



Introduction
Human leg length and other body proportions are influenced by genetic and environmental factors that can be studied from a human evolution perspective, and in terms of phenotypic variation and patterns of growth in mammals (Bogin et al., Reference Bogin, Kapell, Varela Silva, Orden, Smith, Loucky, Dasgupta and Hauspie2001; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2010). Leg length and trunk length and their proportions (relative to stature) have been used as epidemiological markers of body fat gain, cardiovascular disease and diabetes (Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008). Studies have reported that leg length is an indicator of quality of early life environmental conditions that influence physical growth in children (Gunnell et al., Reference Gunnell, Smith, Frankel, Kemp and Peters1998; Bogin et al., Reference Bogin, Kapell, Varela Silva, Orden, Smith, Loucky, Dasgupta and Hauspie2001; Wadsworth et al., Reference Wadsworth, Hardy, Paul, Marshall and Cole2002; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008).
Body size and body segments have different timings and tempos of growth, and leg length in particular increases faster relative to other body dimensions and matures earlier than stature (Bogin, Reference Bogin1999; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008, Reference Bogin and Varela-Silva2010, Reference Bogin and Varela-Silva2012). Growth of leg length is extremely responsive to nutrient shortage, chronic energy deficiency, infection and other unfavourable life conditions during infancy and childhood, leading to short relative leg length and thereby short adult height (Bogin et al., Reference Bogin, Smith, Orden, Varela-Silva and Loucky2002; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008; Datta Banik et al., Reference Datta Banik, Mirzaei Salehabadi and Dickinson2017). The absolute size and relative leg length to height are thus sensitive indicators of the nutritional status, quality of life and household socioeconomic status of children and adolescents (Bailey et al., Reference Bailey, Xu, Feng, Hu, Zhang and Qui2007; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2010; Pomeroy et al., Reference Pomeroy, Stock, Stanojevic, Miranda, Cole and Wells2012). A study in Merida, Yucatan, reported differential growth patterns of knee height (lower leg length) and stature among 9- to 17-year-old boys and girls (Datta Banik et al., Reference Datta Banik, Mirzaei Salehabadi and Dickinson2017). Knee height showed an earlier age at maximum increment compared with stature. However, velocity at the age of maximum increment was higher for stature than for knee height. Therefore, it may be presumed that leg length, due to its earlier timing of growth compared with stature, is more sensitive to early life environmental conditions, including undernutrition, chronic diseases and poor household socioeconomic status, in the pre-pubertal and pubertal growth periods. If children suffer from chronic undernutrition, their legs may stop growing, and eventually they will have shorter relative subischial leg length (RSLL) in adulthood. Consequently, variability in adult stature can be explained by differential leg lengths and proportions across populations (Bogin et al., Reference Bogin, Smith, Orden, Varela-Silva and Loucky2002; Cole, Reference Cole2003; Bogin, Reference Bogin2013).
Chronic undernutrition and its impact on physical growth in children are the reasons behind having shorter RSLL, and its association with higher body fat has already been reported (Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008), and this calls for further research in different communities. Shorter leg length as a marker of adverse early life environmental conditions and its negative impact on health and nutrition, and association with higher body fat in adulthood, can be explained in the light of evolutionary life history theory (Adair et al., Reference Adair, Popkin, Akin, Guilkey, Gultiano and Borja2011). Childhood is a stage of negligible energy expenditure for reproduction, and energy is therefore used for growth and maintenance with any excess being stored. If children suffer from diseases due to poor environmental conditions, diet and nutritional status, energy is spent for disease prevention and maintenance at the expense of growth. In the explanation of life history theory, a report from Bolivia mentioned inter-relationships between child growth, food intake and the development of the immune system (McDade et al., Reference McDade, Reyes-García, Tanner, Huanca and Leonard2008). This is also true for adults, where unhealthy individuals require higher protein intake than their healthy peers (Powanda & Beisel, Reference Powanda and Beisel2003). A study in rural Yucatan in Mexico reported that the observed high disease incidence and insufficient energy and protein intake rates in children were due to poor socioeconomic status and unhealthy living conditions, which had negative impacts on physical growth (Cuanalo de la Cerda et al., Reference Cuanalo de la Cerda, Ochoa Estrada, Tuz Poot and Datta Banik2014).
