of severity, with a high degree of alexithymia corresponding to “one pole of the developmental continuum” of emotional awareness according to Lane and Schwartz (Reference Lane and Schwartz1987).
The constellation of social cognition abilities appears to be fundamental when considering individuals as social beings. Indeed, the success of humans in social interactions is one of the major abilities driving our evolution and adaptation (Humphrey, Reference Humphrey1976). While social cognition was first explored in psychiatric conditions, research has extended to neurology in the past two decades. Exponential research has also been undertaken in a wide range of disorders such as schizophrenia (Savla, Vella, Armstrong, Penn, & Twamley, Reference Savla, Vella, Armstrong, Penn and Twamley2013), autism (Baron-Cohen, Reference Baron-Cohen2000; Kanner, Reference Kanner1943; Travis & Sigman, Reference Travis and Sigman1998), bipolar disorder (Samamé, Reference Samamé2013), brain injury (McDonald, Reference McDonald2013; Spikman, Timmerman, Milders, Veenstra, & van der Naalt, Reference Spikman, Timmerman, Milders, Veenstra and van der Naalt2012), and neurodegenerative disorders (Elamin, Pender, Hardiman, & Abrahams, Reference Elamin, Pender, Hardiman and Abrahams2012; Snowden et al., Reference Snowden, Gibbons, Blackshaw, Doubleday, Thompson, Craufurd and Neary2003).
Numerous studies support the specificity of social cognition as a distinct area of cognitive functioning that is only partially dependent on neurocognition (Addington & Piskulic, Reference Addington and Piskulic2011; van Hooren et al., Reference van Hooren, Versmissen, Janssen, Myin-Germeys, à Campo, Mengelers and Krabbendam2008; Ventura, Wood, & Hellemann, Reference Ventura, Wood and Hellemann2013). For example, in schizophrenia, Fanning, Bell, and Fiszdon (Reference Fanning, Bell and Fiszdon2012) showed that 25% of their participants had intact neurocognition but impaired social cognition. Moreover, social cognition impairments may crucially impact daily life such as work, independent living or social functioning in schizophrenia (Brekke, Kay, Lee, & Green, Reference Brekke, Kay, Lee and Green2005). In traumatic brain injury, social cognition impairments are negatively associated with eventual outcome, lasting into the chronic stage post-injury (Spikman et al., Reference Spikman, Timmerman, Milders, Veenstra and van der Naalt2012).
However, to date, the data have remained hard to synthesize regarding social cognition functioning and dysfunctioning. The first main reason is theoretical discrepancies, as in the above-mentioned definitions. The second main reason, which is intrinsically related to the first, is the great heterogeneity in methodologies used in studies, which may provide inconsistent results (Corbera, Wexler, Ikezawa, & Bell, Reference Corbera, Wexler, Ikezawa and Bell2013; Mehta et al., Reference Mehta, Thirthalli, Subbakrishna, Gangadhar, Eack and Keshavan2013). These limitations have prevented researchers and clinicians from clearly understanding the nature and the severity of social cognition dysfunctioning, as well as its specificities in different conditions. In particular, these limitations stem from a current problem in studies of social cognition: the lack of a clear and comprehensive model encompassing the different dimensions and their relationships. Studying the factor structure of social cognition is a first step to better understand the architecture of the function (Child, Reference Child2006). Indeed, factor structure provides evidence regarding the scope and the number of social cognition dimensions, their independency and the relationships between them (Nunnally & Bernstein, Reference Nunnally and Bernstein1994).
AIM OF STUDY
The aim of this study is to systematically review studies that explored the factor structure of social cognition in adult general and clinical populations.
METHOD
This systematic review was based on the PRISMA statements (Moher et al., Reference Moher, Shamseer, Clarke, Ghersi, Liberati and Petticrew2015).
Literature Search
A systematic search was conducted in Pubmed, Scopus, Psycinfo, Psycarticles and Psychology and Behavioral Sciences Collection databases by AE in March 2017. Combinations of the following terms were searched: “factor structure” OR “principal component* analysis” OR “exploratory factor analysis” OR “confirmatory factor analysis” AND “social cognition”, from January 1982 to March 2017. Additionally, the reference lists of the retrieved articles were examined for cross-references.
Inclusion Criteria
By consensus between A.E. and A.P., studies were included if they met the following criteria: Sample size of more than 30 participants; Participants with an age ranging from 18 to 65 years; Social cognition assessed by neuropsychological tools; Assessment of at least two distinct components of social cognition; Factor analysis (principal component analysis, exploratory or confirmatory factor analyses) conducted on social cognition scores; Studies published in peer reviews.
The search was not limited in terms of study design, date, language, or pathological condition. After downloading article references, duplicates were excluded. All abstracts were read. If abstracts were insufficiently informative about eligibility criteria, the full texts were read.
RESULTS
Search Results
The initial search provided 441 articles. Only 11 fulfilled the above-mentioned selection criteria (see Figure 1). All were conducted in psychiatric populations and/or healthy participants. No study was conducted in populations suffering from acquired brain damage.

