Introduction
Septoplasty is a basic surgical procedure in the field of otorhinolaryngology, and is commonly performed to correct septal deviations. Stammberger and Posawetz first described the endoscopic application of septoplasty to treat septal deviation in 1990.Reference Stammberger and Posawetz1 Since then, numerous surgeons have adopted endoscopic septoplasty because the method has several advantages in terms of visualisation and minimal invasiveness. Despite the use of endoscopic techniques, complications such as post-operative haematoma and nasal septum perforation can still occur, suggesting that further refinement of the technique is necessary to reduce the incidence of complications.
Nasal packing is commonly performed in many institutions to prevent post-operative complications such as bleeding, septal haematoma, displacement of cartilage and synechia. However, this procedure can cause discomfort, pain, mucosal injury, toxic shock syndrome and breathing difficulties. Several alternative nasal septum suturing techniques have been reported to be more effective, reliable and comfortable for the patient than nasal packing.Reference Günaydın, Aygenc, Karakullukcu, Fidan and Celikkanat2–Reference Cukurova, Cetinkaya, Mercan, Demirhan and Gumussoy6
Septoplasty can be complicated by septal perforation, crusting, bleeding and nasal obstruction. Although several reports have described the use of suturing to repair perforations of the nasal septum,Reference Li, Liu, Yu and Zhang7, Reference Chen, Rui, Deng, Wen, Xu and Shi8 large perforations can be particularly difficult to treat.Reference Chen, Rui, Deng, Wen, Xu and Shi8 Thus, avoidance of nasal septum perforation is paramount. For cases in which the bilateral nasal septum mucosa is torn during septoplasty, repair is required to prevent nasal septum perforation.
However, suturing the nasal mucosa can be problematic: perpendicular insertion of a curved needle into the nasal mucosa is quite difficult. In 2013, a new endonasal suturing instrument equipped with a straight needle, the Maniceps septum stitch device (Mani, Tochigi, Japan), was developed for septal surgery to address these issues (Figure 1). Here, we describe our clinical experience with the Maniceps septum stitch device, which was used to suture the nasal septum during septoplasty.

Fig. 1 Maniceps septum stitch device: the jaw width of the device (‘a’) is wider than that of the conventional Maniceps instrument, with an effective length (‘b’) of 55 mm and a total length (‘c’) of 220 mm.
Materials and methods
Septum stitch device
The Maniceps septum stitch system is a new and improved iteration of the conventional Maniceps device (Mani, Tochigi, Japan) used for nasal septum surgery. The Maniceps device is a suturing instrument shaped like a pair of forceps (Figure 1). The grasping ability of the Maniceps septum stitch device allows suturing of a deep area of tissue during open or endoscopic surgery. This device was originally intended for other areas of surgery, such as in the urological field. One jaw of the instrument holds a straight needle with a suture thread (length, 5 mm), which is transferred to the jaw tip when the device is closed. The tip of the Maniceps septum stitch forceps is shown in Figure 2.

Fig. 2 Photographs of the tip of the forceps: (a) on one side, the device is equipped with a 4-0 straight needle and suture thread; (b) the forceps jaw tips close upon grasping; and (c) the straight needle with suture thread is taken by the opposite jaw tip.
The concept of the improved Maniceps septum stitch system is the same as that of the conventional Maniceps device; however, the shape has been altered to facilitate the placement of sutures into the nasal septum. Three major modifications have been made to the device for better approximation of the anatomical structure of the nasal septum: (1) the jaw width of the forceps is wider, which makes it easier to insert the device into the posterior nasal septum; (2) the effective length of the Maniceps septum stitch device is 55 mm and the total length is 220 mm (Figure 1), which allows a larger space for the endoscope; and (3) the device employs a finer absorbable 4-0 suture thread.
Surgical technique
All surgical procedures were performed using a 0° rigid endoscope (Karl Storz, Tuttlingen, Germany) under general anaesthesia at Dokkyo Medical University Hospital (Mibu, Japan). An initial incision was made 10 mm cephalad to the caudal end of the septal cartilage, and the septal cartilage was separated from the perichondrium of the nasal septum. After removing the deviated cartilage or part of the vomer and perpendicular plate of the ethmoid bone, we repositioned the cartilage in its original location.Reference Takahashi and Takahashi9
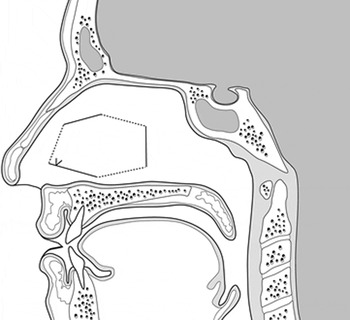
Following septoplasty, we sutured the transnasal septum using a 4-0 straight needle with absorbable thread that was pinched at the tip of one jaw of the Maniceps septum stitch device. Each jaw of the Maniceps septum stitch device was inserted into the respective nostril. When the device is closed, the opposing jaw grasps the needle tip. The first suture was placed in the posterior nasal septum, which was originally in the area of the vomer and perpendicular plate, in which haematomas frequently occur. After placing the first suture, we removed the Maniceps septum stitch device from the nasal cavity and repositioned the tip to the side holding the needle. Next, we reinserted the Maniceps septum stitch device into the nasal cavity to suture the anterior septum horizontally with the septal cartilage. The same procedure was repeated three or four times on the elevated part of the septum. We also performed the continuous mattress suturing techniqueReference Sessions10 (Figure 3), also known as a ‘quilting suture’.Reference Hari, Marnane and Wormald11, Reference Shah, Kumari, Pradhan and Thapa12
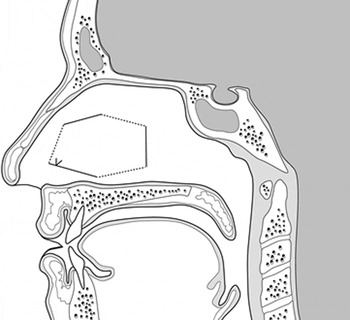
Fig. 3 Illustration of continuous mattress suturing (i.e. ‘quilting suture’ technique) of the nasal septum.
