


Infants with CHD requiring early open-heart surgery are at an increased risk of adverse neurodevelopmental outcomes, including physical, behavioural, and cognitive impairments.Reference Snookes, Gunn and Eldridge 1 , Reference Marino, Lipkin and Newburger 2 Improvements in surgical and post-operative management have reduced mortality; however, increased morbidity has led to greater focus on neurodevelopmental outcomes, risk mitigation, and long-term follow-up.Reference Marino, Lipkin and Newburger 2 The American Heart Association and the American Academy of Pediatrics released guidelines in 2012, advocating for long-term surveillance, developmental screening, evaluation, and management of all infants with CHD who undergo open-heart surgery in the first year of life.Reference Marino, Lipkin and Newburger 2 Access to developmental follow-up services has historically been limited to those at highest risk based on the severity of diagnosis and complexity of surgical intervention.Reference Brosig, Butcher and Butler 3 The diagnostic-based inclusion criteria limit access to surveillance for infants who may have functional impairments associated with peri-operative clinical and environmental risk factors. There is a lack of longitudinal studies of all CHD infants after early open-heart surgery to assist with risk stratification and prioritisation in healthcare systems with finite resources.Reference Chorna, Baldwin and Neumaier 4 , Reference Uzark, Smith, Donohue, Yu and Romano 5
It is well established that certain peri-operative clinical management strategies, such as deep hypothermic arrest, have historically contributed to neurological impairment.Reference Li, Yin and Fang 6 , Reference Morton, Ishibashi and Jonas 7 Despite technological advances and a decline in mortality rates, adverse long-term neurodevelopmental outcomes of children with CHD undergoing open-heart surgery remain a significant burden.Reference Hovels-Gurich 8 There is increasing evidence that neurological changes including brain dysmaturation,Reference Claessens, Kelly, Counsell and Benders 9 reduced perfusion,Reference Lim, Kingdom and Saini 10 – Reference Nagaraj, Evangelou and Donofrio 12 and decreased brain volumeReference Von Rhein, Buchmann and Hagmann 13 may be present at birth in up to 50% of infants with complex CHD,Reference Khalil, Suff, Thilaganathan, Hurrell, Cooper and Carvalho 14 leading to neurobehavioural impairments such as feeding difficulties, poor state regulation, hypotonia, hypertonia, jitteriness, restlessness, and agitation requiring modified care practices.Reference Khalil, Suff, Thilaganathan, Hurrell, Cooper and Carvalho 14 – Reference Limperopoulos, Majnemer, Shevell, Rosenblatt, Rohlicek and Tchervenkov 16 Furthermore, inherent patient factors such as type of CHDReference Faraoni, Vo, Nasr and Dinardo 17 and post-operative factors such as length of hospital stayReference Gunn, Beca and Hunt 18 have been reported to contribute to poor long-term neurodevelopmental outcomes.
Identifying such risk factors can assist with predicting likelihood and severity of long-term neurodevelopmental morbidity, as well as offering opportunity for early intervention.Reference Calderon, Stopp and Wypij 19 , Reference Gaynor, Stopp and Wypij 20 Longitudinal studies have historically assessed infants post-operatively along the developmental trajectory.Reference Sananes, Manlhiot and Kelly 21 – Reference Bellinger, Watson and Rivkin 24 Focus is shifting to include evaluation of neurodevelopment pre-operatively as an indicator of future neurodevelopmental performance.Reference Uzark, Smith, Donohue, Yu and Romano 5 , Reference Owen, Shevell and Donofrio 15 , Reference Limperopoulos, Majnemer, Shevell, Rosenblatt, Rohlicek and Tchervenkov 16 , Reference Massaro, Glass and Brown 25 Pre-operative and post-operative neurodevelopmental assessments may identify functional health impairments associated with early CHD management, such as surgical and pharmaceutical interventions and the intensive care environment. Early identification of these impairments informs implementation of neuroprotective measures and clinical management strategies, such as individualised developmentally supportive care,Reference Massaro, Glass and Brown 25 , Reference Lisanti, Cribben, Connock, Lessen and Medoff-Cooper 26 and assists with clinical prioritisation and targeted long-term follow-up.
The primary aim of this study was to investigate pre-operative and post-operative neuromotor performance of infants undergoing early open-heart surgery. Second, we aimed to identify risk factors contributing to adverse developmental outcomes at 6 months of age, to inform clinical prioritisation and implementation of long-term care pathways.