Fig. 1 PRISMA flow diagram of systematic literature search.
Results of Factor Structure Analyses
Two studies were conducted in healthy populations, three in schizophrenia spectrum disorders, five in both populations and one in three different populations (healthy population, schizophrenia spectrum disorders, and bipolar disorder). The reviewed studies reported from one- to four-factor structures of social cognition. Among the 11 reviewed studies (see Appendix for detailed description), most proposed a distinction in social cognition between low- and high-level information processing (four studies) or between affective and cognitive processing (also four studies). Nevertheless, three additional studies did not use these dichotomies.
Low-Level versus High-Level Processing
Four studies reported a distinction between low- and high-level information processing. The reported factor structure explained 52% to 74% of the social cognition.
Bliksted, Fagerlund, Weed, Frith, and Videbech (Reference Bliksted, Fagerlund, Weed, Frith and Videbech2014) assessed social cognition, neurocognition and symptomatology in 36 first-episode schizophrenia participants. The two first factors were interpreted as different levels regarding the complexity of information processing: Factor 1 was composed of tasks assessing complex social cognition, such as the understanding and the accuracy of theory of mind states. On the other hand, Factor 2 comprised tasks assessing the attribution of simple mental states and tasks assessing the ability to detect non-theory of mind animations. Factor 3 comprised tasks assessing the ability to discriminate between sarcasm and sincerity.
Buck, Healey, Gagen, Roberts, and Penn (Reference Buck, Healey, Gagen, Roberts and Penn2016) compared social cognition structure between participants with schizophrenia spectrum disorders (N=65) and controls (N=50). In the non-clinical sample, a three-factor solution emerged. Factor 1 was named “hostile attributional style.” Factor 2, labeled “higher level inferential and regulatory processes.” was composed of tasks assessing theory of mind and jumping to conclusions and Factor 3, named “lower-level social cue detection,” comprised tasks assessing the perception of emotion. Whereas Factor 1 was also found in schizophrenia spectrum disorders, Factors 2 and 3 were rather confounded in one undifferentiated factor named “social cognition skills.”
Mancuso, Horan, Kern, and Green (Reference Mancuso, Horan, Kern and Green2011) administered five tasks assessing social cognition to 85 participants with schizophrenia spectrum disorders. Apart from a first factor labeled “hostile attributional style,” the two remaining factors were interpreted as different levels regarding the complexity of information processing. Factor 2, named “lower-level social cue detection,” comprised tasks assessing facial emotion recognition, processing of non-verbal information transmitted by others, and detection of lies. Factor 3, called “higher-level inferential and regulatory processes”, comprised tasks targeting the ability to manage subjective emotional states and to detect sarcasm.
Thaler, Allen, Sutton, Vertinski, and Ringdahl (Reference Thaler, Allen, Sutton, Vertinski and Ringdahl2013) also reported this distinction using five social cognition tasks administered to 78 participants with bipolar disorder or with schizophrenia. Factor 1 (lower social cognitive factor), labeled “social/emotional processing,” comprised tasks of basic facial and social stimuli processing. Factor 2 (higher social cognitive factor), named “theory of mind,” comprised tasks requiring inference and expression of others’ ambiguous intentions.
Affective versus Cognitive Processing
Four studies highlighted a distinction between affective and cognitive information processing. The reported factor structure explained 56.5% to 75.7% of the social cognition.
Bell, Tsang, Greig, and Bryson (Reference Bell, Tsang, Greig and Bryson2009) administered four tasks assessing social cognition to 151 participants with schizophrenia spectrum disorders. Factor 1, labeled “theory of mind,” comprised tasks requiring the inferring of intentions to others and corresponded to the cognitive component of social cognition. Factor 2, named “affect recognition,” was composed of tasks assessing facial and prosodic emotion recognition and corresponded to the affective component of social cognition. According to the authors, both these factors corresponded to elemental features of social cognition. Factor 3, called “egocentricity,” represented the self-experience of relatedness, corresponding to a more autistic understanding of others (i.e., experiencing others as existing only to meet their needs and being unable to demonstrate empathy). Factor 4, labeled “rapport,” comprised the ability to establish rapport, as rated by interviewers. According to Bell et al. (Reference Bell, Tsang, Greig and Bryson2009), these two latter factors corresponded to holistic aspects of social cognition.
Etchepare et al. (Reference Etchepare, Merceron, Amieva, Cady, Roux and Prouteau2014) used seven tasks to assess social cognition abilities in 109 healthy participants. Factor 1, named “emotional information processing,” was composed of tasks assessing facial emotion recognition, theory of mind, alexithymia, and emotional awareness. Factor 2, labeled “cognitive theory of mind,” was constituted only by a task assessing the ability to attribute intentions without emotional information. Factor 3 comprised emotional fluency task scores and was named “emotional lexicon.” Finally, Factor 4 corresponded to facial emotional recognition and denomination scores and was labeled “facial emotion recognition.” Factors 1, 3, and 4 represented the affective component of social cognition, whereas Factor 2 reflected the cognitive aspect.
