



1. Introduction
Natural disasters have become increasingly prevalent and destructive in recent decades. Globally, natural disasters occur almost five times as frequently as they did 40 years ago (UNICEF, 2015a). The groups most vulnerable to these consequences of climate change are the poor and the young (Philipsborn and Chan, Reference Philipsborn and Chan2018). The poor often lack the ability to cope with disasters while children are vulnerable along multiple dimensions: nutrition, injury, drinking water and sanitation (Favor, Reference Favor2011: 24). Not only are the immediate effects of natural disasters large but their effects persist in children since early-life anthropometric deficiencies frequently last into adulthood (Almond and Currie, Reference Almond and Currie2011). These effects are often concentrated in poor children since their households are usually the most exposed and they lack the ability to respond.
Although the effects of a variety of shocks have been established, as pioneered by Maccini and Yang (Reference Maccini and Yang2009), one shortcoming in the literature is that these focus on individual shocks. However, children in developing countries are frequently exposed to multiple shocks within a given year (World Bank, 2014). Since households have limited means to address shocks, multiple shocks within a short period are particularly harmful and their effects may not necessarily be additive in the presence of the liquidity constraints that often exist in developing countries (Deaton, Reference Deaton1991).
This study examines the medium-term effects of exposure to a multitude of shocks on anthropometric outcomes. In doing so, we examine two interrelated questions. Firstly, are the effects of exposure to natural disasters persistent and do they vary across gender? Secondly, does access to credit or remittances make households more resilient to shocks? Whereas previous studies have identified which investments help with particular shocks, less is understood about what helps across a variety of shocks. Not only does access to credit help to resolve the liquidity constraints that are particularly destructive (Deaton, Reference Deaton1991), but it is also a policy instrument that is frequently used.
We studied Indonesia due to its prevalence of natural disasters. It is located on an actively moving tectonic plate and the subductionFootnote 1 of the Indian Oceanic plate against the Eurasia Continental plate makes it vulnerable to earthquakes, tsunamis and volcanic activity. According to The Indonesian National Agency for Disaster Management, from 2002 to 2012 there were 12,494 disasters resulting in 190,087 casualties (Kusumastuti et al., Reference Kusumastuti, Viverita, Suardi and Danarsari2014). The Indonesian context has previously been studied. For instance, Gignoux and Menéndez (Reference Gignoux and Menéndez2016) quantify the effect of earthquakes on welfare dynamics in the aftermath. They show that households might be able to recover physical capital in the wake of disasters. Based on an asset/income metric, they find no long-term adverse effects. However, evidence shows that natural disasters affect wellbeing more than asset losses (Hallegatte et al., Reference Hallegatte, Vogt-Schilb, Bangalore and Rozenberg2016). Our study is based on this premise. We used the Indonesia Family Life Survey (IFLS) to construct a sample of children between ages 0 (in-utero) to 12 years on Java Island (for reasons detailed in section 3) and measure the prevalence of stunting. Our results reveal that girls exposed to multiple types of disasters are shorter by 0.19 standard deviations and are 7 per cent more likely to be stunted. We find no persistent effect on boys.
These results extend the literature in three ways. Firstly, we provide empirical evidence on the effects of exposure to a series of disaster events in a literature where most studies focus on an individual shock (e.g., Foster, Reference Foster1995; Hoddinott et al., Reference Hoddinott, Alderman, Behrman, Haddad and Horton2013; Caruso and Miller, Reference Caruso and Miller2015; Fujiki and Hsiao, Reference Fujiki and Hsiao2015). Secondly, most studies tend to investigate effects in the immediate aftermath (e.g., Block et al., Reference Block, Keiss, Webb, Kosen, Moench-Pfanner, Bloem and Timmer2003; Datar et al., Reference Datar, Liu, Linnemayr and Stecher2013; Brunson, Reference Brunson2017; Nguyen et al., Reference Nguyen, Nguyen and Grote2020). Our focus is on the persistence of these initial effects. We find that girls in Indonesia are worse off since the growth retardation persists in the medium-term. Lastly, we find suggestive evidence that even in the presence of access to credit or remittances the exposure effect does not mitigate. In places like Indonesia which are prone to multiple disasters simultaneously, policymaking is not always disaster specific (Kusumastuti et al., Reference Kusumastuti, Viverita, Suardi and Danarsari2014; Bakkour et al., Reference Bakkour, Enjolras, Thouret, Kast, Tyas, Mei and Prihatminingtyas2015). We highlight the need for establishing coping mechanisms beyond access to credit in recovering post-disasters.
The remainder of the paper is organized as follows. Section 2 justifies our focus on Indonesia, while section 3 provides the data and empirical methodology. The results are discussed in section 4 and section 5 concludes.