Methods
Study design
This was a prospective cohort study of infants with CHD who underwent open heart surgery before 4 months of age. Infants were recruited through the Queensland Paediatric Cardiac Service at the former Mater Children’s Hospital and subsequently the Lady Cilento Children’s Hospital in Brisbane, Australia, between August 2014 and September 2015. The study was approved by the Mater Human Research Ethics Committee 8 May, 2014 (HREC/14/MHS/59).
Infants were screened for eligibility via medical records and in consultation with cardiac surgeons and surgical care coordinators. Signed consent was gained from parents/carers pre-operatively, only after surgeons had discussed the need for surgery. Infants requiring emergency surgery, where there was no opportunity for pre-operative recruitment, were recruited post-operatively before hospital discharge.
Participants
Infants were eligible for the study if they had CHD requiring open-heart surgery before 4 months of age. Infants were excluded from the study if they underwent (a) surgery at another hospital or (b) alternative cardiac interventions for CHD (e.g. catheterisation). Infants with chromosomal abnormalities were included in the study to ensure accurate representation of the clinical population.
Measures
Prechtl’s Method of the Qualitative Assessment of General MovementsReference Einspieler, Prechtl and Bos 27 and the Test of Infant Motor PerformanceReference Campbell 28 were selected as pre-operative and pre-discharge measures for assessing neuromotor performance. Clinical neurological examination was conducted as part of routine care.
The General Movements was selected for the assessment of spontaneous voluntary movement in this fragile high-risk cohort, owing to its non-invasive administration and ability to predict later neurological impairment.Reference Einspieler, Marschik, Bos, Ferrari, Cioni and Prechtl 29 , Reference Noble and Boyd 30 This assessment has strong inter- and intra-rater reliability, the best sensitivity and specificity compared with other neonatal assessment tools, and good predictive validity for later motor dysfunction.Reference Noble and Boyd 30 , Reference Spittle, Doyle and Boyd 31 Cramped synchronised general movements and absent fidgety movements are highly predictive of cerebral palsy,Reference Einspieler, Marschik, Bos, Ferrari, Cioni and Prechtl 29 – Reference Bosanquet, Copeland, Ware and Boyd 32 and abnormal general movements may be associated with cognitive dysfunction at school age in pre-term infants.Reference Einspieler, Bos, Libertus and Marschik 33 Writhing movements are assessed from birth – 26 weeks post menstrual age – to 8 weeks, and categorised into normal, hypokinesis, poor repertoire, chaotic, or cramped-synchronised; fidgety movements are assessed from 9 to 15 weeks, and are categorised into normal fidgety, abnormal fidgety, and absent fidgety.Reference Einspieler, Prechtl and Bos 27 In this study, categories were collapsed to normal – normal writhing and normal fidgety – and abnormal – all other categories – owing to the small study size.
The Test of Infant Motor Performance was selected as a normed, validated, and reliable tool for assessing postural and selective motor control needed for functional performance in early infancy.Reference Campbell, Zawacki and Rankin 34 The Test of Infant Motor Performance has strong inter- and intra-rater reliability and has been shown to be useful for detecting developmental deviance in young infants.Reference Campbell, Zawacki and Rankin 34 Administration of the 42 items assesses development of head and trunk control, as well as selective control of arms and legs. The assessment can be used from 34 weeks of postmenstrual age through to 17 weeks of chronological age for term infants, or 4 months corrected age for pre-term infants. Observed items are scored 0 (not observed during spontaneous activity) or 1 (observed). Elicited items have rating scales with 4–7 levels. Total raw scores range from 0 to 142.Reference Campbell 28 Raw scores were converted to age-adjusted z-scores.
The Ages and Stages Questionnaire 3rd editionReference Squires and Bricker 35 was selected as a well-validated tool to screen development at 6 months of age, and a cost-effective means of following up all participants via telephone. The Ages and Stages Questionnaire is a caregiver-rated questionnaire that screens development in children aged 1–66 months across five domains: communication, gross motor, fine motor, problem-solving, and personal social functioning.Reference Squires and Bricker 35 The questionnaire includes multiple-choice questions reflecting developmental milestones, and open-ended questions eliciting caregiver concern. Multiple-choice questions are scored depending on whether the item is performed consistently (10 points), sometimes (5 points), or not yet (0 points). Domain scores are summarised and categorised as above, close to (1 SD below) or below (2 SD below) the age-defined cut-off scores. For this study, categories were collapsed to normal (above cut-off) and delayed (close to or below cut-off) owing to the clinical relevance of mild delay in this cohort and consequent low threshold for referral for assessment.Reference Marino, Lipkin and Newburger 2 , Reference Mussatto, Hoffmann and Hoffman 36 , Reference Noeder, Logan and Struemph 37
Procedures
Neuromotor performance of infants enrolled in the study was assessed at two time points: (1) before cardiac surgery and (2) after cardiac surgery before hospital discharge. Where possible, timing of assessments was standardised to the day before or of surgery, and the day of hospital discharge. Infants unable to undergo pre-operative assessment were included in the study for pre-discharge assessment. Overall development was assessed at 6 months of age.