Mehta, Thirthalli, et al. (Reference Mehta, Bhagyavathi, Thirthalli, Kumar and Gangadhar2014) administered five social cognition tasks to 170 schizophrenia participants and 111 healthy participants. A three-factor solution was found in schizophrenia participants. Factor 1, labeled “socio-emotional processing,” comprised tasks assessing emotion recognition, social perception, and faux-pas recognition, corresponding to the affective side of social cognition. Factor 2, named “social–inferential ability,” combined theory of mind tasks and personalizing bias scores, corresponding to the cognitive side. Finally, Factor 3, constituted by externalizing bias scores, was called “external attribution bias.” Of interest, a similar structure was found in healthy participants. Factor 1 (“socio-emotional processing”) comprised the same tasks, except for the addition of the personalizing bias score. However, Factor 2, also labeled “social-inferential ability”, comprised only second-order theory of mind and externalizing bias.
Ziv, Leiser, & Levine (Reference Ziv, Leiser and Levine2011) administered four social cognition tasks to 75 healthy participants. Factor 1, labeled “cognitive theory of mind,” was composed of tasks assessing first- and second-order theory of mind and matrix reasoning, and corresponded to the cognitive aspect of social cognition. Factor 2, named “emotion recognition and processing,” grouped tasks assessing emotion processing and the understanding of irony and corresponded to the affective aspect of social cognition.
Other Factor Structures in Social Cognition
Three studies did not differentiate low- and high-level or affective and cognitive processing.
Browne et al. (Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016) administered five tasks assessing emotion processing and theory of mind to 179 participants with schizophrenia and 104 healthy participants. They reported that social cognition items loaded on a unitary factor for both groups.
Corbera et al. (Reference Corbera, Wexler, Ikezawa and Bell2013) administered five tasks measuring social cognition to 30 participants with schizophrenia spectrum disorders and 24 healthy participants. After combining their results, they reported that Factor 1, labeled “interpersonal discomfort,” comprised a measure of personal distress and an egocentric self-protective view of relatedness. Factor 2, named “basic social cognition,” included the ability to identify facial and vocal emotions as well as theory of mind. Finally, Factor 3, called “empathy,” comprised different empathic abilities like empathic concern, perspective-taking and fantasy.
Stouten, Veling, Laan, van der Helm, and van der Gaag (Reference Stouten, Veling, Laan, van der Helm and van der Gaag2015) reported a four-factor structure after administering four tasks about social cognition to 162 participants with first-episode psychosis. Factor 1, named “social cognitive biases,” comprised tests assessing various cognitive biases (like safety, subjective cognitive problems, belief inflexibility bias, social cognitive problems, and attention for threats). Factor 2, called “emotion processing speed,” was composed of reaction times obtained in recognizing facial emotion tasks. Factor 3, labeled “general social cognition,” comprised tasks assessing theory of mind, recognition of facial emotions and social knowledge. Finally, Factor 4, named “attribution and inference bias,” was composed of tests assessing jumping to conclusions and external attributional bias.
DISCUSSION
The aim of this study was to systematically review studies of factor structure of social cognition in general and clinical populations, both psychiatric and neurologic. A total of 11 studies were included in this review. The numbers of observed factors reported in the social cognition structure varied from one to four, explaining 52% to 75.7% of the social cognition. In the human sciences, where data are always less precise than in the natural sciences, a solution explaining 60% of the total variance is considered as satisfactory (Hair, Reference Hair2006), which is the case with many of the studies reviewed.
These findings support the study by Mehta et al. (Reference Mehta, Thirthalli, Subbakrishna, Gangadhar, Eack and Keshavan2013) that did not find any robust factor structure in schizophrenia spectrum disorders. However, that review was limited to one condition and included studies which sometimes measured only one component of social cognition. Our review is an up-to-date and extensive overview of the literature regarding the factor structure of social cognition. We included studies conducted in general and/or in clinical populations that investigated at least two components of social cognition.
Low-Level versus High-Level Processing
Four studies were in favor of a distinction between low-level and high-level processing in social cognition. Three of them (Buck et al., Reference Buck, Healey, Gagen, Roberts and Penn2016; Mancuso et al., Reference Mancuso, Horan, Kern and Green2011; Thaler et al., Reference Thaler, Allen, Sutton, Vertinski and Ringdahl2013) reported a similar structure: (i) a low-level factor composed of tasks assessing emotion recognition through facial expressions, vocal intonations or gestures as well as lie recognition. These tasks require answering basic social stimuli or low-level mental representations; (ii) a high-level factor composed of tasks assessing jumping to conclusions, the ability to solve interpersonal problems, to manage emotions as well as theory of mind skills, especially the ability to detect sarcasm and infer an intention. These tasks require inferring complex mental states, taking another perspective or managing subjective emotional states.
