


Introduction
Self-contained underwater breathing apparatus (SCUBA) comprises a tank, mouthpiece and regulator that delivers pressurised air at the same pressure as the aquatic depth attained.Reference Reuter, Paparella, Shumrick, Gluckman and Meyerhoff1 This apparatus was developed in 1943 by Cousteau and Gagnan.Reference Edmonds, Lowry and Pennefather2 As a result of rapid technological development and growing economical facilities, there are now more than 28 million registered divers worldwide.3
Several laws and principles affect human physiology underwater. The most important one is Boyle's law, which states that the volume of a gas varies inversely with the pressure.Reference Edmonds, Lowry and Pennefather2 For example, at a depth of 10 m, the pressure is 2 atmosphere (ATA) and the volume of a gas will be compressed by half. If pressure equalisation is insufficient, air-containing spaces, such as the paranasal sinuses and middle ear, can be damaged; this is termed barotrauma.Reference Edmonds, Lowry and Pennefather2, Reference Neblett4
The most common diving-related problem among sports SCUBA divers is middle-ear barotrauma, followed by paranasal sinus barotrauma.Reference Reuter, Paparella, Shumrick, Gluckman and Meyerhoff1, Reference Neblett4–Reference Roydhouse6 Uzun et al. have found that the incidence of paranasal sinus barotrauma in sports SCUBA divers is 27 per cent per diver and 0.5 per cent per dive.Reference Uzun, Tas, Yagiz, Cicek and Inan5 Although paranasal sinus barotrauma is the second most common complication of sports SCUBA diving,Reference Neblett4, Reference Uzun, Tas, Yagiz, Cicek and Inan5 there is little published research on this subject. In the English literature, the author could find only two research articles (one of limited content) and one cited reference, regarding paranasal sinus barotrauma in divers.Reference Edmonds, Lowry and Pennefather2, Reference Roydhouse6, Reference Fagan, McKenzie and Edmonds7
The common predisposing factors for paranasal sinus barotrauma are upper respiratory tract infection, nasosinusal pathology, forceful Valsalva's manoeuvre and inappropriate diving techniques.Reference Reuter, Paparella, Shumrick, Gluckman and Meyerhoff1, Reference Edmonds, Lowry and Pennefather2, Reference Neblett4–Reference Becker and Parell8 However, it is not known whether there are any other factors which may influence the occurrence of paranasal sinus barotrauma in divers with no symptoms or signs of rhino-sinus disease on routine pre-dive examination.
Thus, the current study evaluated several parameters in relation to paranasal sinus barotrauma in sports SCUBA divers with normal findings on routine pre-dive examination.
Material and methods
From an initial group of 49 sports SCUBA divers, this study analysed pre-dive and follow-up records for 46 divers (11 female, 35 male; median age 25 years, age range 14–38 years) who had no prior contraindications to diving, according to a standard pre-dive examination used for sports SCUBA diving candidates.Reference Bove9 Three divers were excluded as a result of the pre-dive examination, two due to rhinosinusitis and one due to allergic rhinitis. In the routine pre-dive examination of the remaining 46 diving candidates who did not have any symptoms of acute or chronic rhino-sinus disease, anterior and posterior rhinoscopy, sinus radiography (Caldwell and Waters positions) and nasal endoscopy (performed in subjects with a previous history of rhino-sinus disease) showed no sign of rhinitis and/or sinusitis. These subjects' nasal fossae, middle meati and spheno-ethmoidal recesses were free of disease. Subjects with mild nasal septum deviation which did not cause any symptoms or total obstruction on one side were not excluded.
Each SCUBA dive lasted approximately 20 to 30 minutes at a mean depth of 18 m in open salt water (range, 2–61 m). All divers were trained by the same trainer and completed the same diving programme, according to the Confédération Mondiale des Activités Subaquatiques (World Underwater Federation) international diver certificate system. The SCUBA tanks contained pressurised atmospheric air. None of the divers had undertaken air flight or high attitude travel in the two days before their dive.
Pressure equalisation techniques were explained to each diver individually. To equalise the middle ear and paranasal sinus pressure, divers used the Valsalva and Frenzel manoeuvres on descent and the Toynbee manoeuvre on ascent.
Divers were instructed to inform the investigator if any symptom was experienced during diving. The dive trainer interviewed all divers after each dive and informed the investigator in the event of any diving-related symptom.
