Case report
Coronary artery anomalies are rare but recognised causes of sudden death. Isolated coronary ostial atresia, seen in left coronary artery atresia, is absence of the left coronary ostium and main trunk with the left anterior descending and circumflex arteries normally connecting and obtaining blood supply from the right coronary artery via collaterals.Reference Musiani, Cernigliaro, Sansa and DeGasperis1 Single coronary artery describes a coronary ostium giving rise to both main coronary arteries. Left coronary artery atresia differs from a single coronary artery as blood flows from the right to the left coronary via collateral vessels whose calibre is smaller than the target left-sided vessel. This collateral circulation is often inadequate to meet cardiac metabolic needs, and those affected exhibit differing age-related symptomatology. Neonates typically present with failure-to-thrive and myocardial infarction, whereas older children present with syncope.Reference Musiani, Cernigliaro, Sansa and DeGasperis1 Patients may have signs of left ventricular dysfunction and subendocardial ischemia on electrocardiogram.Reference Gebauer, Cerny, Vojtovic and Tax2 Diagnosis is usually delayed because findings are non-specific. Some are asymptomatic when extensive collateral circulation is present, and these patients require surgical revascularisation to prevent coronary ischemia.Reference Musiani, Cernigliaro, Sansa and DeGasperis1, Reference Gebauer, Cerny, Vojtovic and Tax2 Coronary ostial atresia is well described in pulmonary atresia/intact ventricular septum and coronary-cameral fistulae from the right ventricle, where one or both coronary arteries are supplied exclusively through fistulae. We report absence of both coronary artery ostia in a single/common coronary system not associated with pulmonary atresia, discussing potential embryologic basis and importance of early identification and intervention. A similar anomaly has been previously described in one other case report to date.Reference Olawale, Kearney and Krishnamurth3
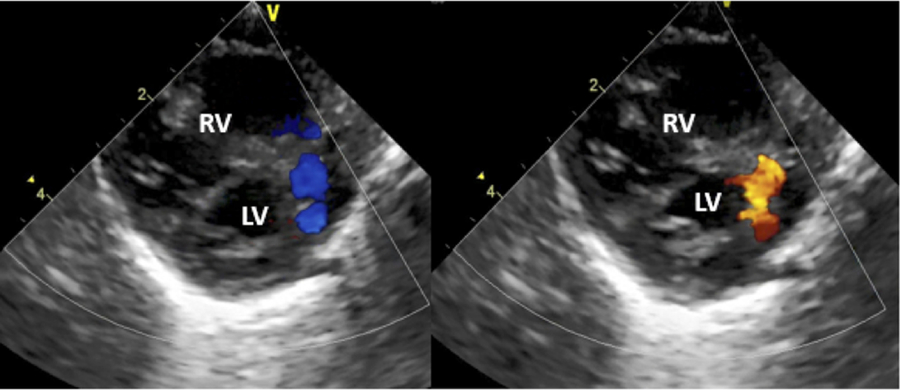
A 1-day-old 3.3-kg term neonate with prenatal cardiac diagnosis suspicious for a ventricular septal defect is delivered via emergent caesarean section secondary to nuchal cord presentation. APGAR scores were 8/9; however, the patient developed respiratory distress requiring oxygen. Laboratory results were normal. Physical examination and chest radiograph were consistent with transient tachypnea of the newborn. Antibiotics were started for presumed sepsis. Postnatal echocardiogram revealed a large patent ductus arteriosus with bidirectional shunting, patent foramen ovale with left-to-right shunting, and normal systolic function. Echocardiogram at 29 hours of life revealed new, moderate left ventricular dysfunction. Coronary arteries were not well visualised. A vascular structure with to-and-fro flow (Fig 1) suggestive of a coronary artery fistula was seen. ST segment depression in the anterior precordial leads was noted by electrocardiogram. Troponin was slightly elevated (0.16 ng/ml); BNP was significantly elevated (23,657 pg/ml). The patient was started on dopamine and milrinone and transported to the neonatal intensive care unit.