The association of leg length with body mass index (BMI), overweight, obesity and body fatness has been much studied (Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008, Reference Bogin and Varela-Silva2010; Bogin, Reference Bogin, Cameron and Bogin2012). Body mass index is considered to be an indicator of nutritional status and adiposity. However, its reliability as an estimate body fat is questionable because it is a measure of height-adjusted body weight, which is composed of body fat and fat-free mass, including muscle, bones, water and organs (WHO, 2004; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2012). In Asian populations, an association of low BMI with relatively higher body fat has been reported, so WHO (2004) proposed a different cut-off for overweight. Studies in India have also reported substantial misclassification of BMI-based overweight in relation to percentage body fat (Misra, Reference Misra2015). This background advocates the estimation of body fat independent of BMI.
Populations living in hilly and mountain regions have the added disadvantage of not having enough minerals in the soil and locally available crops (Anderson, Reference Anderson2007), which might affect growth during childhood. This might influence the leg lengths of individuals, independent of socioeconomic status. This has also been reported in Darjeeling district in West Bengal, India (Biswas et al., Reference Biswas, Das, Chakraborty, Biswas, Sharma and Biswas2014) and in Tibet (Dermience et al., Reference Dermience, Mathieu, Li, Vandevijvere, Claus and De Maertelaer2017). Therefore, it is presumed that the cumulative influence of adverse environmental conditions is responsible for short height in hilly and mountainous populations and differential growth and maturity patterns of leg length, both in terms of absolute size and relative to stature manifest in short leg lengths in such communities.
Therefore, shorter leg length as a marker of unfavourable environment and probable epigenetic effects is an important finding that need to be confirmed through further research across the world in communities living in different physical, social, cultural and economic environments (Bogin & Varela-Silva, Reference Bogin and Varela-Silva2010). Ethnicity plays an important role that may act as a proxy for the genetic background of a community. India is a country with diverse environmental conditions where ethnic groups that are mostly endogamous live under varied socioeconomic conditions (Tamang & Thangaraj, Reference Tamang and Thangaraj2012).
The present research was conducted among the Limbu – an indigenous community from Darjeeling district in West Bengal, India. It was hypothesized that higher body fat would be associated with lower RSLL (Bogin & Beydoun, Reference Bogin and Beydoun2007; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008). The aim was to confirm previous findings (Bogin & Beydoun, Reference Bogin and Beydoun2007; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008) using the somatic characteristics of the Limbu community. It was expected that these relationships might be evident in this community, which has a poor socioeconomic background with the possibility of suffering from the impact of adverse environmental conditions in childhood. The main objective of the study was to evaluate the magnitude of the association of percentage body fat with RSLL, after adjusting for age, sex and BMI, among adolescents and adults.
Methods
Study area and data collection
Data were taken from a cross-sectional study carried out in the Limbu community of Darjeeling district in West Bengal, India, in 2010–2014 that was initially sponsored by the Indian Council of Medical Research, New Delhi (see Acknowledgments). The Limbu is an indigenous community living in the Himalayan and sub-Himalayan regions of West Bengal in India and Nepal. They are also found in Sikkim, another state in the north-eastern part of India. The majority of Limbu households operate a crop-livestock farming system. Limbu men and women also work in government sectors, particularly the army. Based on information from the local Government of West Bengal office in Siliguri City in Darjeeling district, the 2010–14 survey area covered 102 Limbu settlements (villages and hamlets) in Darjeeling, Kurseong, Kalimpong (presently a separate district) and Siliguri sub-divisions near Naxalbari, Bagdogra and Matigara blocks (an administrative division) of the then Darjeeling district. In the absence of separate information in the Census of India (2011) for Limbu community people, the Limbu settlements were identified and a demographic survey was carried out in 85 settlements (selected from the sub-divisions) and a list of 16- to 19-year-old adolescents (n = 129) and 20- to-39-year-old adults (n = 681) was prepared. Inclusion criteria were: 1) member of Limbu community (official identity proof issued by the Government of India for Scheduled Tribe community was checked); 2) resident of Darjeeling district, and 3) citizen of the Republic of India.