Neuromotor assessments were administered by an experienced occupational therapist (M.C.), formally trained in the utilisation of both tools, and accredited through the general movements trust. Assessments were conducted in the cot or incubator in the cardiac ward or paediatric ICU and were video-recorded for later scoring. Clothing was minimised to enhance observation of performance, and lines and attachments were positioned to optimise freedom of movement. For Assessment of General Movements and spontaneous movement items of the Test of Infant Motor Performance, infants were video-recorded in supine position for 5–10 minutes during alert wakefulness. Test of Infant Motor Performance items assessing elicited movement required infants to maintain alert wakefulness while being moved through a series of postures reflecting caregiving practices. Administration time was 15–30 minutes depending on state regulation and fragility of the infant. Settling techniques were applied throughout the assessments as required. Infants requiring frequent settling, and those receiving pharmacological interventions influencing activity and arousal levels, required increased assessment time. Where testing was interrupted or unable to be continued owing to the infant’s state, missed items were administered within 24 hours, as recommended in the test user’s manual.Reference Campbell 28 This was not possible for infants assessed on the day of surgery, leading to longer administration times. The Ages and Stages Questionnaires were administered via telephone with caregivers once infants were 6 months of age.
Scoring of assessments was completed by the assessor. All General Movements scores were confirmed by two General Movements Trust advanced trained raters, provided with the age of participants but blinded to clinical and diagnostic information.
Demographic data collection
Clinical and demographic information of participants was collected from the Queensland Paediatric Cardiac Service surgical database. Demographic information included gender, gestation in weeks, weight and age at the time of surgery, primary cardiac diagnosis, co-morbidities, and caregiver level of education. Clinical information included surgical procedure, cardiopulmonary bypass, aortic cross-clamp time, circulatory arrest time, duration of mechanical ventilation, number of complications, length of stay (ICU and hospital), and method of feeding at discharge. The Aristotle Comprehensive Complexity Score was collected as a measure of complexity of both the procedure and the patient, comprising the Aristotle Basic Complexity Score as an indicator of technical difficulty and the Aristotle Patient-adjusted Complexity Score reflecting inherent patient risk.Reference Lacour-Gayet, Clarke and Jacobs 38 , Reference Lacour-Gayet and Clarke 39 When infants were unable to undergo pre-operative or pre-discharge assessment, reasons were ascribed to infant – for example, unable to maintain state for testing – or environment-related – for example, discharged before testing – factors. Demographic information is summarised in Table 1.
Table 1 Demographic, clinical, and surgical characteristics

ACC=Aristotle Comprehensive Complexity Score; ABC=Aristotle Basic Complexity Score; APAC=Aristotle Patient-adjusted Complexity Score; Aox=aortic cross-clamp; Ax=assessment; CA=circulatory arrest; CPB=cardiopulmonary bypass; GMs=Prechtl’s General Movements assessment; HLHS=hypoplastic left heart syndrome; ICU=intensive care unit; IPPV=intermittent positive pressure ventilation; IQR=interquartile range; n=number; post-op=post-operative; pre-op=pre-operative; TGA=transposition of great arteries; TIMP=test of infant motor performance
* Chromosomal abnormalities included trisomy 21 (n=6), trisomy 16 (n=1), and 22q11 (n=2)
** Complications included delayed chest closure, systemic vein obstruction, wound infection, arrhythmia (+/− necessitating pacemaker), vocal cord dysfunction, seizure, chylothorax, pneumothorax, and renal failure
*** Study participants requiring CA, total (n=14), pre-operative assessment group (n=3), no pre-operative assessment group (n=11)
Statistical analysis
STATA statistical software package version 13.0 was used for all statistical analyses. 40 Descriptive statistics were used to summarise participants’ demographic and clinical characteristics. Means and standard deviations were used to summarise continuous data, and frequencies and percentages for categorical data. Continuous measures were checked for normality using visual inspection of histograms and the Shapiro–Wilk test. Comparison of pre–post performance was analysed using McNemar’s test for categorical general movements, and Wilcoxon’s signed rank test for continuous test of infant motor performance z-scores. Univariate logistic regression was used to identify associations between dependent clinical factors and patient characteristics on dichotomous ages and stages outcome categories. Variables meeting a p-value threshold of <0.2 were checked for collinearity and included in multivariate logistic regression models using backward elimination of variables. All final models were checked and assumptions for logistic modelling met.