2. Why Indonesia?
In this section we elaborate on the reasons for choosing Indonesia as a canvas for studying links between child health and natural disasters. Firstly, the prevalence of natural disasters renders Indonesia a viable case study. The International Disaster Database EM-DAT records 98 natural disasters (out of which 90 occurred in the IFLS regions) during our study period of 2002 to 2007. The recorded human loss is 177,153 while total damages amount to US$9 billion (EM-DAT, 2018). Apart from the destruction, these events also lead to other outcomes such as air pollution that affect child wellbeing. For instance, Jayachandran (Reference Jayachandran2009) examined the air pollution from forest fires in 1997 and found that prenatal exposure resulted in 16,400 fewer surviving children.
Secondly, Indonesia has the third highest youth population in the world, making it a relevant context for studying child health. The county is home to 72 million of the world's 2.3 billion children aged 0 to 14 years (UNICEF, 2015b). Childhood exposure could result in stunted growth. especially during the first two years when children grow faster than any other time of life (Almond and Currie, Reference Almond and Currie2011). Hence child health is at the forefront of the country's agenda and therein lies our third reason: Indonesia is a classic example of why economic growth is not sufficient for improving child health (Trisnantoro et al., Reference Trisnantoro, Soemantri, Singgih, Pritasari, Mulati, Agung and Weber2010). Despite maintaining a consistent economic growth of three to five per cent in the past 20 years, Indonesia still accounts for two per cent of the world's under five mortality rate (UNICEF, 2015a). Part of the problem lies in health care access. The 1998 Asian Financial Crisis replaced the authoritarian regime with a democratic system, thereby placing 500 districts (in 33 provinces) in charge of delivering their own health interventions in lieu of the centralized system. While Indonesia has improved child health standards – in 2015 the country recorded only 27 deaths per 1,000 live births compared to 85 deaths per 1,000 live births in 1990 – the need for health interventions is still prevalent (Trisnantoro et al., Reference Trisnantoro, Soemantri, Singgih, Pritasari, Mulati, Agung and Weber2010). Natural disasters lead to destruction of health facilities thereby exacerbating the vulnerability of children and the elderly. Hence, Indonesia indeed constitutes a viable case study for us to explore using the data and methods detailed in the next section.
3. Data, empirical methodology, and econometric issues
3.1 Indonesia family life survey
Our data is from the IFLS, a nationally representative panel dataset, implemented by the RAND Corporation and the Demographic Institute at the University of Indonesia. The first round of the survey (hereafter IFLS1) – fielded in 1993 – covered approximately 7,224 households in 13 out of 27 provinces representing 83 per cent of the Indonesian population. The most recent round of the survey, IFLS5, took place in 2014 (i.e., 21 years after the IFLS1). The re-contact rate between the first and the fifth wave is 92 per cent. In our analysis, we use information from IFLS waves 2, 3, 4 and 5, which were collected in 1997, 2000, 2007 and 2014 respectively.
3.2 Model
The study analyzes the effect on child health outcomes of being exposed to different types of natural disasters. Thus, for child $i$ residing in community c in municipality (kabupaten) k during round t, we estimate the following model:
residing in community c in municipality (kabupaten) k during round t, we estimate the following model:

The child health outcomes are denoted by $\textrm{CH}.$
We capture the human capital accumulation in children through two methods. Firstly, we use the height-for-age Z score (HAZ) based on child height collected by an anthropometrist.Footnote 2 Child height encompasses all health events since birth and is a ubiquitous metric of long-run child stature employed in the economics and nutrition literatures (Block et al., Reference Block, Keiss, Webb, Kosen, Moench-Pfanner, Bloem and Timmer2003; Maccini and Yang, Reference Maccini and Yang2009; Dataret al., Reference Datar, Liu, Linnemayr and Stecher2013; Cornwell and Inder, Reference Cornwell and Inder2015). Child height is also strongly correlated with adult height which is used as a metric of population health (Fogel, Reference Fogel1994) as well as productivity, wages and long-run growth (Strauss and Thomas, Reference Strauss and Thomas1998). Secondly, we use an indicator for stunting which is set to one if HAZ is two standard deviations below the reference group mean and zero otherwise. Stunting is a widely regarded measure of nutritional status and physical health stock (Adair and Guilkey, Reference Adair and Guilkey1997; Hoddinott et al., Reference Hoddinott, Alderman, Behrman, Haddad and Horton2013; Giles and Satriawan, Reference Giles and Satriawan2015). Both these outcomes – measured using IFLS5 from 2014 (t = 1) – help us assess the persistence of the effects in the medium term.