Study sample
The present study was based on a purposive, non-probability sample selected from the survey data (Cochran, Reference Cochran1977). It comprised 97 adolescents aged 16–19 years and 260 adults aged 20–39 years, estimated from the size of population with 5% margin of error at 95% confidence level. The adolescents included 47 boys and 50 girls, and the adults 135 men and 125 women. None of the participants reported having any health problems in 3 months prior to the fieldwork.
Anthropometric measurements
Anthropometric measurements were recorded during 2011–14 during household visits, following standard protocol (Lohman et al., Reference Lohman, Roche and Martorell1988). Height (cm) and sitting height (SH, cm) were measured to the nearest tenth of a centimetre using a standard stadiometer with platform (Seca, Germany). A standard anthropometric box 40 cm tall × 50 cm wide × 30 cm deep was used to measure SH. The participant sat on this with their knees bent at a 90 degree angle to their thighs. Body weight was measured to the nearest 0.05 kg using an electronic scale (Seca, model 881, Hamburg, Germany). Subischial leg length (SLL) (cm) was height minus SH. Skinfold thicknesses were measured using a standard caliper (Harpenden, UK). Four skinfold thicknesses were measured (biceps, triceps, subscapular and suprailiac) and the sum of four skinfolds calculated. Derived indices included BMI (weight (kg) divided by height (m) squared) and relative subischial leg length (RSLL) (SLL/stature×100). Percentage body fat (PBF) was estimated from density, using the standard formulas, by age and sex for adolescents and adults (Durnin & Womersley, Reference Durnin and Womersley1974). The specific formulas by age (below 17 years, 17–19 years, 20–29 and 30–39 years) were used. The PBF was estimated using the formula: (4.95/density–4.50)×100 (Siri, Reference Siri1956). All measurements were made by a single researcher (see Acknowledgments) and intra-observer technical error of measurement was within acceptable limits (Ulijaszek & Kerr, Reference Ulijaszek and Kerr1999). An adult woman from the community was always present when anthropometric measurements were being recorded from female participants.
Analysis
Data analysis was done using SPSS statistical software Version 15.00. Descriptive statistics of age and anthropometric variables (mean values and standard deviation) in adolescents and adults were calculated and sex differences of characteristics estimated using Student’s t-test. An effect size measure to interpret standardized difference between two mean values was tested using Cohen’s d. Linear regression models predicting PBF from RSLL and BMI were developed to explain the inter-relationships between the parameters. Models were adjusted for age and sex in adolescents and adults. Statistical significance was set a priori at p<0.05.
Results
Table 1 shows the distribution of the anthropometric characteristics of the adolescent and adult participants by sex. The mean age of the adolescent boys was 17.04 years and that of girls 16.29 years (significantly different at p<0.05); mean age of the adult men was 31.21 years and that of women 30.16 years (not significantly different). All the anthropometric parameters showed a significant sex difference (p<0.05), with the exception of body weight (kg) in adolescents, and relative subischial leg length (RSLL, %), subscapular skinfold (mm) and sum of four skinfolds (mm) in adults. The highest t-values were found for sum of skinfolds among adolescents and height (cm) in adults. Adolescent boys were taller by 9 cm than girls, and men were taller than women by more than 12 cm. The mean RSLL values were marginally higher among girls and women compared with boys and men, respectively. However, mean sitting height and subischial leg length were higher among boys and men than girls and women, respectively. Females (adolescents and adults) showed consistently higher mean values of skinfold thickness, sum of four skinfolds and percentage body fat (PBF). Mean PBF values were higher in girls (22.41%) and women (21.46%) than boys (16.34%) and men (14.72%), respectively. Therefore, females (adolescents and adults) had more than 6% more body fat than their male counterparts. Effect size measures of the standardized differences of mean values of age and anthropometric parameters in male and female participants using Cohen’s d showed similarities with the results obtained using t-test. The Cohen’s d values showed medium (≥0.50) and large (≥0.80) effects in all variables that corresponded with significant sex differences of mean values using the t-test, except for age in adolescents. The Cohen’s d values were <0.20, indicating a small effect for age and body weight among adolescents, age, RSLL, subscapular skinfold and sum of skinfolds among adults (Table 1).