In the fourth study, Bliksted et al. (Reference Bliksted, Fagerlund, Weed, Frith and Videbech2014) did not include facial or prosodic emotion recognition tasks but provided evidence for a low versus high process distinction within theory of mind. Indeed, the ability to infer simple mental states is considered as low-level processing. High-level processing is reflected by tasks requiring understanding and accurately describing more complex mental states. The authors established links with the model of Apperly and Butterfill (Reference Apperly and Butterfill2009).
As previously highlighted by Mancuso et al. (Reference Mancuso, Horan, Kern and Green2011), this distinction between low- and high-level processing has also been hypothesized in the social neurosciences. Indeed, on the basis of knowledge about brain structure functioning, Ochsner (Reference Ochsner2008) differentiated a low-level construct, characterized by embodied simulation supported by mirror neurons, and a high-level construct, including integration of context such as in the understanding of false beliefs. Nevertheless, the role of mirror neurons in the low-level construct remains controversial. For example, in their meta-analysis, Van Overwalle and Baetens (Reference van Overwalle and Baetens2009) reported that mirror neurons are not systematically activated in tasks assessing theory of mind.
The literature provides a strong conceptual framework for this dichotomy. Several authors (Adolphs, Reference Adolphs2009, Reference Adolphs2010; Frith & Frith, Reference Frith and Frith2008) differentiate a low-level processing in social cognition that is implicit, fast, automatic, unconscious from a high-level processing, which is explicit, slow, flexible, effortful, and conscious. This corresponds to classic dual-process theories (for a recent review, see Happé, Cook, & Bird, Reference Happé, Cook and Bird2017), also known in the literature as “system 1 and system 2” (Evans, Reference Evans2008), “reflexive and reflective processing” (Lieberman, Reference Lieberman2007), “implicit and explicit processing” (Frith & Frith, Reference Frith and Frith2008), or “controlled and automatic processing” (Schneider & Shiffrin, Reference Schneider and Shiffrin1977).
The dual process system is supported by several types of evidence. Developmental research provides strong evidence for the hierarchical development of low and high processes. First, children begin to understand desires, intentions and false beliefs (Bartsch & Wellman, Reference Bartsch and Wellman1989). In middle childhood, they first acquire the ability to interpret white lies correctly, then ironic criticism, deceptive intent and finally sarcasm (Demorest, Meyer, Phelps, Gardner, & Winner, Reference Demorest, Meyer, Phelps, Gardner and Winner1984). Onishi (Reference Onishi2005) demonstrated that 18-month-old children are able to succeed in implicit false-belief tasks but not in explicit false-belief tasks until the age of 4 years.
According to Apperly and Butterfill (Reference Apperly and Butterfill2009), high-level processing requires heavy cognitive resources like language and executive functions which are acquired later, and is partially underwritten by low-level processing. Both clinical research and neuroimaging studies provide evidence for the partial separability of low- and high-level processes. For example, adults with Asperger syndrome can successfully perform explicit theory of mind tasks but fail to attribute mental states (implicit processing) spontaneously (Senju, Southgate, White, & Frith, Reference Senju, Southgate, White and Frith2009). Moreover, various patterns of activation have been reported for explicit and implicit theory of mind tasks (for a meta-analysis, see Molenberghs, Johnson, Henry, & Mattingley, Reference Molenberghs, Johnson, Henry and Mattingley2016). However, the results of this meta-analysis also suggest some common networks between these processes. Indeed, some authors are in favor of a hierarchy between low and high processing (Apperly & Butterfill, Reference Apperly and Butterfill2009; Mancuso et al., Reference Mancuso, Horan, Kern and Green2011; Onishi, Reference Onishi2005), others not (Senju et al., Reference Senju, Southgate, White and Frith2009).
Affective versus Cognitive Processing
Four studies are in favor of a distinction between the affective and cognitive components in social cognition (Bell et al., Reference Bell, Tsang, Greig and Bryson2009; Etchepare et al., Reference Etchepare, Merceron, Amieva, Cady, Roux and Prouteau2014; Mehta, Thirthalli, et al., Reference Mehta, Bhagyavathi, Thirthalli, Kumar and Gangadhar2014; Ziv et al., Reference Ziv, Leiser and Levine2011). On the one hand, the affective factor is composed of tasks requiring “emotion-driven” processes, participants having to process emotional information. On the other, the cognitive factor is always composed of at least one cognitive theory of mind task, requiring participants to infer intention or understand mental states. In cognitive theory of mind tasks, no emotional information processing is required.
This distinction is reminiscent of Adolphs (Reference Adolphs2010) model, adapted by McDonald (Reference McDonald2013). Both are theoretical models that still lack empirical evidence. In the second of the three components of this model, named “evaluation and interpretation”, the authors distinguish “hot” and “cold” social cognition. Hot social cognition refers to emotion processing, whereas cold social cognition corresponds to the ability of thinking about things from another’s point of view, including theory of mind. Hot versus cold social cognition is equivalent to affective versus cognitive components of social cognition.