This is important for three reasons. Firstly, it is well-known that parents try to mitigate the effect of disasters in children through investments in them. Since parental responses are endogenous, it is typically hard to identify if they invest in the children who are most likely to survive – thereby increasing cross-sibling inequality – or take remedial action for the benefit of all children (Berry et al., Reference Berry, Dizon-Ross and Jagnani2019). Secondly, the initial effect may dissipate over time due to catching up under the right conditions as shown in Filipino children (Adair, Reference Adair1999) and Bolivian children (Godoy et al., Reference Godoy, Nyberg, Eisenberg, Magvanjav, Shinnar, Leonard, Gravlee, Reyes-Garcia, Mcdade, Huanca and Tanner2010). Thus the outcomes of these investments are difficult to measure in the short run. The third reason is that disaster relief aid is not instantaneous. Typically humanitarian response takes about eight months to materialize (World Bank, 2014: 104). Thus it is important to investigate the persistence of the initial disaster effect after parents have had time to respond and aid programs have started to kick in as well. We are able to uncover the effects lasting 7 to 12 years after the disasters have occurred owing to continuous data collection of the IFLS panel.
3.2.1 Defining exposure and the sample
The final sample is comprised of all the children on Java Island aged 0 (in-utero) to 12 at the time of IFLS4 in 2007 (n = 1,262). These children are from 998 households that reside in 168 communities. There are 634 boys and 628 girls. We restrict the sample to Java Island for two reasons. Firstly, it reflects the proximity to the epicenter of the most disastrous natural disaster in the IFLS provinces during our study period – the Yogyakarta earthquake (EM-DAT, 2018).Footnote 3 Given the geography of Indonesia, including all the children is likely to bias the results downward as those regions are less likely to have: (a) experienced this natural disaster; and (b) dealt with any repercussions in the aftermath. This earthquake also spawned a series of public policy changes with respect to disaster management in order to mitigate the risks and accelerate the rehabilitation efforts (Pujiono, Reference Pujiono, Karnawati, Pramumijoyo, Anderson and Husein2008). Given that the government response to these types of disasters is endogenous, restricting our sample to Java Island also allows us to limit time-varying regional heterogeneity that may affect children's health.
Apart from the household survey, all the IFLS waves include a community facility survey where the community (village) leaders were interviewed about, among other things, the history and climate of the community over the last five years. Using the IFLS4 (2007) community survey, we determined the communities that were exposed to any natural disaster between 2002 and 2007. The different types of natural disasters in this study include floods, earthquakes, landslides, volcano eruptions, tsunamis, droughts and forest fires. Table 1 lists the number of events that IFLS communities encountered within each disaster category.
Table 1. Recorded number of events and exposure levels on Java Island, 2002–2007

Source: IFLS wave 4.
In the effective sample, 50 per cent of the children experienced at least one type of natural disaster. Out of this, 35 per cent were exposed to exactly one disaster type. The total types of disasters to which children were exposed range from 0 to 5, however, only four per cent encountered more than three disasters types. The children were most exposed to floods followed by earthquakes, while the other types were relatively smaller in frequency. The most damage was recorded from earthquakes (US$8.374 billion) and floods (US$1.489 billion) (EM-DAT, 2018). The Indian Ocean Tsunami that occurred on 26 December 2004 is the largest natural disaster Indonesia has experienced to date. None of the IFLS communities record being exposed, which is not surprising since the province hardest hit – Aceh – was not historically part of the IFLS panel due to political tensions (Frankenberg and Karoly, Reference Frankenberg and Karoly1995). Only one community indicates exposure to a tsunami (in 2007) that affected seven children. We performed analysis without this community and our results remain robust as shown in online appendix table A2. Using the information in table 1, we formed two different ways of capturing the severity of disaster exposure: based on disaster type and reported damage.
We computed the number of different types of disasters each community (child) experienced following recent literature (Datar et al., Reference Datar, Liu, Linnemayr and Stecher2013; Maclean et al., Reference Maclean, Popovici and French2016; Caruso, Reference Caruso2017). Children in communities that did not experience any type of disasters have an imputed value of zero. Our approach is consistent in the context of serial correlation among events (e.g., floods leading to landslides) for which it would prove difficult to separately identify individual effects (Datar et al., Reference Datar, Liu, Linnemayr and Stecher2013). The implicit assumption is that a community that goes through a multitude of disaster categories is worse off than if it were exposed to one disaster category.
There are potentially two issues with this implicit assumption. It could be argued that a community, albeit experiencing only few floods, might have experienced more serious floods (in terms of the damage caused) than another community that went through multiple disaster types. Another problem is that natural disasters are covariate shocks – correlated across households within communities (Günther and Harttgen, Reference Günther and Harttgen2009). Since the sample size is not sufficiently large to detect an effect, a more robust measure would be to use the reported damage. IFLS records the reported economic and human loss caused by natural disasters. Fortunately the number of households that lost a family member is minimal (18 households). Therefore we resort to capturing the economic (asset) loss that affected 734 households. We then create a binary exposure variable with a value of one if the household recorded economic loss due to any type of natural disaster. Zero is imputed for households that either did not experience any disasters or did not endure economic loss. According to table 2, nine per cent of the children are from a household with reported economic loss.
