


Anatomically corrected malposition refers to an anomaly where the arterial trunks arise from their morphologically appropriate ventricles, but exit in parallel rather than spiral fashion.Reference Van Praagh and Van Praagh1 Left juxtaposition of atrial appendages is commonly associated with this anomaly. I describe here the anatomical features of a patient with this anomaly who had a large defect in the atrial septum. The defect was closed in the catheterisation laboratory. The anatomic peculiarities delayed the diagnosis until adulthood, and offered challenges during the intervention.
Case report
A 20-year-old lady was evaluated echocardiographically because of effort intolerance and a systolic murmur. Application of the sequential segmental approach revealed usual atrial arrangement, concordant atrioventricular and ventriculoarterial connection, enlarged right-sided cardiac chambers, and a parallel arrangement of the concordantly connected arterial trunks.Reference Anderson and Ho2 The aortic valve was located anterior and to the left of the pulmonary valve, with the leaflets of both arterial valves supported by completely muscular infundibulums. The ventricular septum was intact, and the unobstructed aortic arch was right-sided. Doppler interrogation showed mild subaortic infundibular obstruction and moderate pulmonary hypertension. A transoesophageal echocardiogram revealed an abnormal position of the atrial appendages, and a large defect measuring 20 millimetres within the oval fossa (Fig. 1). The left-to-right shunt was increased by the mild subaortic infundibular obstruction. This atrial septal defect, located behind the parallel arterial trunks, was not detected easily on transthoracic echocardiogram, this contributing to the delay in her diagnosis to adulthood.
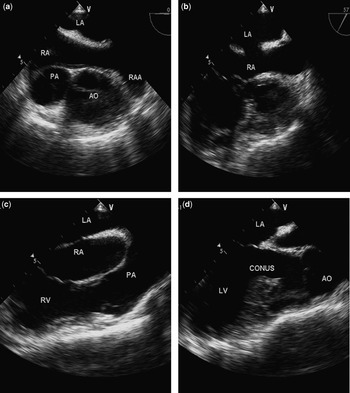
Figure 1 The transoesophageal echocardiogram (a) shows the left juxtaposition of right atrial appendage (RAA), along with the leftward and anterior location of the aorta (Ao) relative to the pulmonary trunk (PA). A modified view (b) demonstrates the atrial septal defect, while panels (c) and (d) show the right and left ventricular outflow tracts, respectively, each having the arterial valvar leaflets supported by complete muscular infundibulums. Abbreviation: RA, LA: Right and left atrium, RV, LV: Right and left ventricle.
Haemodynamic assessment showed a ratio of pulmonary to systemic flows of 3.4 to 1, moderate pulmonary arterial hypertension, and a subaortic gradient of 20 millimetres of mercury. Selective injections confirmed left juxtaposition of atrial appendages. There was a single coronary artery arising from the anterior and rightward coronary aortic sinus. (Fig. 2) Using transoesophageal echocardiographic guidance, the atrial septal defect was closed using a 22 millimetre Amplatzer septal occluder (AGA Medical, Golden Valley, MN), without balloon sizing. The location of the occluder was more leftward than usual due to the altered plane of the atrial septum, and conventional fluoroscopy and transthoracic echocardiography were entirely uninformative (Fig. 2). The enlargement of the right-sided chambers, and the pulmonary arterial pressures, were noted to be returning towards normal on follow-up echocardiogram.

Figure 2 The left ventriculogram (a) shows the left ventricle (LV) with its mildly narrowed elongated subaortic infundibulum in left anterior oblique projection, a single coronary artery from anterior right coronary sinus of aorta (Ao), and an intact ventricular septum. The right ventriculogram (b) shows the pulmonary trunk (PA) arising in parallel fashion from the right ventricle (RV), characteristic of anatomically corrected malposition. The unusual location of the device used to close the atrial septal defect (arrow) made fluoroscopic guidance uninformative.
Discussion
Anatomically corrected malposition is an unusual arrangement of the ventriculo-arterial junction in which, although the connections are concordant, the arterial trunks arise in parallel fashion, with both arterial valves supported by complete infundibulums.Reference Blume, Chung, Hoffer and Geva3 In the setting of concordant atrioventricular connections and right handed ventricular topology, the aorta originates from the morphologically left ventricle in left-sided and anterior relation to the pulmonary trunk.Reference Bernasconi, Cavalle-Garrido, Perrin and Anderson4 The combination is often associated with left juxtaposition of atrial appendages, when the broad-based and triangular right atrial appendage overlies the finger like tubular left atrial appendage.Reference Melhuish and Van Praagh5 Other associations include ventricular septal defects, subaortic obstruction, single coronary artery, and right aortic arch.Reference Bream, Elliott and Bargeron6
When the atrial appendages are juxtaposed, the plane of the atrial septum extends behind the parallel outflow tracts.Reference Melhuish and Van Praagh5 Because of this, the presence of the atrial septal defect in my patient, being positioned closer to the appendages, was not easily identified using transthoracic echocardiography. Modified transoesophageal views, however, identified the abnormal atrial appendages, delineated the unusual plane of the atrial septal defect, and guided its closure using a device inserted on a catheter. The mild subaortic obstruction had increased the left-to-right shunt, and led to moderate pulmonary arterial hypertension. My patient illustrates well all the complex associations of anatomically corrected malposition, emphasising the challenges in diagnosis, and the potential difficulties of transcatheter closure of atrial septal defects in this malformation. To the best of my knowledge, my report also represents the first documented closure of an atrial septal defect in a patient having an altered septal plane because of left juxtaposition of the atrial appendages.