Table 1. Descriptive statistics of participants’ age and anthropometric characteristics, Limbu community, Darjeeling, 2010–14
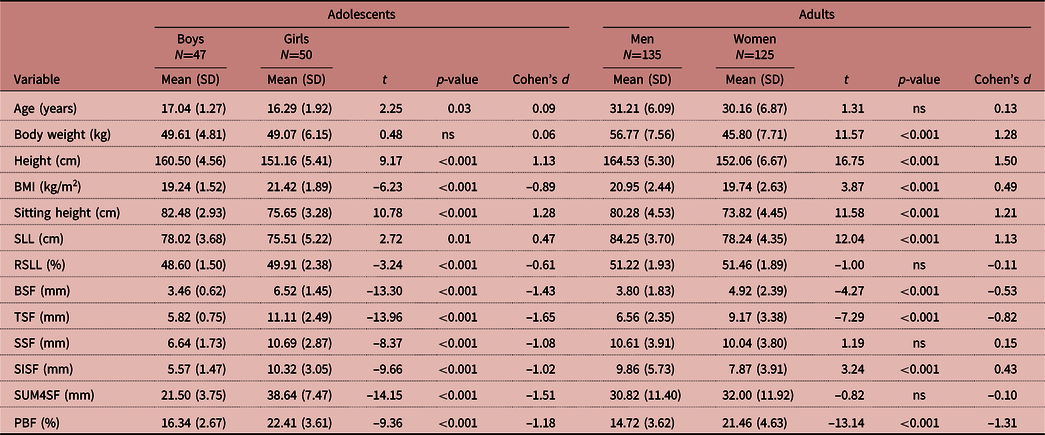
SD: Standard deviation; ns: not significant; BMI: body mass index; SLL: subischial leg length; RSLL: relative subischial leg length; BSF: biceps skinfold; TSF: triceps skinfold; SSF: subscapular skinfold; SISF: suprailiac skinfold; SUM4SF: sum of 4 skinfolds; PBF: percentage body fat.
Multiple linear regression models to find the inter-relationships between PBF, RSLL and BMI, after adjustment for age and sex, are presented in Table 2. Parameter estimates of the response variable (PBF) included 95% confidence intervals for the coefficient. In the models among adolescents and adults, ANOVA p-values of <0.05 indicated a statistically significant relationship between variables. The regression models accounted for 60% and 72% of total variability explained by adjusted R 2 among adolescents and adults. The PBF as a response variable showed 61.50% and 85.0% of variability around the mean in the fitted models, which was explained by the R 2 statistic among adolescents and adults, respectively. The PBF was found to be significantly related to sex (boys and girls) and RSLL among adolescents (p<0.001) and to all the predictors (age, sex, RSLL and BMI) among adults (p<0.001). Among adolescents, for 1% lower RSLL, there was a 0.86% increase in body fat, holding other predictors in the model constant. Among adults there was a 0.36% rise in body fat due to a 1% lower value of RSLL. The regression models for PBF as a response variable are presented in the form:
Table 2. Linear regression models for percentage body fat (PBF) in response to BMI and relative subischial leg length (RSLL) as predictors among adolescents (47 boys, 50 girls) and adults (135 men, 125 women)
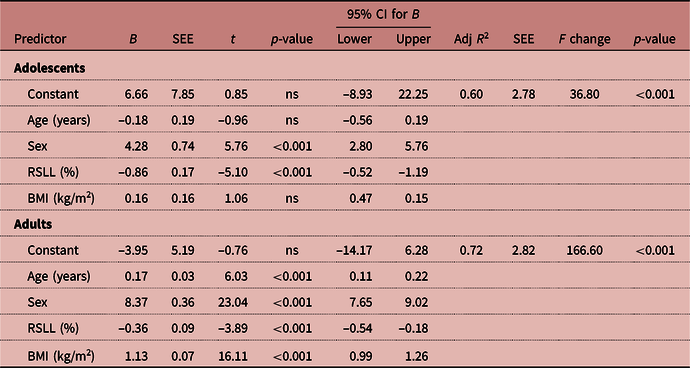
Boys and men=1, girls and women=2.
BMI: body mass index; RSLL: relative subischial leg length; SEE: standard error of estimate; CI: confidence interval; B: regression coefficient; Adj R 2: adjusted R squared; F: F-test in regression; ns: not significant.