Table 2. Descriptive statistics with the corresponding IFLS rounds (in parentheses)
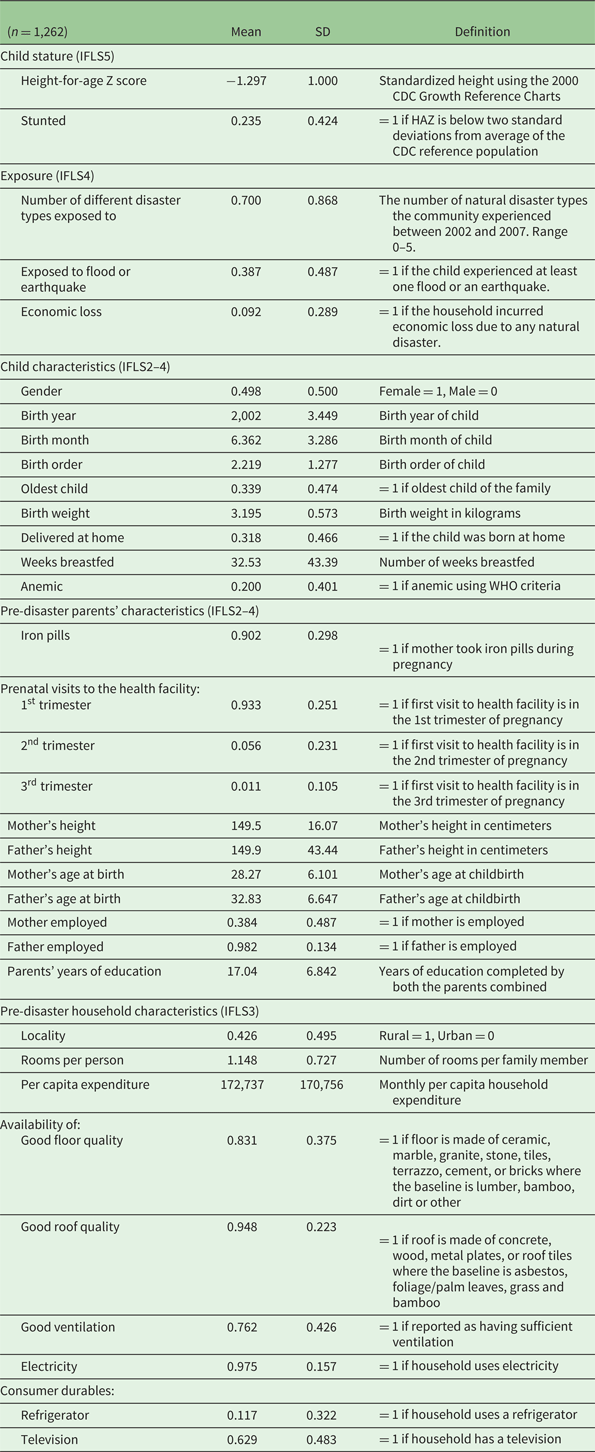
Note: The descriptive statistics for the effective sample using fixed effect model of equation (1).
Source: IFLS panel. Sample: Children on Java Island aged 0–12 in 2007.
3.2.2 Control variables and selective migration
In equation (1), ${X_{it - 1}}\;$ is a vector of ex-ante child characteristics: gender, birth order, an indicator for being the oldest child, and information specific to his/her childhood (e.g., birth weight, duration breastfed, and location of the birth). ${X_{\textrm{pht} - 1}}$
is a vector of ex-ante child characteristics: gender, birth order, an indicator for being the oldest child, and information specific to his/her childhood (e.g., birth weight, duration breastfed, and location of the birth). ${X_{\textrm{pht} - 1}}$ is a vector of the parent and household characteristics listed in table 2, measured before the natural disasters (t = −1) to avoid endogeneity. We further include fixed effects, $fe$
is a vector of the parent and household characteristics listed in table 2, measured before the natural disasters (t = −1) to avoid endogeneity. We further include fixed effects, $fe$ , based on the birth cohort (year and month of birth). Since culture and religious practices could also affect a child's nutrition and health, we use religion dummies. For households that moved between IFLS3 and IFLS4 we employ the intent to treat (ITT) methodology to account for selective migration. Following a natural disaster, families could relocate altogether and/or pregnant mothers could opt to raise children in ‘safer’ locations that are less disaster prone and may not necessarily be part of the sampling regions. The ITT approach corrects for the potential selection by assigning migrant households back to their pre-disaster community. Assuming the natural disasters are not perfectly predictable, ITT would then allow the sample to be treated as randomized irrespective of the actual location after the shock (Almond and Mazumder, Reference Almond and Mazumder2011). The idiosyncratic error term ${\varepsilon_{it}}$
, based on the birth cohort (year and month of birth). Since culture and religious practices could also affect a child's nutrition and health, we use religion dummies. For households that moved between IFLS3 and IFLS4 we employ the intent to treat (ITT) methodology to account for selective migration. Following a natural disaster, families could relocate altogether and/or pregnant mothers could opt to raise children in ‘safer’ locations that are less disaster prone and may not necessarily be part of the sampling regions. The ITT approach corrects for the potential selection by assigning migrant households back to their pre-disaster community. Assuming the natural disasters are not perfectly predictable, ITT would then allow the sample to be treated as randomized irrespective of the actual location after the shock (Almond and Mazumder, Reference Almond and Mazumder2011). The idiosyncratic error term ${\varepsilon_{it}}$ is expected to be independent. We estimate equation (1) using the ordinary least squares methodFootnote 4 and cluster the standard errors at the community level based on the survey sampling design (Abadie et al., Reference Abadie, Athley, Imbens and Wooldridge2017).Footnote 5
is expected to be independent. We estimate equation (1) using the ordinary least squares methodFootnote 4 and cluster the standard errors at the community level based on the survey sampling design (Abadie et al., Reference Abadie, Athley, Imbens and Wooldridge2017).Footnote 5
3.3 Summary statistics
Based on table 2, the average child in the sample is about one standard deviation shorter than the CDC reference group and approximately 23 per cent are stunted. This is consistent with similar studies in the literature (Cornwell and Inder, Reference Cornwell and Inder2015). At the time of IFLS4, the average child was 5 years old and was the second child in the family. Since birth histories are recorded only for children under the age of 5 (Frankenberg and Karoly, Reference Frankenberg and Karoly1995: 13), we use the IFLS wave immediately after the child's birth year to collect the information on the birth weight, birth delivery location, and nutrition in early childhood (number of weeks breastfed).Footnote 6 About 31 per cent of the children were born at home, weighed approximately 3 kilograms and breastfed, on average, for 32 weeks.