For cases in which the bilateral opposing nasal septum mucosa was torn, we sandwiched the cartilage between the injured septal mucosa (Figure 4). The inserted cartilage was gently covered with the injured mucosa of the nasal septum and sutured together using the Maniceps septum stitch device. Finally, in all cases, we covered the injured mucosal surface with a 1 mm thick silicon plate.
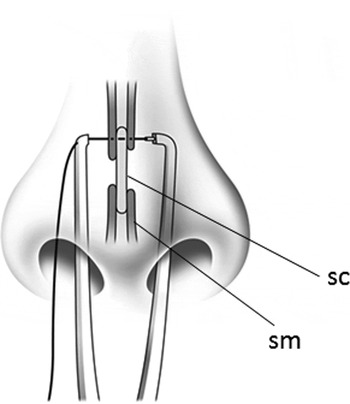
Fig. 4 In this illustration, the nasal septal mucosa is torn and septal cartilage (‘sc’) is sandwiched between the injured septal mucosa (‘sm’). These structures are stitched and fixed together with the Maniceps septum stitch device to prevent perforation.
Results
A retrospective review was performed of 13 patients who underwent nasal septal suturing with the Maniceps septum stitch device for septoplasty between December 2012 and June 2013. Three surgical cases were performed by the junior surgeon (AK) and 10 cases were conducted by the senior surgeon (TN). In three cases, the nasal mucosae were torn, requiring suturing of the mucosa and cartilage and covering with a silicon plate. Quilting suturing was performed for three patients and required 312.6 seconds on average from start to completion. Seven patients were sutured horizontally from the posterior to anterior nasal septum. None of the 13 patients had post-operative perforations or other complications up to 3 months after surgery.
Discussion
Several alternative septal suturing techniques have recently been introduced that appear to have efficacy comparable or preferable to that of nasal packing.Reference Günaydın, Aygenc, Karakullukcu, Fidan and Celikkanat2–Reference Cukurova, Cetinkaya, Mercan, Demirhan and Gumussoy6 However, these suturing techniques are quite difficult to perform. In contrast, the Maniceps septum stitch device allows for easier suturing of the nasal septum owing to the shape of its needle. The most basic suturing technique consists of a needle inserted perpendicularly to the tissue. However, it is difficult to insert a curved needle in a perpendicular fashion into the nasal mucosa. The Maniceps septum stitch device can be used to insert a 4-0 straight needle with an absorbable thread perpendicularly into the nasal mucosa. In addition, the sutures are absorbable and usually do not have to be removed post-operatively.
In recent years, there have been several reports on devices utilised for suturing or fixing the nasal septum. These include the septal stapler, which is advocated by Yildirim et al.Reference Yildirim, Cingi and Kaya13 It is comfortable to use, particularly for those surgeons with less experience who may find it difficult to blindly suture the nasal septum in the nasal cavity. Korkut et al. reported on the efficiency of a novel trans-septal suturing device, in which a straight needle is inserted from one side of the nasal cavity.Reference Korkut, Teker, Eren, Gedikli and Askiner4 Some surgeons are apprehensive when suturing torn nasal mucosa and fixing free cartilage to prevent septal perforation, because the cartilage is often shifted and torn by pressure from the needle when using a one-sided approach.
The Maniceps septum stitch device can potentially solve these problems. Furthermore, it possesses several properties useful for nasal septum suturing. For example, the shape of the Maniceps septum stitch forceps allows for easy suturing of the nasal septum within the visual field of the endoscope and will not damage the lateral wall of the nasal cavity. In addition, this device can accommodate many different types of suturing technique, including quilting suturing,Reference Sessions10, Reference Hari, Marnane and Wormald11 and axial or vertical single suturing, even when the operator is less experienced. Therefore, the use of this device is likely to reduce stress for the surgeon.
The Maniceps septum stitch device can also help to prevent perforation of the nasal septum. Even in cases with a tear on one side of the nasal mucosa, the Maniceps septum stitch device allows easy suturing to stabilise the nasal mucosa of the anterior or posterior nasal septum. For cases in which the bilateral septal mucosa is torn, an approach to enclose the nasal septum on both sides is better than approaching from one side, although the free cartilage may still be shifted by the needle when using a two-sided approach.
Compared to other suturing techniques, the Maniceps septum stitch device appears to be simple, easy to operate and safe for the patient. Post-operative complications, particularly septal perforation, can be considerably reduced through the use of the Maniceps septum stitch device. Although we encountered no cases of septal haematoma or infection with its use, further experience is required to validate these initial findings, including determination of the best suturing technique (e.g. horizontal or quilting) for the nasal septum, and surgical time, among other parameters.
Conclusion
This paper describes the use of a new endonasal instrument for suturing the nasal septum during septal surgery. The Maniceps septum stitch device allows a safe and technically easy surgical procedure (with the option of quilting suturing) that can help to prevent the incidence of nasal perforation as a post-operative complication, by enabling simple suturing of the mucosa and cartilage. We believe that the Maniceps septum stitch device is a valuable new instrument for suturing the nasal septum during septal surgery.