Adolescents: PBF=6.66–0.18 Age + 4.28 Sex (boys 1, girls 2) – 0.86 RSLL + 0.16 BMI
Adults: PBF=–3.95 + 0.17 Age + 8.37 Sex (men 1, women 2) – 0.36 RSLL + 1.13 BMI
Relatively high tolerance (>0.87) and low variance inflation factor (<1.02) for the independent variables meant neither model exhibited multicollinearity between predictors. Normality tests (Shapiro-Wilk tests, p>0.05) and P-P plots showed the residuals were normally distributed with no patterns. Durbin–Watson statistics (adolescents: 1.88; adults: 1.76) indicated no autocorrelation in the residuals from the multiple regression analysis.
Discussion
The study results showed a significant negative relationship between percentage body fat (PBF) and relative subischial leg length (RSLL) (%) among adolescents and adults in the Limbu community of West Bengal. This supports the hypothesis that higher body fat is associated with lower RSLL, as proposed in previous studies (Bogin & Beydoun, Reference Bogin and Beydoun2007; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008). The study found that higher body fat, independent of BMI, correlated with lower RSLL among adolescents and adults in this population, indicating a possible association with poor quality of living conditions in childhood. However, it could also be due to the allometry of total body fat with body proportions – a larger trunk results in more body fat as the trunk carries more body fat than do the legs (Norgan, Reference Norgan1994a,b; Norgan & Jones, Reference Norgan and Jones1995; Bogin & Beydoun, Reference Bogin and Beydoun2007).
In the present study, the female participants (adolescents and adults) had a higher mean BMI and PBF than males. The significance of the differences in the mean values of anthropometric characteristics between males and females was tested using the t-test; the magnitude of any differences was ensured by the effect size measure (Cohen’s d). Differences were more evident for adolescents, where the regression coefficients were higher than for adults. Among adolescents, the inter-relationships between PBF and RSLL were significant after adjusting for BMI and other predictors, and adults showed a significant, positive relationship between BMI and PBF. The variability in the height, weight and BMI data was higher among adults than among adolescents.
Previous studies reported that sitting height may be affected by gluteo-femoral fat, which can overestimate the sitting height ratio (SHR) and underestimate RSLL (Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008, Reference Bogin and Varela-Silva2010). However, in the case of the Limbu community this issue was not very important due to the presence of moderate PBF among adolescents and adults. Unpublished results from the same research project (related to the present study) showed the mean waist circumferences (men 69.2 cm, women 68.0 cm) and hip circumferences (men 84.2 cm, women 82.5 cm) of adults were moderate and had no apparent influence on sitting height, suggesting that underestimation of subischial leg length and RSLL was not an issue.
Relatively short leg length in Limbu adults presumably has a long history since their childhood. Datta Banik et al. (Reference Datta Banik and Mukhopadhyay2016), in their study in the Darjeeling district of West Bengal, reported low height-for-age (stunting) among Limbu children and adolescents, below the WHO reference curve for height-for-age. The prevalence of stunting was high in 16- to 18-year-old Limbu adolescents (boys 16%, girls 40%). Lower RSLL is an important predictor of raised body fat (%). However, reports on the health and nutritional status of Limbu adults are not available for this region. Evaluation of the BMI-based nutritional status of Limbu adolescents and adults was not an objective in the present study. However, the prevalence of BMI-based undernutrition in the present adult sample was 13.3% for men and 36.8% for women, and that of overweight was 15% for men and 11.2% for women, based on WHO (2004) criteria. Adolescents had normal BMI-for-age z-scores, based on the WHO standard (de Onis et al., Reference de Onis, Onyango, Borghi, Siyam, Nishidaa and Siekmann2007).