Since we focus on human development, it is necessary to account for possible micronutrient deficiencies. As noted in the literature (e.g., Orazem and King, Reference Orazem, King, Schultz and Strauss2007; Strauss and Thomas, Reference Strauss, Thomas, Schultz and Strauss2007), iodine deficiency and anemia (caused by low iron intake) can lead to adverse birth outcomes, increased susceptibility to disease, and reduced cognitive development. We define the likelihood of being anemic using World Health Organization (WHO) thresholds since their hemoglobin cutoff points are valid for the Indonesian population (Khusun et al., Reference Khusun, Yip, Schultink and Dillon1999). Approximately 20 per cent of the children in the sample are anemic.
Next we turn to pre-disaster parental characteristics. As before, the information pertaining to childbirth (e.g., prenatal visits and taking iron pills) was derived from the IFLS waves closest to the child's birth year. About 90 per cent of the mothers took iron pills while pregnant and about 93 per cent reported pre-natal visit to the health facility during the first trimester of the pregnancy (table 2). Two potential issues in a study like this are the endogeneity of birth timing (i.e., parents choosing to have children during months with favorable weather conditions) and genetics. Given the impossibility of predicting natural disasters – particularly when the study employs a multitude of events non-discriminately – the endogeneity of birth timing becomes less relevant. As for genetics, Cornwell and Inder (Reference Cornwell and Inder2015) find that the low stature in Indonesian children cannot be attributed purely to genetics and is more likely to be caused by a range of environmental factors. Bearing this in mind, we include each parent's height (measured in centimeters) to account for intergenerational transmission of health. Based on table 2, the average parent is about 150 cm tall. Furthermore, we control for each parent's age at the time of the child's birth, years of education (combined for both parents), and whether the parents were employed, since these factors are likely to contribute to child rearing practices. The average mother (father) is approximately 28 (33) years old at the time of the child's birth. While 98 per cent of the fathers are employed, only 38 per cent of the mothers hold a job at the time of the child's birth and the average household has about 17 combined years of schooling.
Since the child's health could be related to his/her location, we include a host of household characteristics that prevailed at childbirth. These include the locality (43 per cent rural), rooms per person (one), and monthly per capita household expenditure (172,737 Indonesian Rupiah or approximately US$12). For favorable living conditions we account for the quality of the floor, durable roofing, sufficient ventilation, and asset wealth using consumer durables.
3.4 Pre-disaster sample balance
Before moving on to the estimations, we conduct a pre-disaster sample balance test using the IFLS3 wave summarized in online appendix table A1. It is important to establish that there were no systematic differences in the households and communities before any of the disaster events occurred in this study. As mentioned before, the 1,262 children in the sample are from 998 households in 168 communities. Out of the total, 494 of the households (50 per cent) have experienced at least one type of natural disaster. We find that the only reported imbalance is in the quality of the housing. It appears that the average floor quality in the exposed households was statistically higher than that of the non-exposed households. However, the roof quality and the ventilation were statistically higher (better) in the non-exposed households. Better quality houses should theoretically bias our results toward finding no effect.