Results
Participant characteristics
A total of 123 infants were screened for eligibility, and 60 were recruited to the study (see Fig 1 for study flow). Median gestational age at birth was 38.78 weeks (interquartile range=36.93–39.72) and median age at the time of surgery was 1.86 weeks (interquartile range=0.93–6). Demographic, clinical, and surgical data are presented in Table 1.
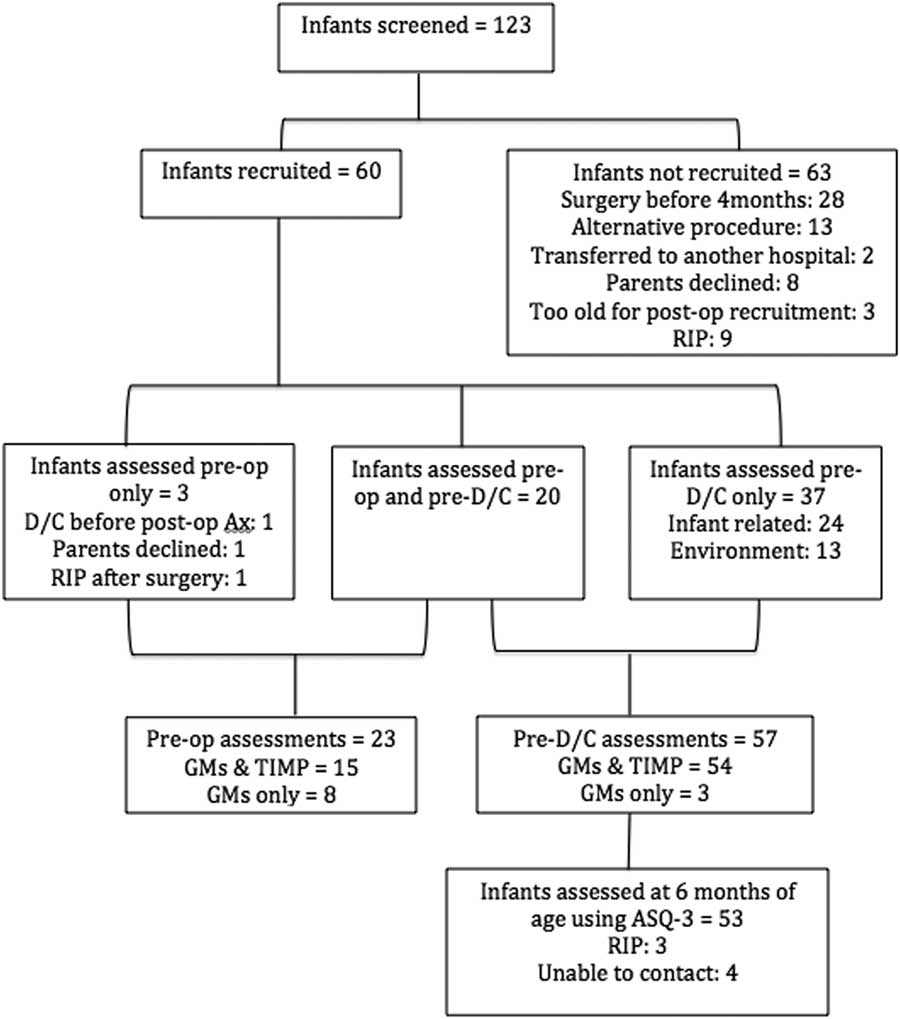
Figure 1 Recruitment flowchart. D/C=discharged; pre-op=pre-operative; post-op=post-operative; RIP=deceased.