Similarly, other authors have differentiated the affective and cognitive components in studies on theory of mind and on empathy. In clinical research, brain impairment studies provide strong evidence for a dissociation between affective and cognitive impairments in the two components (Shamay-Tsoory, Reference Shamay-Tsoory2015; Shamay-Tsoory & Aharon-Peretz, Reference Shamay-Tsoory and Aharon-Peretz2007; Shamay-Tsoory, Tibi-Elhanany, & Aharon-Peretz, Reference Shamay-Tsoory, Tibi-Elhanany and Aharon-Peretz2006). These dissociations are also described in autism spectrum disorder (impaired cognitive but preserved affective empathy) and psychopathy (impaired affective but preserved cognitive empathy) (Blair, Reference Blair2005; Jones, Happé, Gilbert, Burnett, & Viding, Reference Jones, Happé, Gilbert, Burnett and Viding2010; Shamay-Tsoory, Harari, Aharon-Peretz, & Levkovitz, Reference Shamay-Tsoory, Harari, Aharon-Peretz and Levkovitz2010). Neuroimaging research provides strong evidence that dissociated networks support affective and cognitive theory of mind (for a recent review, see Abu-Akel & Shamay-Tsoory, Reference Abu-Akel and Shamay-Tsoory2011), or affective and cognitive empathy (Dvash & Shamay-Tsoory, Reference Dvash and Shamay-Tsoory2014; Fan, Duncan, de Greck, & Northoff, Reference Fan, Duncan, de Greck and Northoff2011; Shamay-Tsoory, Aharon-Peretz, & Perry, Reference Shamay-Tsoory, Aharon-Peretz and Perry2009).
Of the 11 studies included in the present review, it should be underscored that three reported inconsistent results regarding the above-mentioned distinctions (low- vs. high-level processing and affective vs. cognitive processing). Indeed, Browne et al. (Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016), Corbera et al. (Reference Corbera, Wexler, Ikezawa and Bell2013) and Stouten et al. (Reference Stouten, Veling, Laan, van der Helm and van der Gaag2015) reported no distinction between theory of mind and emotion perception, tasks loading on the same factor. Regarding Browne et al. (Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016), this discrepancy in results may be explained by the statistical analyses that the authors used. Indeed, the study by Browne et al. (Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016) was the only one to use a confirmatory factor analysis, in the assumption that measures assessing theory of mind and emotion perception would load on a unidimensional model.
Attributional Style
When included in studies, attributional style is regularly reported to be an isolated factor in social cognition (Buck et al., Reference Buck, Healey, Gagen, Roberts and Penn2016; Mancuso et al., Reference Mancuso, Horan, Kern and Green2011; Mehta, Thirthalli, et al., Reference Mehta, Thirthalli, Bhagyavathi, Keshav Kumar, Subbakrishna, Gangadhar and Keshavan2014; Stouten et al., Reference Stouten, Veling, Laan, van der Helm and van der Gaag2015). This result raises questions about the links between attributional style and other social cognition dimensions. Conceptually, attributional style describes a cognitive style related to personality, rather than a type of performance (Buck et al., Reference Buck, Healey, Gagen, Roberts and Penn2016; Healey, Bartholomeusz, & Penn, Reference Healey, Bartholomeusz and Penn2016). However, some models, such as the one suggested by the Social Cognition Psychometric Evaluation (SCOPE) study (Green et al., Reference Green, Penn, Bentall, Carpenter, Gaebel, Gur and Heinssen2008; Green, Olivier, Crawley, Penn, & Silverstein, Reference Green, Olivier, Crawley, Penn and Silverstein2005; Pinkham et al., Reference Pinkham, Penn, Green, Buck, Healey and Harvey2014), include attributional style in social cognition without explaining how it is related to other dimensions. The SCOPE model is a list of potentially relevant social cognition dimensions based on expert surveys. Nevertheless, consensus among recognized experts is considered as the least compelling level of evidence with regard to interventional research (American Psychological Association, 2006). Further research is thus needed to better understand attributional style as a component of social cognition in neuropsychological assessment, and how it is related to other dimensions.
Crossing Perspectives: Proposition of a Global Model of Social Cognition in Neuropsychology
The above-mentioned models of social cognition (e.g., low- vs. high-level, affective vs. cognitive social cognition) have received strong support from lesion studies, neuroimaging, developmental and clinical research. Some recent studies have tried to bridge the gap between them by partially merging low-level and high-level processing with affective and cognitive processing. For example, following their factor analysis, Mehta, Thirthalli, et al. (Reference Mehta, Bhagyavathi, Thirthalli, Kumar and Gangadhar2014) hypothesized that their cognitive factor of social cognition (i.e., “social–inferential ability”) could be divided into two components: a low-level (understanding goals of actions) and high-level (processing more complex judgements of others) mental state inference. Thaler et al. (Reference Thaler, Allen, Sutton, Vertinski and Ringdahl2013) also claim that their two social cognition factors (i.e., “social/emotional processing” and “theory of mind”) both support the low- versus high-level distinction of Mancuso et al. (Reference Mancuso, Horan, Kern and Green2011) and the affective versus cognitive distinction of Ziv et al. (Reference Ziv, Leiser and Levine2011).