During a dive, if the diver experienced acute, severe frontal or facial pain, with or without epistaxis, due to an inability to equalise the pressure difference between the sinuses and the ambient pressure, this was defined as paranasal sinus barotrauma.Reference Edmonds, Lowry and Pennefather2, Reference Uzun, Tas, Yagiz, Cicek and Inan5, Reference Fagan, McKenzie and Edmonds7, Reference Becker and Parell8 As it is not usually indicated for the routine management of paranasal sinus barotrauma,Reference Edmonds, Lowry and Pennefather2 radiography was not performed in divers with barotrauma symptoms unless symptoms persisted. Any barotrauma which occurred during an upper respiratory tract infection was excluded.
The following parameters were evaluated and compared for divers with and without paranasal sinus barotrauma: sex, alcohol consumption, smoking, use of decongestants (pseudoephedrine with or without nasal sprays), mild nasal septal deviation, sinusitis history (including allergic rhinitis), inability to perform Valsalva manoeuvre, inability to perform Toynbee manoeuvre, and middle-ear barotrauma history.
Statistical analysis was carried out using the chi-square test and Fisher's exact test. A p value below 0.05 was considered statistically significant.
The Trakya University Faculty of Medicine institutional ethics committee approved the study.
Results and analysis
The divers completed a total of 1217 dives (median, 15; range, three to 100). Paranasal sinus barotrauma occurred in 12 divers (26.1 per cent) during 13 dives (1.1 per cent) over the observation period; all episodes resolved without sequelae. A decongestant was usually the only treating drug. Antibiotics were used in one diver whose symptoms persisted for more than 24 hours. In this subject, a sinus computed tomography (CT) scan revealed a fluid level in the right maxillary sinus and full opacity in the left maxillary sinus (Figure 1). This diver was forbidden from diving until one and a half months after the symptoms had recovered.
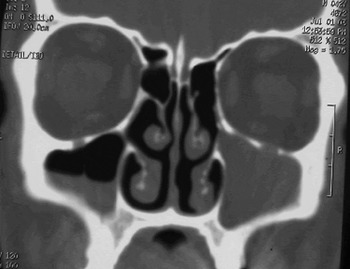
Fig. 1 Coronal sinus computed tomography scan of a diver with severe paranasal sinus barotrauma, showing a fluid level in the right maxillary sinus and opacity of the left maxillary sinus.
The main symptoms reported were frontal or facial headache, experienced by all affected divers, and epistaxis, experienced by four divers. Six of the affected divers reported that their symptoms had begun during descent, and three during ascent; three divers did not know at which diving phase their symptoms had begun.
Among the evaluated parameters, a history of sinusitis and of middle-ear barotrauma was significantly more frequent in barotrauma group divers than in non-barotrauma group divers (Table I). Although the barotrauma group had higher rates of smoking, decongestant use, mild septal deviation and inability to perform the Valsalva manoeuvre, compared with the non-barotrauma group, these differences were not statistically significant (Table 1).
Table I Pre-dive parameters in paranasal sinus barotrauma vs non-barotrauma groups

* n = 12; †n = 34. ‡Chi-square, Fisher exact test, p < 0.05. F = female; M = male
Discussion
Paranasal sinus barotrauma occurs because the relatively rigid walls of the sinus cavity cannot expand or contract in response to the pressure changes experienced during diving, in accordance with Boyle's Law. Normally, the paranasal sinuses are air-filled cavities and communicate with the nasal cavity through their ostia.Reference Garges10 Paranasal sinus barotrauma of descent, also termed ‘sinus squeeze’, occurs during the diving descent if a sinus ostium is blocked. This results in a negative pressure in the sinus cavity, which elicits mucosal congestion, oedema and haemorrhage within the sinus cavity, accompanied by immediate pain. As the sinus cavity fills with oedema fluid and blood, the main symptom of paranasal sinus barotraumas – the sharp, intense pain (due to a vacuum in the sinuses) – is relieved.Reference Becker and Parell8 During ascent to the surface, mild epistaxis (the second commonest symptom of paranasal sinus barotrauma) may occur when expansion of the enclosed air expels blood and mucus from the sinus ostium.Reference Reuter, Paparella, Shumrick, Gluckman and Meyerhoff1, Reference Edmonds, Lowry and Pennefather2, Reference Fagan, McKenzie and Edmonds7, Reference Becker and Parell8 As it was supported by the present study, paranasal sinus barotrauma of descent may be seen two times more than the paranasal sinus barotrauma of ascent.