At the community level, 86 communities (51 per cent) experienced at least one type of disaster. However, there were no pre-existing differences between the communities based on the availability of formal banks, medicine posts or the distance to the city center. These communities, in the absence of natural disasters, are therefore comparable to each other.
4. Results
4.1 Effects on child stature
We begin the analysis of child stunting by presenting our main results in table 3, which summarizes the coefficients of interest, while the unabridged results are presented in online appendix table A3. The results reveal two key factors. Firstly, while the overall sample does not exhibit any effect on HAZ (panel A, column 1), the girls who were exposed to a multitude of natural disasters are (statistically) significantly shorter (panel A, column 3). Secondly, this is emphasized by the likelihood of stunting as summarized in table 3, panel B. We find that exposed girls are likely to be about 0.19 standard deviations shorter and 7 per cent more likely to be stunted (column 3). The magnitudes, relative to the sample mean, correspond to a 14 per cent reduction in height and a 30 per cent increased likelihood of stunting.Footnote 7 What we observe is the persistent effect of exposure since the outcomes are measured 7 to 12 years after the occurrence of natural disasters in this study.
Table 3. Effects of natural disaster types on child stature

Notes: Estimates of the effect of exposure to natural disasters on child height (standardized) and probability of being stunted, using the fixed effects model as shown in equation (1). Standard errors (in parentheses) are clustered at the community level. All regressions control for child characteristics, pre-disaster parent and household factors listed in table 2, and include religion dummies, birth year, birth month, and pre-disaster municipality of residence fixed effects.
**Significant at 5%.
Source: IFLS panel. Sample: Children on Java Island aged 0–12 in 2007.
Next we turn to measuring severity of exposure using the reported economic loss in table 4. While the HAZ coefficients are no longer statistically significant (panel A), the magnitudes of stunting are much stronger. The children in households with recorded economic loss are 13 per cent more likely to be stunted (panel B, column 1) and this effect is primarily driven by girls (19 per cent).Footnote 8 This result corroborates our findings in table 3, panel B, and henceforth we treat exposure based on disaster types as our main model for brevity.
Table 4. Effects of economic loss from natural disasters on child stature

Notes: Estimates of the effect of household economic loss due to natural disasters on child height (standardized) and probability of being stunted, using the fixed effects model as shown in equation (1). Standard errors (in parentheses) are clustered at the community level. All regressions control for child characteristics, pre-disaster parent and household factors listed in table 2, and include religion dummies, birth year, birth month, and pre-disaster municipality of residence fixed effects.
**Significant at 5%, *significant at 10%.
Source: IFLS panel. Sample: Children on Java Island aged 0–12 in 2007.
The effect we observe is consistent with parental stress and inability to smooth consumption. Experiencing a natural disaster is likely to deprive the child, especially through maternal stress, interrupted prenatal care, loss of or reduction in family income, and consequently loss of nutrition. The gender differential effects found here are qualitatively consistent to that of Datar et al. (Reference Datar, Liu, Linnemayr and Stecher2013) where the authors found that boys are less likely to be stunted than girls when exposed to natural disasters in rural India. Deuchert and Felfe (Reference Deuchert and Felfe2015) document adverse educational outcomes in the long-term for girls exposed to Typhoon Mike in Cebu, The Philippines. However, it is not difficult to find contradictory studies. Cornwell and Inder (Reference Cornwell and Inder2015) found no significant differences in the effect of rainfall on child health based on the gender. Another study reveals that males were more likely to be stunted in the first year, whereas females were more likely to become stunted in the second year of life (Adair and Guilkey, Reference Adair and Guilkey1997). The resilience of girls is documented in Adair (Reference Adair1999) who found that girls are more likely to catch up in the aftermath of growth faltering.
Nonetheless, our magnitudes are qualitatively comparable to studies employing other shocks in early life to estimate the effect on child stature (ex. war (Akresh et al., Reference Akresh, Bhalotra, Leone and Osili2012)). Linear growth retardation in childhood is likely to exacerbate the ability to reach potential as these children grow older. For instance, Vogl (Reference Vogl2014) reports wage gains for both men and women for a one-centimeter increase in height. Overall, we find that exposure to a series of natural disasters affects girls disproportionately and that these effects are visible 7 to 12 years after the disasters.
4.2 Mechanisms
In this section, we concentrate on the pathways through which exposure to natural disasters could adversely affect human capital accumulation. This study puts emphasis on exposure to a multitude of disaster events. However when pinpointing the exact mechanisms, being able to distinguish between different disaster types is useful. For instance, floods could affect the food supply, earthquakes may disrupt access to health facilities, and forest fires could result in respiratory illness. In each of these cases, the mechanisms that lead to poor child health are not uniform. While our sample is not large enough to allow separate identification, we still investigate a potential pathway – access to credit – that could cripple communities as they undergo multiple disaster types in a relatively short period of time (five years).