Although the study was cross-sectional in nature, the reported association between higher body fat and lower RSLL may be viewed in the light of evolutionary life history theory, which explains the influence of early life environmental factors like inadequate infant feeding practices, poor nutrition and infectious diseases in infancy on growth and also traces the long-term impact of these early experiences on economic and health outcomes measured in the adulthood (Kuzawa et al., Reference Kuzawa, Adair, Bechayda, Borja, Carba and Duazo2020). Cohort-based longitudinal studies provide a deep understanding of an organism’s metabolism and patterns of energy allocation to the body’s functions, growth, maintenance, reproduction and the resultant trade-offs (Adair et al., Reference Adair, Popkin, Akin, Guilkey, Gultiano and Borja2011; Kuzawa et al., Reference Kuzawa, Adair, Bechayda, Borja, Carba and Duazo2020). Human beings growing up in unfavourable environmental conditions tend to have reduced aspects of three components of biological adaptation namely, survival, productivity (e.g. somatic growth, behaviour and cognition) and reproduction (Bogin et al., Reference Bogin, Varela-Silva and Rios2007). The risks of survival due to adverse environmental conditions include fetal loss, infant mortality and child mortality. The subsequent impacts on productivity will be low birth weight, growth failure (low height-for-age or stunting) and asymmetric body proportions (e.g. short RSLL) during childhood and adolescence, and increased body fat and enhanced risk for chronic and metabolic diseases in the adulthood. Infectious disease burden, low energy intake and high energy expenditure in early life may have negative impacts on reproduction in adulthood leading to reduced fecundity and fertility (Bogin et al., Reference Bogin, Varela-Silva and Rios2007). In addition to the evidence of malnutrition and chronic infection, Social–Economic–Political–Emotional (SEPE) inequalities and insecurities are also responsible factors for growth failure among children and adolescents (Scheffler et al., Reference Scheffler, Hermanussen, Bogin, Liana, Taolin and Cempaka2019; Bogin & Varea, Reference Bogin and Varea2020).
Limbu community people live in the sub-Himalayan and Himalayan regions where micronutrient deficiencies in the soil and crops have been reported (Anderson, Reference Anderson2007; National Planning Commission of Nepal, 2013). Micronutrient deficiencies in childhood and adolescence cause impairment of growth, reduced immune competence and cognitive and developmental problems that may have associations with risks for morbidity and mortality in adulthood (Viteri & Gonzalez, Reference Viteri and Gonzalez2002; Iglesia et al., Reference Iglesia, Doets, Bel-Serrat, Román, Hermoso and Peña-Quintana2010; Cao et al., Reference Cao, Gao, Yan, Li, Su, Xu and Yan2015; Gao et al., Reference Gao, Tu, Li, Cao, Jiang and Shi2015; Bening et al., Reference Bening, Margawati and Rosidi2017; Yin et al., Reference Yin, Li, Li, Jia, Liu and Tan2017). To the best of the author’s knowledge, no previous research has been published from the Darjeeling Hills of West Bengal on micronutrient deficiencies in the soil and their negative impact on health and nutrition in children, adolescents and adults. However, Biswas et al. (Reference Biswas, Das, Chakraborty, Biswas, Sharma and Biswas2014) reported on goiter prevalence in the sub-Himalayan regions of Darjeeling district in West Bengal. Dermience et al. (Reference Dermience, Mathieu, Li, Vandevijvere, Claus and De Maertelaer2017) reported on the effects of nutrient imbalance in minerals and trace elements in Tibet, which ultimately have an impact on growth and bone metabolism leading to chronic energy deficiency and stunting in preschool children. Adverse socioeconomic conditions, unhealthy lifestyle and poor hygiene due to a shortage of water, particularly in the winter, are other factors associated with an increased risk of diseases that have been reported in the Limbu and Mech communities in Darjeeling (Bhattacharjee, Reference Bhattacharjee2015).
Other studies in the region have reported poor household socioeconomic and living conditions that were associated with poor nutritional status and growth failure in children and adolescents of the Limbu community (Bhattacharjee, Reference Bhattacharjee2015; Bhattacharjee et al., Reference Bhattacharjee, Datta Banik and Mukhopadhyay2020). Households with higher per capita monthly income and expenditure, a working mother (versus mother who is a housewife) and improved household infrastructure (construction, toilet use, water connection) had adolescent boys and girls who were taller than their counterparts with lower socioeconomic indicators. Adolescent children of working mothers were found to be taller than their peers whose mothers were housewives (Bhattacharjee et al., Reference Bhattacharjee, Datta Banik and Mukhopadhyay2020). The study also reported that the protein consumption (g/day) of Limbu adolescents was 31.0% less than the recommended dietary allowance of the Indian Council of Medical Research (ICMR, 2009). Thus, it appears that Limbu children and adolescents in the region have been suffering from chronic undernutrition since childhood and have low macronutrient consumption rates (Bhattacharjee, Reference Bhattacharjee2015). Poor household socioeconomic status, poor living conditions and an inadequate diet together had a negative impact on the growth of Limbu children and adolescents that might have a long-term impact in adulthood, resulting in short stature and low RSLL.