Paranasal sinus barotrauma of ascent, also termed ‘reverse sinus squeeze’, occurs when a sinus ostium becomes occluded at depth, thus preventing escape of expanding gases during diving ascent.Reference Edmonds, Lowry and Pennefather2 Epistaxis may sometimes be the sole symptom.Reference Fagan, McKenzie and Edmonds7 However, rarely, prevention of expanding gases in the sinus may fracture the sinus walls or force gas into an already existing fracture, which can cause subcutaneous emphysema.Reference Edmonds, Lowry and Pennefather2, Reference Garges10 Occasionally, air may rupture into the cranial cavity and cause pneumocephalus.Reference Becker and Parell8, Reference Goldmann11, Reference Tryggvason, Briem, Guomundsson and Einarsdottir12 Although unusual, blindness, meningitis and trigeminal nerve dysfunction have also been reported due to sinus barotrauma.Reference Becker and Parell8, Reference Buisson, Darsonval and Dubin13, Reference Murrison, Smith, Francis and Counter14
Severe frontal headache was the dominant presenting symptom in all cases in the present study. If pain is experienced in other parts of the face, especially along the upper jaw, it should be verified as being of sinus aetiology; what initially appears to be paranasal sinus barotrauma may actually be referred tooth pain.Reference Garges10
Cerebral decompression sickness is one of the most important and dangerous complications of diving, and it should be considered in the differential diagnosis in serious cases of paranasal sinus barotrauma with complicating sinus infection, in which severe headache may persist for some hours after the dive. If there is any doubt, there should be no hesitation in administering hyperbaric oxygen therapy.Reference Edmonds, Lowry and Pennefather2
Although severe frontal headache is the dominant symptom, the maxillary sinus is the most commonly affected sinus, according to radiological sinus examination of divers with paranasal sinus barotrauma.Reference Fagan, McKenzie and Edmonds7 In their study on paranasal sinus barotrauma in divers, Fagan et al. found that 79 per cent of divers with the condition who were examined radiologically showed sinus anomalies on plain sinus X-rays. While most cases showed only mucosal thickening, a small number had a fluid level or gross mucosal thickening causing total or near-total sinus opacity.Reference Fagan, McKenzie and Edmonds7 However, Fagan et al. did not perform baseline radiological examination of the divers at the beginning of their study, and thus the abnormal radiological findings found after diving (e.g. mucosal thickening) might have existed previously (perhaps related to previous sinus disease or to the subject's diving experience).
Yanagawa et al., in their study on magnetic resonance imaging of divers' paranasal sinuses, found that divers tended to have paranasal sinus mucosal hypertrophy.Reference Yanagawa, Okada, Ishida, Fukuda, Hirata and Fujita15 In addition; these authors found that X-ray examination of the paranasal sinuses may not always give reliable information and may sometimes mislead the examiner.
Because of its long drainage pathway through the fronto-ethmoidal recess and the lack of accessory ostia, the frontal sinus could be expected to be the most frequently involved sinus in paranasal sinus barotrauma. This theory is in accordance with the dominant symptom of pain over the frontal sinuses. Moreover, in contrast to the present study, Roydhouse found that the frontal sinuses were involved more frequently than the maxillary sinuses among SCUBA divers with ‘sinus squeeze’.Reference Roydhouse6 Further study, including paranasal sinus computed tomography (CT) or magnetic resonance imaging scanning both at baseline and after paranasal sinus barotrauma development, may be useful to establish which sinus is the most frequently involved in paranasal sinus barotrauma of divers.
According to Edmonds (a major author in the field), radiographs and scans are not indicated for the routine clinical management of sinus barotrauma, as they do not substantially influence the course of treatment.Reference Edmonds, Lowry and Pennefather2 Thus, in the present study, radiography was not performed in those divers with paranasal sinus barotrauma symptoms. However, paranasal sinus and cranial CT scanning was needed in one subject (Figure 1) because of persistent post-dive facial pain and headache.
The management of barotrauma includes prevention.Reference Reuter, Paparella, Shumrick, Gluckman and Meyerhoff1 The most important precautions for the prevention of paranasal sinus barotrauma in divers are: avoidance of diving during bouts of upper respiratory infection, sinusitis or rhinitis;Reference Edmonds, Lowry and Pennefather2 use of positive pressure techniques such as the Valsalva manoeuvre, beginning immediately prior to descent and then at regular intervals of 0.5–1 m during descent;3 feet-first descent;Reference Neblett4 and slow descents and ascents.Reference Edmonds, Lowry and Pennefather2, Reference Uzun, Tas, Yagiz, Cicek and Inan5 Upper respiratory infections, naso-sinusal pathology (such as significant nasal septum deviation, nasal congestion due to nasal polyps, chronic sinusitis and uncontrolled allergic rhinitis), and forceful Valsalva manoeuvre are well known to affect the ventilation of both the paranasal sinuses and the middle-ear spaces during periods of rapid pressure change.Reference Reuter, Paparella, Shumrick, Gluckman and Meyerhoff1, Reference Edmonds, Lowry and Pennefather2, Reference Neblett4–Reference Becker and Parell8, Reference Uzun16 Such disorders can be evaluated by a careful pre-dive otorhinolaryngological examination and subsequently treated. None of the divers in the present study had any of these conditions (as the study inclusion criteria specified normal routine pre-dive and otolaryngological examinations, without any signs of nasal or sinusal disease).