As shown in Deaton (Reference Deaton1991), households can cope with a disaster using savings. Hill and Porter (Reference Hill and Porter2017) document the plight of Ethiopians in protecting consumption against drought and food inflation. Similarly, multiple disasters occurring concurrently or within a short period of time could overwhelm household savings. Formal banks, on the other hand, play a dual role in the community: encouraging savings and lending credit. We thus study the economic resilience of households through the availability of a formal bank. The ability to smooth consumption through credit accessibility plays an important role as an ex-post risk-coping strategy (Foster, Reference Foster1995; Sawada, Reference Sawada2007). We proxy the access to credit using the availability of a formal bank in IFLS3 (pre-disaster) in the community to avoid shock-related endogeneity in the measurement. In doing so, we create a binary indicator $I$ that is equal to one if the community had a formal bank in IFLS3 and zero otherwise. Next, we interact the exposure variable with the indicator $I$
that is equal to one if the community had a formal bank in IFLS3 and zero otherwise. Next, we interact the exposure variable with the indicator $I$ and modify equation (1) which can be re-written as follows:
and modify equation (1) which can be re-written as follows:

The comparison between ${\beta_1}$ and ${\beta_3}$
and ${\beta_3}$ would then determine if there is a marginal difference in the impact of natural disaster exposure. With regard to credit access, we use ${\beta_1}$
would then determine if there is a marginal difference in the impact of natural disaster exposure. With regard to credit access, we use ${\beta_1}$ as the effect on children exposed to multiple natural disasters in communities without a formal bank. We report ${\beta_1},\; \; {\beta_2},$
as the effect on children exposed to multiple natural disasters in communities without a formal bank. We report ${\beta_1},\; \; {\beta_2},$ and ${\beta_3}\;$
and ${\beta_3}\;$ in table 5.
in table 5.
Table 5. Mechanisms: access to credit

Notes: Estimates of the effect of formal bank availability (ex-ante) in the community on child height (standardized) and probability of being stunted, using the fixed effects model as shown in equation (2). Standard errors (in parentheses) are clustered at the community level. All regressions control for child characteristics, pre-disaster parent and household factors listed in table 2, and include religion dummies, birth year, birth month, and pre-disaster municipality of residence fixed effects.
**Significant at 5%.
Source: IFLS panel. Sample: Children on Java Island aged 0–12 in 2007.
Based on panel A in table 5, girls in communities with limited access to credit (i.e., without a formal bank) are approximately 0.21 standard deviations shorter (panel A, column 3) and 9 per cent more likely to be stunted (panel B, column 3). We also find that the effect of having a bank (${\beta_2}$ ) and the differential effect of exposure in communities that have a bank $({\beta_3})$
) and the differential effect of exposure in communities that have a bank $({\beta_3})$ are both statistically insignificant. Intuitively we would expect credit access to enable consumption smoothing that helps families mitigate some of the losses due to the natural disaster. In the absence of such, households would resort to unsustainable coping mechanisms like ‘liquidated productive assets or slaughtered or sold livestock to overcome the immediate food insecurity thereby jeopardizing their food security in the long-term’ (UNICEF, 2015a: 54). Therefore, we interpret this result as suggestive of the disadvantage the children – particularly girls – face even in the presence of coping strategies.
are both statistically insignificant. Intuitively we would expect credit access to enable consumption smoothing that helps families mitigate some of the losses due to the natural disaster. In the absence of such, households would resort to unsustainable coping mechanisms like ‘liquidated productive assets or slaughtered or sold livestock to overcome the immediate food insecurity thereby jeopardizing their food security in the long-term’ (UNICEF, 2015a: 54). Therefore, we interpret this result as suggestive of the disadvantage the children – particularly girls – face even in the presence of coping strategies.
A valid critique of using availability of a formal bank as a proxy for credit accessibility is that even if there is a bank in the community, there is no certainty that the people (especially the poor) are in fact able to borrow from such institutions. Given general bureaucratic tendencies and the absence of viable collaterals, credit lending to at-risk populations might be minimal, despite the physical existence of a bank. To remedy this issue, we study access to remittances which also help households to smooth consumption. Since seeking employment in cities or abroad could also be an endogenous response to natural disasters, we once again use the IFLS3 wave conducted before these events occurred. IFLS3 did not directly measure the remittances (Adams and Cuecuecha, Reference Adams and Cuecuecha2010; Nguyen and Purnamasari, Reference Nguyen and Purnamasari2011). We thus resort to using migrant workers as a proxy. We define a migrant worker household as one that has at least one family member working outside in a city or abroad. We combine domestic and international migrants since using only the latter would limit the statistical power. Using equation (2), where the $I$ indicator now denotes migrant worker household, we then estimate the differential effect on children in households that would be receiving remittances versus those that do not. We summarize the results in table 6. These results echo those of table 5. Girls in households without the possibility of remittances are equally negatively affected by disasters as those in households with remittances. They are 0.18 standard deviations shorter and 6 per cent more likely to be stunted. We once again do not find an effect on boys. Naturally, we cannot definitively prove that: (a) migrant workers sent remittances; or (b) even if they did, those were used to improve child health. However, assuming that households use remittances to smooth consumption is not unrealistic. Research in Indonesia shows that households with remittances use it for consumption goods – food – rather than investment goods (Adams and Cuecuecha, Reference Adams and Cuecuecha2010). Given the persistence of adverse effects (among girls) even in the presence of access to credit or remittances, this highlights the need for coping mechanisms beyond consumption smoothing.