Our review provides further support for the relevance of crossing perspectives. Indeed, in most of the studies reviewed, factor analyses consistently differentiated emotional perception (e.g., through prosody, facial emotions) and cognitive theory of mind (Bell et al., Reference Bell, Tsang, Greig and Bryson2009; Browne et al., Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016; Etchepare et al., Reference Etchepare, Merceron, Amieva, Cady, Roux and Prouteau2014; Thaler et al., Reference Thaler, Allen, Sutton, Vertinski and Ringdahl2013; Ziv et al., Reference Ziv, Leiser and Levine2011). This difference could be understood as a distinction between affective and cognitive processing, but also as a distinction between low- and high-level processing.
Thus, among the social cognition tests used in clinical neuropsychology, two dimensions can be distinguished: (i) the nature of processed information: affective processing, which is mainly characterized by the processing of emotional information, and cognitive processing, which requires subjects to process information like intentions, beliefs, and/or knowledge, in which emotion is absent or secondary; (ii) the level of processed information: low-level processing, which is characterized by automatic, implicit processing, and high-level processing, which encompasses more complex cognitive processes (e.g., executive functioning), thus corresponding to more controlled, explicit and effortful processing.
Figure 2 synthesizes these assumptions in a two-dimensional model of social cognition for clinical neuropsychology, with examples of corresponding domains of assessment. For each domain, tasks are proposed. They were chosen according to the following criteria: (1) tasks were included in reviewed studies; (2) tasks are commonly used in clinical practice. In addition, we have added the Situational Features Recognition Test (SFRT) to exemplify social knowledge and the Theory Of Mind-15 (TOM-15), a task simultaneously providing assessment of first- and second-order false beliefs. These tasks were not used in the reviewed studies but are usually cited in the literature. Though based on the review results, the model needs further validation to ensure that the tasks actually correspond to these particular domains.
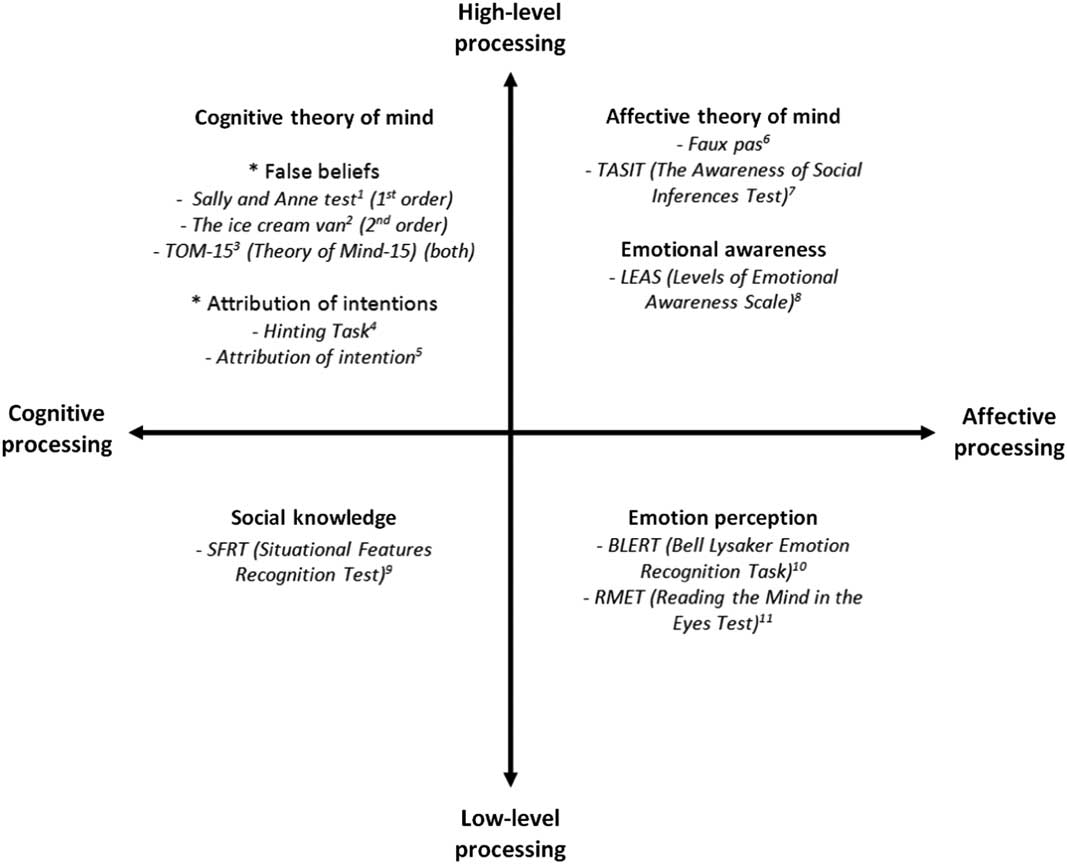
Fig. 2 A two-dimensional model of social cognition.Note.1 Baron-Cohen et al. (Reference Baron-Cohen, Leslie and Frith1985); Wimmer & Perner (Reference Wimmer and Perner1983). 2 Perner & Wimmer (Reference Perner and Wimmer1985). 3 Desgranges et al. (Reference Desgranges2012). 4 Corcoran, Mercer, & Frith (Reference Corcoran, Mercer and Frith1995). 5 Brunet, Sarfati, & Hardy-Baylé (Reference Brunet, Sarfati and Hardy-Baylé2003); Sarfati, Hardy-Baylé, Besche, & Widlöcher (Reference Sarfati, Hardy-Baylé, Besche and Widlöcher1997). 6 Baron-Cohen, O’Riordan, Stone, Jones, & Plaisted (Reference Baron-Cohen, O’Riordan, Stone, Jones and Plaisted1999); Stone, Baron-Cohen, & Knight (Reference Stone, Baron-Cohen and Knight1988). 7 McDonald, Flanagan, Rollins, & Kinch (Reference McDonald, Flanagan, Rollins and Kinch2003). 8 Lane, Quinlan, Schwartz, Walker, & Zeitlin (Reference Lane, Quinlan, Schwartz, Walker and Zeitlin1990). 9 Corrigan & Green (Reference Corrigan and Green1993). 10 Bell, Bryson, & Lysaker (Reference Bell, Bryson and Lysaker1997). 11 Baron-Cohen, Wheelwright, Hill, Raste, & Plumb (Reference Baron-Cohen, Wheelwright, Hill, Raste and Plumb2001).