• Nasal and paranasal sinus disorders are well known factors facilitating the occurrence of sinus barotrauma in affected divers
• The present study evaluated predisposing factors for sinus barotrauma in healthy divers with normal findings on a routine pre-dive examination
• Healthy divers with a history of sinusitis or middle-ear barotrauma appeared to be more prone to sinus barotrauma
• A more detailed pre-dive examination for such divers is suggested
The present study found that paranasal sinus barotrauma was experienced more commonly by divers with a history of sinusitis or of middle-ear barotrauma (Table I). These results may be related to the diver's difficulty in equalising the pressure differential in air-containing spaces such as the paranasal sinuses or middle ear when there is marginal patency of the sinus ostia or eustachian tube. In addition, these findings may suggest that divers with a history of sinusitis may have predisposing factors for ostial insufficiency which could not be detected during routine nasal and sinus examination (e.g. mucosal lesions in the middle meatus, hindering ostial patency), increasing the risk of paranasal sinus barotrauma. Fagan et al. found that 50 per cent of divers with paranasal sinus barotrauma gave a history of intermittent or long term symptoms referable to the upper respiratory tract or to nasal or sinusal disorders.Reference Fagan, McKenzie and Edmonds7 In such circumstances, a paranasal sinus CT scan may be useful in order to detect possible predisposing anatomopathological conditions. Use of CT scanning may also enable investigation of any correlation between sinus ostia size and barotrauma occurrence. However, the present study did not have such data available, as the standard protocol of the pre-dive examination did not include paranasal sinus CT scanning.
Most cases of paranasal sinus barotrauma require no treatment, or only a decongestant. Occasionally, antibiotics are needed.Reference Fagan, McKenzie and Edmonds7 In the present study, antibiotics were used in only one case, a diver whose symptoms persisted for more than 24 hours. This diver was not allowed to dive until one and a half months after the symptoms had resolved. Surgical drainage is rarely indicated. In intractable and recurrent cases, endoscopic sinus surgery may be useful to widen the sinus ostia, preventing paranasal sinus barotrauma.Reference Edmonds, Lowry and Pennefather2 However, endoscopic sinus surgery may not necessarily obviate the risk of serious neurological sequelae.Reference Parell and Becker17 In such divers, a pressure test should be conducted in a hyperbaric chamber or, more practically, in a 5 m or deeper swimming pool, if no clinical and radiological evidence of ostial insufficiency persists after sinus surgery. Diving may be resumed if no pain develops during the pressure test. However, these divers must be warned of the relevant risks and should use nonforceful techniques of clearing the sinuses during diving.Reference Parell and Becker17
Conclusion
Paranasal sinus barotrauma is a common disorder in sports SCUBA divers, and can occur even in divers with normal routine pre-dive and otolaryngological examinations. In sports SCUBA divers, paranasal sinus barotrauma is usually self-limiting and resolves without sequelae. However, rarely, serious complications can ensue. In divers with a normal routine pre-dive examination, the occurrence of paranasal sinus barotrauma does not appear to be related to sex, alcohol consumption, smoking, decongestant use, mild nasal septal deviation or inability to perform the Valsalva or Toynbee manoeuvres. However, divers with a history of sinusitis, allergic rhinitis or middle-ear barotrauma may be more prone to paranasal sinus barotrauma, compared with divers without such a history. Such divers should take rigorous precautions against the development of paranasal sinus barotrauma. Diving candidates with a previous history of sinusitis, allergic rhinitis or middle-ear barotrauma may be better examined using paranasal sinus CT scanning, instead of the routine pre-dive nasal and sinus examination. However, further studies are needed to evaluate this assumption.
Acknowledgements
The author thanks Tamer Yorukoglu, Diving Trainer, Argos diving center, Edirne, Turkey, for his great assistance, and Prof Ibrahim Hizalan, MD, Department of Otorhinolaryngology, Uludag University Faculty of Medicine, Bursa, Turkey, for his advice on the preparation of the manuscript.