Figure 1. Vascular structure with to-and-fro flow into the RV that was thought possibly to be a coronary artery fistula.
Following transport, the patient suffered a cardiac arrest during vascular catheter placement. He was intubated and cardiopulmonary resuscitation initiated. Profuse blood was noted from the endotracheal tube and despite maximal resuscitative efforts, the patient remained bradycardic, hypotensive, and acidotic. Cardiology and cardiovascular surgery were consulted; extracorporeal membrane oxygenation support was considered futile in the setting of diffuse pulmonary haemorrhage. The patient expired at 36 hours of life.
Post-mortem findings
The external surface of the heart (Fig 2a) illustrated a smooth epicardium, and the major coronary arteries appeared to have a normal pattern with a left anterior descending artery meeting the posterior descending to the right of the cardiac apex. There was a prominent branch of the right coronary artery appearing to emanate from the right ventricular apex. Another prominent coronary was a pre-ventricular branch near the right atrial appendage. Internally, the right and left heart appeared normal. Neither the aorta nor the pulmonary artery showed evidence of coronary ostia. The pulmonary valve was of normal morphology. There was a single/common coronary artery coursing between the aorta and main pulmonary artery without evident origin (Fig 2b). The branching pattern and distribution appeared otherwise normal, and the central coronaries unusually thick, a similar finding to the previous case described in the literature.Reference Olawale, Kearney and Krishnamurth3 There was no obvious origin of coronary-cameral fistulae from either ventricle. Intracardiac evaluation was notable for a patent foramen ovale and ductus arteriosus.

Figure 2. Exterior, anterior view. Ao = ascending aorta, LAA = left atrial appendage, PA = main pulmonary artery, RAA = right atrial appendage, white arrows = right coronary artery, black arrows = left coronary artery, black arrowheads = dilated fistulous coronary artery, dotted line = plane of transaction of ascending aorta in subsequent figure.

Figure 3. Exterior, right anterior oblique cranially angulated view. Transected ascending aorta (Ao [black label proximal, white label distal]) is reflected anteriorly revealing single/common coronary artery passing between Ao and main pulmonary artery (PA). White arrows indicate right coronary portion; black arrows indicate left coronary portion. Dao = descending aorta, LA = left atrium, PDA = patent ductus arteriosus, RA = right atrium, orientation arrow: A = anterior, L = left, P = posterior, R = right.
Discussion
Coronary anomalies occur in 0.2–1.2% of patients with congenital heart disease, with coronary ostial atresia the rarest.Reference Bogers, Gittenberger-de Groot, Poelmann, Péault and Huysmans4 Non-patency of the left coronary ostium with or without atresia of the left main coronary artery has been previously described. This case is reminiscent of coronary ostial atresia in pulmonary atresia/intact ventricular septum with significant right ventricular coronary-cameral fistulae or so-called right ventricular-dependent coronary circulation, where some or all coronary perfusion arises from right ventricular fistulae. In pulmonary atresia/intact ventricular septum with right ventricular-dependent coronary circulation, elevated right ventricular pressure is essential for effective coronary perfusion.Reference Guleserian, Armsby and Thiagarajan5 We speculate that coronary perfusion was dependent on elevated right ventricular pressure and decreased pulmonary vascular resistance led to decreased pressure with resultant malperfusion and fatal ischemia. If this coronary anomaly were detected in utero, immediate post-natal intervention may have been possible.
Coronary ostial atresia may be congenital or acquired. It is unclear if this patient’s anomalies were related to a genetic condition as no genetic testing was completed. Thickening of central coronary arteries raises the possibility of Williams syndrome, known to be associated with coronary ostial stenosis. In two cases, left coronary artery atresia has been reported with supravalvar aortic stenosis.Reference Rosenkranz, Murphy and Cosgrove6 Coronary ostial atresia should not imply obliteration of previously patent connections. Evidence in avianReference Bogers, Gittenberger-de Groot, Poelmann, Péault and Huysmans4 and humanReference Tomanek7 embryos support that coronary ostia result from penetration of the aortic wall by coronary vasculature surrounding the aorta and pulmonary artery between 6 and 7 weeks gestation. Failure of coronary-aortic penetration may result in coronary ostial atresia, with a likely multi-factorial cause. Gittenberger-de-Groot et al in studying epicardial outgrowth inhibition in avian embryos, reported a case where “the connection of both main coronaries to the aorta was missing and replaced by two ventriculo-coronary communications (fistulae).”Reference Eralp, Lie-Venema and DeRuiter8 They postulate that fistulae supplying the coronaries may precede development of pulmonary atresia rather than being a result of high right ventricular pressure.Reference Gittenberger-de Groot, Sauer and Bindl9
This is a rare case describing coronary ostial atresia in a single/common coronary system with coronary-cameral fistulae. Visualisation of coronary ostia by fetal echocardiogram is challenging; however, a high index of suspicion pre- or immediately post-natally may allow for delivery at a tertiary care centre where early – preferably elective – mechanical circulatory support as a bridge to transplantation can be offered.
Acknowledgements
We thank N. Sasaki, M. Patel, and C. Zeidenweber for their thoughtful comments on this manuscript.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.