Implications for the Assessment of Social Cognition in Clinical Neuropsychology
Our results also provide new insights into the assessment and interventions that target social cognition, which is a topic of great interest in neuropsychology (Kelly, McDonald, & Frith, Reference Kelly, McDonald and Frith2017). Given the structure of social cognition, clinical assessment should ideally cover the two dimensions of the above-described model. In a treatment perspective, it is indeed crucial to distinguish between impairment tendencies in low-level or high-level processing and affective or cognitive processing. According to clinical neuropsychology guidelines, results should be crossed and performances compared to define and isolate difficulties in specific social cognitive domains (Brown, Del Dotto, Fisk, Taylor, & Breslau, Reference Brown, Del Dotto, Fisk, Taylor and Breslau1993; Lezak, Reference Lezak2004; Seron & Van der Linden, Reference Seron and Van der Linden2000).
Similarly, performances in social cognition also need to be crossed with other domains of cognitive performance. There is indeed strong evidence that neurocognition and social cognition are both related and separate constructs (Addington & Piskulic, Reference Addington and Piskulic2013; van Hooren et al., Reference van Hooren, Versmissen, Janssen, Myin-Germeys, à Campo, Mengelers and Krabbendam2008; Ventura et al., Reference Ventura, Wood and Hellemann2013). For example, Mehta, Bhagyavathi, Thirthalli, Kumar, and Gangadhar (Reference Mehta, Bhagyavathi, Thirthalli, Kumar and Gangadhar2014) reported that cognitive flexibility, as well as verbal and visual memories, predicted faux-pas recognition in a schizophrenia sample. This point has major implications for the methodology of social cognition assessment. First, neurocognitive deficits should be identified before assessment of social cognition. If severe neurocognitive impairments are identified, social cognition assessment should be adapted by proposing tasks with less cognitive load. If more discrete neurocognitive dysfunctions are identified, then caution is required when making conclusions about the assessment of social cognition. In any case, assessing neurocognition before social cognition avoids confounding social cognition difficulties with more basic neurocognitive ones.
In the same therapeutic perspective, the assessment of social cognition can be advantageously complemented by a self-rated questionnaire like the OSCARS (Observable Social Cognition: A Rating Scale) (Healey et al., Reference Healey, Combs, Gibson, Keefe, Roberts and Penn2015). Few tools have received satisfactory validation to date. Self-questionnaires allow subjective perception about one’s social cognitive abilities to be measured and may go beyond the lack of sensitivity of objective testing when exploring potential targets for cognitive intervention.
Limitations and Perspectives
The first limitation of this study is the heterogeneity in the factor analyses in the studies reviewed, which limits their comparability. Indeed, of the 11 studies included, three different factor analyses (principal components analysis, exploratory or confirmatory factor analysis), two various extraction methods (maximum likelihood, principal axis factor), and four different rotation methods (quartimax, oblique, promax, varimax) were used. Moreover, several studies did not report the extraction and/or rotation method used, even though discrepancies in extraction or rotation methods can lead to discrepancies in results (Tabachnick & Fidell, Reference Tabachnick and Fidell2013).