Of the 60 infants enrolled in the study, 23 (38%) participated in pre-operative assessment, 15 (25%) in both the General Movements and Test of Infant Motor Performance, and eight (13%) in the General Movements test only owing to medical and/or physiological instability with handling. We have previously reported the feasibility of pre-operative assessment in this cohort.Reference Campbell, Rabbidge, Ziviani and Sakzewski 41
Pre-operative assessment
Median age of infants at pre-operative assessment was 3 weeks corrected gestational age (interquartile range=0–6). Before surgery, 14 (61%) infants assessed presented with normal General Movements, five (22%) with poor repertoire, three (13%) with hypokinesis, and one (4%) with cramped synchronised movements. Of the 15 infants who completed the Test of Infant Motor Performance, three (20%) performed within the average to low-average range (0.5–1 SD below the mean) and 12 (80%) in the below to far-below-average range (1.5–2 SD below the mean). The median age-adjusted z-score was −1.39 (interquartile range=−1.78 to −1.06). Pre-operative assessment results are outlined in Table 2.
Table 2 Results of pre-operative, pre-discharge, and 6-month assessments

ASQ-3=ages and stages questionnaire 3rd edition; GMs=Prechtl’s general movements assessment; IQR=interquartile range; n=number; post-op=post-operative; TIMP=test of infant motor performance; SD=standard deviation
Normal ASQ-3 – above cut-off; Delayed ASQ-3 – ⩾1 SD below cut-off
* McNemar based on n=21 for infants assessed pre-operatively and pre-discharge
** Wilcoxon signed rank based on n=13 for infants assessed pre-operatively and pre-discharge
Pre-discharge assessment
A total of 57 (95%) infants underwent pre-discharge assessment: one died in the post-operative period, one was discharged before assessment, and the parents of one declined assessment on the day of discharge. An additional three (5%) infants were unable to maintain a quiet alert state for Test of Infant Motor Performance administration, participating in the General Movements only. Median age at pre-discharge assessment was 5 weeks corrected gestational age (interquartile range=2–8). Normal general movements were observed in 42 (74%) infants: 29 (51%) in the writhing age and 13 (23%) in the fidgety age. In all, 12 (21%) infants presented with poor repertoire, one (1.8%) with chaotic movements, and two (3.5%) with cramped synchronised movements. Clinical neurological examination of the infants with cramped synchronised and chaotic general movements was abnormal. Below-average to far-below-average performance on the test of infant motor performance was observed in 22 (40.7%) infants, and median age-adjusted z-score was −0.93 (interquartile range=−1.4 to −0.69). There were no significant differences between pre-operative and pre-discharge general movements (p=0.63) or Test of Infant Motor Performance scores (p=0.28) on McNemar’s and Wilcoxon’s signed rank test, respectively. Pre-discharge assessment results are outlined in Table 2.
Six-month assessment
Overall development at 6 months of age was assessed in 53 (88%) infants at a median age of 6 months 10 days (27.14 weeks, interquartile range=26.14–28.57): one infant died in the post-operative period, two died before the 6-month assessment, and four were unable to be contacted. Results of the 6-month assessment are presented in Table 2. Median time between discharge and the 6-month assessment was 21.14 weeks (interquartile range=16.86–24.14). Gross motor delay was most commonly identified, in 28 (52.8%) infants. Both infants who presented with cramped synchronised movements at hospital discharge had motor delay at 6 months of age, and had received a diagnosis of cerebral palsy. Delay in personal–social skills was identified in 18 (34%) infants, fine motor skills in 12 (22.6%), problem-solving skills in 10 (18.9%), and communication in eight (15.1%).
Predictive models
Univariate logistic regression identified significant independent variables for inclusion in multivariate modelling for each outcome domain, as listed in Table 3. Statistically significant variables for each domain were included in predictive multivariate regression models for each ages and stages developmental domain, as outlined in Table 4. When adjusted for time between pre-discharge and 6-month assessment, gross motor delay was negatively associated with gestational age (p=0.03), length of hospital stay (p⩽0.01), and Test of Infant Motor Performance score at discharge (p⩽0.01). Delayed personal social skills were also negatively associated with gestational age (p=0.02), Test of Infant Motor Performance score at discharge (p=0.01), and length of hospital stay (p⩽0.01). Length of hospital stay was also significantly associated with delayed fine motor skills (p=0.05) and duration of mechanical ventilation with delayed problem-solving skills (p=0.02).