Human growth is highly plastic; differential growth and development patterns of body dimensions in their absolute size and relative to stature are responsive to early life environmental conditions, including nutrition and diet, disease and household psychosocial and economic status. From the perspective of developmental plasticity (Lasker, Reference Lasker1969; Bateson et al., Reference Bateson, Barker, Clutton-Brock, Deb, D’Udine and Foley2004), leg length is a marker of the quality of living conditions that determine growth in infancy, childhood and the juvenile years and carry forward a phenotype of lower RSLL into adulthood with increased risk of body fatness (Bogin, Reference Bogin1999; Bogin & Beydoun, Reference Bogin and Beydoun2007; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2010). Adverse environmental influences in early life, chronic diseases and higher energy expenditure for the maintenance at the cost of physical growth and development lead to a small size and asymmetric body proportions, which facilitate survival (Bateson et al., Reference Bateson, Barker, Clutton-Brock, Deb, D’Udine and Foley2004). The developmental programming hypothesis suggests that poor maternal nutrition during pregnancy may send a signal to the fetus of an unfavourable postnatal environment that leads to small body size at birth and may have negative impacts on health in adulthood. These issues can also be viewed in the light of the developmental origins of health and diseases (DoHAD) phenomenon as a broader biological mechanism of plasticity and epigenetics (Gluckman et al., Reference Gluckman, Hanson and Buklijas2010). Placental nutrition and lactation buffer against short-term environmental fluctuations and predictive adaptive responses ensure postnatal survival to reach reproductive age (Gluckman et al., Reference Gluckman, Hanson and Spencer2005; Wells, Reference Wells2012). The negative impact of early life experience on final body size (short stature and lower RSLL), and its association with enhanced risk for chronic diseases, body fat gain in adulthood and reduced life expectancy, can also be addressed by the ‘thrifty phenotype’ hypothesis (Hales & Barker, Reference Hales and Barker1992; Wells, Reference Wells2003, Reference Wells2011).
The study has its limitations. The outcomes of the long-term impacts of unfavourable early life environmental conditions as lower RSLL and increased risk of body fat gain among individuals cannot be addressed clearly in a cross-sectional study design like the present study. However, in the absence of other reports from the study region, the present study contributes new data to this area of research that confirm the hypothesis of an association between higher body fat and lower RSLL (Bogin & Beydoun, Reference Bogin and Beydoun2007; Bogin & Varela-Silva, Reference Bogin and Varela-Silva2008). The implementation of nutrition intervention programmes for the children from Limbu and other communities living in the Darjeeling Hills of West Bengal is recommended. Studies on the availability of micronutrients in the soil and local crops at different altitudes of the Darjeeling Hills, and the intake rates of macro- and micronutrients by different people in the community, would enhance the understanding of their association with the nutrition and health of children, adolescents and adults in the region.
In conclusion, the study indicates that relative subischial leg length (RSLL) is a reliable and cost-efficient marker, providing more nuanced information about body composition than BMI and acting as a marker for early life environmental conditions that negatively impact on body size, body proportions and enhanced health risks in the adulthood.
Acknowledgments
The study was part of a research project sponsored by the Indian Council of Medical Research (ICMR), New Delhi. The author acknowledges the help and cooperation of the study participants, Mr Bimal Kumar Sain for his assistance in fieldwork and data collection and the support extended by the authorities of Vidyasagar University in West Bengal, India. The author is also thankful to Mr John Lindsay Edwards for help with the revision of the English language.
Funding
The study was part of the research project mentioned in the Acknowledgments. No research grant was available for the publication.
Conflicts of Interest
The author has no conflicts of interest to declare.
Ethical Approval
Ethical approval was obtained from the appropriate institutional committee of Vidyasagar University, Midnapore, West Bengal, India, in connection with the research project of the Indian Council of Medical Research (ICMR), New Delhi (Sanction Memo No. 5/9/63/2008-RHN dated 23.11.2009). Permission was taken from the local government authorities and the participants gave their informed consent to share information and to participate in the anthropometric measurement sessions. Parents of the adolescents gave permission and the minors gave their verbal assent to record anthropometric measurements.