The present review is also indirectly limited by several characteristics of the literature targeted, in which the results obtained should be considered with caution. First, heterogeneity in tasks used and constructs assessed limits the comparability of the results. Second, social cognition is often measured by tasks that have inadequate or unknown psychometric properties. In particular, studies investigating the validity of these tools in the general population remain rare. Further research is necessary to provide adapted norms and evidence-based interpretation of the difficulties encountered. Some tasks were included more often than others, such as the Reading the Mind in the Eyes Test (RMET)/Eyes Test (Browne et al., Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016; Etchepare et al., Reference Etchepare, Merceron, Amieva, Cady, Roux and Prouteau2014; Thaler et al., Reference Thaler, Allen, Sutton, Vertinski and Ringdahl2013) or the Bell Lysaker Emotion Recognition Test (BLERT) (Bell et al., Reference Bell, Tsang, Greig and Bryson2009; Browne et al., Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016; Corbera et al., Reference Corbera, Wexler, Ikezawa and Bell2013; Thaler et al., Reference Thaler, Allen, Sutton, Vertinski and Ringdahl2013) for assessing emotion perception, and The Awareness of Social Inferences Test (TASIT) (Bliksted et al., Reference Bliksted, Fagerlund, Weed, Frith and Videbech2014; Browne et al., Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016; Buck et al., Reference Buck, Healey, Gagen, Roberts and Penn2016; Mancuso et al., Reference Mancuso, Horan, Kern and Green2011) or the Hinting Task (Bell et al., Reference Bell, Tsang, Greig and Bryson2009; Bliksted et al., Reference Bliksted, Fagerlund, Weed, Frith and Videbech2014; Browne et al., Reference Browne, Penn, Raykov, Pinkham, Kelsven, Buck and Harvey2016; Buck et al., Reference Buck, Healey, Gagen, Roberts and Penn2016; Corbera et al., Reference Corbera, Wexler, Ikezawa and Bell2013; Stouten et al., Reference Stouten, Veling, Laan, van der Helm and van der Gaag2015; Thaler et al., Reference Thaler, Allen, Sutton, Vertinski and Ringdahl2013) for assessing theory of mind.
Recently, Pinkham, Penn, Green, and Harvey (Reference Pinkham, Penn, Green and Harvey2016) and Ludwig, Pinkham, Harvey, Kelsven, and Penn (Reference Ludwig, Pinkham, Harvey, Kelsven and Penn2017) investigated several psychometric properties of eight social cognition tasks in 179 and 38 schizophrenia participants and 104 and 39 control participants, respectively. Currently, only the Hinting Task has displayed satisfactory psychometric properties so the validity of these tasks should be further investigated. A third limitation stems from small sample sizes, thereby limiting the generalizability of the results obtained and generating confounding effects of sociodemographic variables. As Bakker, Hartgerink, Wicherts, & van der Maas (Reference Bakker, Hartgerink, Wicherts and van der Maas2016) recently recalled, a formal power analysis should be more systematically performed before planning any study to enhance the robustness of results. Moreover, the heterogeneity of study samples suffering from different conditions (i.e., bipolar disorder, schizophrenia spectrum disorders, first-episode vs. chronic psychosis) could lead to discrepancies in results. Such discrepancies could reflect pathological processes rather than the structure of social cognition.
Similarly, several assumptions can be made about differences in the structure of social cognition between clinical populations and healthy controls. In our review, two studies highlighted a difference between a clinical population (schizophrenia) and healthy controls. The factor analysis of Buck et al. (Reference Buck, Healey, Gagen, Roberts and Penn2016) distinguished low-level and high-level processing in the healthy control group contrary to the schizophrenia group where these two factors loaded on the same one. According to these authors, social cognition abilities were more differentiated in healthy controls, schizophrenia participants suffering from a general performance deficit.
On the contrary, Mehta, Thirthalli, et al. (Reference Mehta, Bhagyavathi, Thirthalli, Kumar and Gangadhar2014) found a different factor structure in their study: three factors for the schizophrenia group and two for healthy controls. Indeed, the component “externalizing bias” loaded as a distinct factor in the schizophrenia group. According to these authors, social cognition abilities in schizophrenia and in healthy controls share more similarities than differences. Further research on this issue is, therefore, required. Finally, most of the studies reviewed were conducted in schizophrenia spectrum disorders. Further research remains necessary before extending the conclusions to other clinical populations.
CONCLUSION
Most studies that have explored the factor structure of social cognition provide support for two theoretical models: one distinguishing two levels of information processing (i.e., low- vs. high-level), and the other two types of processed information (i.e., affective vs. cognitive information). Moreover, these models are supported by several theoretical considerations and empirical evidence (i.e., developmental, clinical, and neuroimaging studies). Recently, some studies started to create links between these two models. We hypothesize that both models can be integrated in a two-dimensional model of social cognition, crossing low- and high-level processing with affective and cognitive processing. By specifying the architecture of social cognition, this model makes it possible to classify the available measurements more precisely and to organize assessment in clinical practice.
This review constitutes a first step to a better grasp of the nature and the constitution of social cognition in clinical neuropsychology. Given that social cognition impairments are transdiagnostic, further research will provide crucial information for assessing the accuracy and relevance of therapeutic interventions.
ACKNOWLEDGMENTS
The authors thank Dr. Ray Cooke for copy editing. The authors declare no conflict of interest.
APPENDIX: FACTOR STRUCTURE OF SOCIAL COGNITION