Table 3 Factors associated with ASQ-3 outcome at 6-month assessment, using univariate logistic regression

APAC=Aristotle patient-adjusted complexity; ASQ=ages and stages questionnaire, 3rd edition; CI=95% confidence interval; GMs=Prechtl’s general movements assessment; IPPV=intermittent positive-pressure ventilation; ICU=intensive care unit; LOS=length of stay; n=number; No.=number; OR=odds ratio; Pre-D/C=pre-discharge; TIMP=test of infant motor performance; wks=weeks
*p<0.05 (statistically significant)
Excluded variables not reaching significance included cyanotic, chromosomal abnormality, age at surgery, palliative procedure, Aristotle Basic and Comprehensive Complexity scores, aortic cross-clamp time, circulatory arrest time, cardiopulmonary bypass time, feeding method at discharge, maternal and paternal education
Table 4 Factors associated with ASQ-3 outcomes at 6-month assessment, using multivariate logistic regression analyses

ASQ=ages and stages questionnaire, 3rd edition; CI=95% confidence interval; n=number (variation due to missing data TIMP scores); OR=odds ratio; SE=standard error; TIMP=test of infant motor performance
*p<0.05 (statistically significant)
Discussion
Our study aimed to compare pre-operative and post-operative neuromotor performance and identify risk factors associated with delayed development at 6 months of age in infants undergoing open-heart surgery before 4 months of age. Although small pre-operative assessment numbers limited pre–post analysis of neuromotor performance, we found that known risk factors and delayed neuromotor performance on the Test of Infant Motor Performance at discharge were associated with delayed development at 6 months of age.
Gross motor delay compared with other developmental domains was the most common functional health impairment at 6 months of age, which is consistent with previous studies.Reference Chorna, Baldwin and Neumaier 4 , Reference Newburger, Sleeper and Bellinger 22 , Reference Mussatto, Hoffmann and Hoffman 36 , Reference Long, Harris, Eldridge and Galea 42 Similar to previous findings, length of hospital stayReference Hovels-Gurich 8 , Reference Newburger, Sleeper and Bellinger 22 , Reference Mackie, Alton and Dinu 43 and gestational ageReference Gunn, Beca and Hunt 18 were significantly associated with delays in gross motor skills at 6 months of age. Length of hospital stay was also significantly associated with delays in fine motor and personal–social skills, and duration of mechanical ventilation with problem-solving skills.Reference Hovels-Gurich 8 , Reference Newburger, Sleeper and Bellinger 22 , Reference Mackie, Alton and Dinu 43 Although analysis for effects of anatomical CHD diagnosis on 6-month outcomes was not possible owing to low numbers, no significant difference was found between cyanotic and acyanotic groups. Single-ventricle physiology, however, was associated with delayed gross motor and problem-solving skills in univariate analysis.Reference Newburger, Sleeper and Bellinger 22 , Reference Bellinger, Watson and Rivkin 24 We did not find any significant association between intra-operative factors such as length of cardiopulmonary bypass or circulatory arrest on 6-month outcomes. Other studies have reported length of circulatory support time as a risk factor;Reference Gaynor, Stopp and Wypij 20 however, our small sample size precluded further analysis, and only two of the 14 infants who underwent circulatory arrest required deep hypothermic arrest.
Longitudinal studies have established the impact of perioperative risk factors on long-term morbidity;Reference Hovels-Gurich 8 , Reference Gaynor, Stopp and Wypij 20 , Reference Gaynor, Stopp and Wypij 23 however, the focus has shifted to neurodevelopmental evaluation before and after surgery to predict later development.Reference Uzark, Smith, Donohue, Yu and Romano 5 , Reference Owen, Shevell and Donofrio 15 , Reference Massaro, Glass and Brown 25 We demonstrated an association between abnormal general movements and lower test of infant motor performance scores at hospital discharge and gross motor delay at 6 months of age. To our knowledge, this is the first study that explored the association between pre-discharge performance on the general movements and test of infant motor performance and development at 6 months of age in a post-cardiac-surgery cohort. Other studies identified relationships between pre- and post-operative neurodevelopmental performance,Reference Limperopoulos, Majnemer, Shevell, Rosenblatt, Rohlicek and Tchervenkov 16 , Reference Massaro, Glass and Brown 25 or associations between clinical risk factors and post-operative motor performance,Reference Uzark, Smith, Donohue, Yu and Romano 5 but did not investigate associations between early post-operative performance and later development. Longitudinal developmental follow-up studies have identified atypical gross motor performance in the first year of life,Reference Sananes, Manlhiot and Kelly 21 , Reference Long, Harris, Eldridge and Galea 42 but have not conducted pre-discharge assessment for prediction of later development. Crowle et alReference Crowle, Walker, Galea, Novak and Badawi 44 assessed infants following cardiac and non-cardiac surgery using the general movements in the writhing and fidgety stages, and the Bayley Scale of Infant Toddler Development – 3rd Edition at 3 months of age. There was no association between writhing movements and 3-month outcomes, but absent fidgety movements were associated with lower scores on all subtests of the Bayley-III. Assessing the trajectory of general movements post-operatively can assist with informing follow-up; however, the absence of pre-operative assessment limits early identification of atypical neurodevelopment and opportunities to modify the environment and care practices.Reference Uzark, Smith, Donohue, Yu and Romano 5 Individualised developmental care approaches have been well established in neonatal ICUs with preterm infants,Reference Moody, Callahan, Aldrich, Gance-Cleveland and Sables-Baus 45 , Reference Als, Duffy and Mcanulty 46 and this approach is now being introduced in cardiac ICUs around the world.Reference Lisanti, Cribben, Connock, Lessen and Medoff-Cooper 26 , Reference Butler, Huyler, Kaza and Rachwal 47 , Reference Sood, Berends and Butcher 48 Similarities in clinical vulnerability associated with neurological dysmaturation and intervention requirements demand a similar focus to minimise risk associated with environmental and care practices on long-term neurodevelopment.Reference Lisanti, Cribben, Connock, Lessen and Medoff-Cooper 26
Implementing routine pre-operative assessment is valuable;Reference Latal 49 however, it presents challenges with critically unwell infants,Reference Massaro, Glass and Brown 25 , Reference Pike, Pemberton and Allen 50 particularly when interventions such as intubation preclude the handling required for administering assessments.Reference Owen, Shevell and Donofrio 15 The General Movements is a favourable pre-operative assessment when medical fragility precludes infant handling, and offers good predictive validity for later motor dysfunction,Reference Noble and Boyd 30 , Reference Spittle, Doyle and Boyd 31 with cramped synchronised and absent or abnormal fidgety movements being highly predictive of later neurodevelopmental delay.Reference Einspieler, Marschik, Bos, Ferrari, Cioni and Prechtl 29 This tool has been well validated in the preterm infant population,Reference Einspieler, Prechtl and Bos 27 but to date has not been widely used in the cardiac population. Crowle et alReference Crowle, Walker, Galea, Novak and Badawi 44 reported that most infants presenting with poor repertoire in the writhing stageReference Crowle, Badawi, Walker and Novak 51 had normal fidgety movements at 12 weeks.Reference Crowle, Walker, Galea, Novak and Badawi 44 Infants who had undergone cardiac surgery, however, had a worse trajectory, with a higher incidence of absent fidgety movements and lower scores on the Bayley-III at 3 months compared with the non-cardiac group. As the General Movements has become a more frequently recognised diagnostic tool in infants with CHD, further evaluation of the predictive validity after open-heart surgery is warranted to inform long-term follow-up requirements.
The Ages and Stages Questionnaire was the primary outcome variable for this study. We grouped scores in the close to cut-off or “monitor” category (1 SD below the mean), with those in the below cut-off or “refer” category (2 SD below the mean) to represent “delayed development” for this cohort. Typically, infants and children with CHD present with low severity or combined developmental delay, and a low threshold for follow-up assessment and evaluation of those “at risk” is warranted to instigate early intervention.Reference Marino, Lipkin and Newburger 2 , Reference Brosig, Butcher and Butler 3 , Reference Mussatto, Hoffmann and Hoffman 36 , Reference Noeder, Logan and Struemph 37 Noeder et alReference Noeder, Logan and Struemph 37 examined the psychometric properties and clinical utility of the ages and stages questionnaire compared with the Bayley-III in the CHD population at 6, 12, 24, and/or 36 months of age. Specificity was high across all domains in the “at-risk” (⩾81.9%) and “below cut-off” (⩾93.6%) categories, and negative predictive value was high in the gross motor subtest, with 84.9% of failed screening associated with true delay on the Bayley-III. This is of particular importance to the CHD population, given the high incidence of gross motor delays in the first year of life.Reference Snookes, Gunn and Eldridge 1 , Reference Newburger, Sleeper and Bellinger 22 , Reference Mussatto, Hoffmann and Hoffman 36 , Reference Long, Harris, Eldridge and Galea 42 Although sensitivity varied across subtests, overall specificity was >93% across all domains.Reference Noeder, Logan and Struemph 37 The Ages and Stages Questionnaire is a low-resource developmental surveillance option, which, combined with known clinical risk factors, offers the ability to screen all at-risk infants in the absence of formal developmental follow-up programmes. Given the frequency of low severity delays in this clinical cohort, a higher level of caution should be adopted when interpreting “at-risk” scores, and referral for developmental assessment and evaluation considered for children scoring ⩾1 SD below the mean in any Ages and Stages domain.Reference Marino, Lipkin and Newburger 2 , Reference Mussatto, Hoffmann and Hoffman 36 , Reference Noeder, Logan and Struemph 37
Our study had several limitations. This was a single-centre study conducted during the time period of a major hospital translocation, affecting timing of surgery for infants and reflecting outcomes of surgical and post-operative management of one service only. The study size was limited to 60 infants owing to the 12-month study time frame. Inclusion of a mixed diagnostic cohort inclusive of chromosomal abnormalities, while representative of this heterogenic cohort, may present a risk to the rigour of developmental outcome scores in larger cohorts. Recruitment was restricted to infants under 4 months of age as the Test of Infant Motor Performance has only been validated for infants up to 17 weeks corrected age. Small pre-operative assessment numbers precluded pre–post analyses to evaluate differences in performance before and after surgical intervention. Timing of assessment administration was constrained in this study design owing to variability in age at the time of surgery and hospital discharge. Although administration at key time points is recommended in longitudinal research studies to strengthen predictive validity,Reference Einspieler, Prechtl and Bos 27 this study was interested in the clinical utility and association between abnormal or delayed neuromotor performance at discharge and delayed development at 6 months. Evaluation of development using the Ages and Stages Questionnaire enabled follow-up of all participants within available resources limitations. Using the Alberta Infant Motor ScalesReference Piper and Darrah 52 or Infant Motor ProfileReference Heineman, Bos and Hadders-Algra 53 would have strengthened analysis of motor performance along the developmental continuum, but was not possible within the constraints of this study. Recommended follow-up beyond 6 months of ageReference Marino, Lipkin and Newburger 2 was not possible within the study time frame, limiting evaluation of domains consolidated later in childhood, such as communication and cognition.
This study identified that early neuromotor delay can be predictive of later motor development, and in conjunction with known clinical risk factors provides a more robust method of risk stratification, implementation of early intervention, and follow-up planning. There is variability in the provision of long-term neurodevelopmental follow-up programmes internationally.Reference Brosig, Butcher and Butler 3 , Reference Michael, Scharf, Letzkus and Vergales 54 While the American Heart Association guidelines recommend surveillance and evaluation at key time points,Reference Marino, Lipkin and Newburger 2 several challenges affect adherence to these recommendations. Access to, and cost of, services typically centralised in tertiary centres presents challenges for families in geographically remote areas. Furthermore, the increasing demands on services as more infants are surviving into adulthood presents challenges to allocation of finite resources. Chorna et alReference Chorna, Baldwin and Neumaier 4 acknowledged inefficiencies in duplication of services and advocated for capitalising on existing resources, such as care co-ordination from Cardiology and multidisciplinary follow-up from well-established neonatal follow-up programmes. Although this approach may be feasible in some centres, it highlights the need for contextualised follow-up programmes based on structure and availability of local health services. Follow-up programmes have historically been provided centrally by acute hospital teams, and limited to high-risk diagnostic groups. The focus has now shifted to establishing a state-wide approach to long-term neurodevelopmental follow-up, using services across the care continuum to enable local and equitable access to surveillance, evaluation, and management, in accordance with best practice guidelines.Reference Marino, Lipkin and Newburger 2
Conclusion
Infants who undergo open-heart surgery before 4 months of age are at risk for poor long-term neurodevelopmental outcomes owing to peri-operative factors. Pre-operative evaluation of this cohort is challenging owing to medical fragility and environmental barriers, but is recommended to guide individualised care practices. Administering the General Movements and Test of Infant Motor Performance before hospital discharge provides valuable information to inform early intervention requirements and long-term surveillance. Longitudinal follow-up beyond 6 months of age is recommended as skill acquisition progresses. An ongoing focus on the benefits of early intervention and a collaborative approach to risk mitigation is required to minimise the long-term impact on developmental outcomes.
Acknowledgements
The authors thank the infants and families who participated in this study, Dr Ben Auld (Cardiologist) for assisting with pre-operative and pre-discharge clinical neurological review of participants, and Lyndal Franklin and Lisa Findlay (Occupational Therapists) for review of general movements assessments.
Financial Support
This study was supported by a HeartKids grants-in-aid grant, funded by The Hospitals Contribution Fund of Australia Ltd (HCF). Leanne Sakzewski was supported by a NHMRC ECR Fellowship (1090828).
Conflicts of Interest
None
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation (National Health and Medical Research Council, Australia) and with the Helsinki Declaration of 1975, as revised in 2008, and has been approved by the institutional committees (Mater Human Research Ethics Committee).