indicator now denotes migrant worker household, we then estimate the differential effect on children in households that would be receiving remittances versus those that do not. We summarize the results in table 6. These results echo those of table 5. Girls in households without the possibility of remittances are equally negatively affected by disasters as those in households with remittances. They are 0.18 standard deviations shorter and 6 per cent more likely to be stunted. We once again do not find an effect on boys. Naturally, we cannot definitively prove that: (a) migrant workers sent remittances; or (b) even if they did, those were used to improve child health. However, assuming that households use remittances to smooth consumption is not unrealistic. Research in Indonesia shows that households with remittances use it for consumption goods – food – rather than investment goods (Adams and Cuecuecha, Reference Adams and Cuecuecha2010). Given the persistence of adverse effects (among girls) even in the presence of access to credit or remittances, this highlights the need for coping mechanisms beyond consumption smoothing.
Table 6. Mechanisms: access to remittances
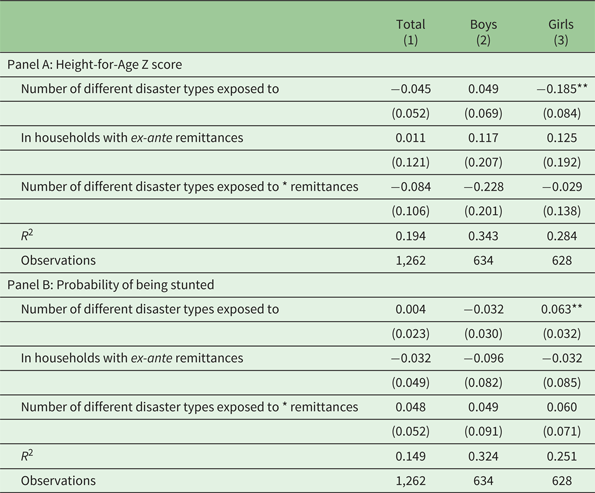
Notes: Estimates of the effect of ex-ante remittance availability in the household on child height (standardized) and probability of being stunted, using the fixed effects model as shown in equation (2). Standard errors (in parentheses) are clustered at the community level. All regressions control for child characteristics, pre-disaster parent and household factors listed in table 2 and include religion dummies, birth year, birth month, and pre-disaster municipality of residence fixed effects.
**Significant at 5%.
Source: IFLS panel. Sample: children on Java Island aged 0–12 in 2007.
4.3 Attrition and mortality selection
Any panel study is likely to yield untrustworthy results if the respondents migrate out of the sample regions. Since children under the age of 12 typically do not migrate on their own, in this section our concern shifts to the migration of their mothers. For instance, if mothers migrated post-disaster to non-IFLS regions because of their experience, the effect we capture through the current analysis is likely to be biased. We therefore construct a separate sample that consists of all the married women – since having children out of wedlock is rare – between the ages of 18 to 44 in 2007 when the disaster information used in this study was collected. These are all the potential mothers of childbearing age. We calculate attrition indicators between the survey rounds 3 to 4, 3 to 5, and 4 to 5 and summarize the results in table 7. The results show that the exposure did not lead to a systematic attrition of childbearing age women in any of the IFLS waves used in this study.
Table 7. Attrition of childbearing age women

Notes: Estimates of the exposure to natural disasters on attrition of childbearing age women. The dependent variable equals 1 if the woman was present in the starting round, but not in the subsequent round; 0 otherwise. All regressions control for information obtained from the starting round: locality (urban/rural), height measured in centimeters, years of education completed, employment status (binary), monthly household expenditure per capita, rooms per person, availability of consumer durables and quality of the housing. Standard errors (in parentheses) are clustered at the community level. All regressions include religion dummies, birth year, birth month, and starting round municipality of residence fixed effects.
Source: IFLS panel. Sample: Married women aged 18–44 in 2007.
Even though married women may not be systematically migrating out of IFLS regions, natural disasters could potentially lead to adverse pregnancy outcomes during prenatal or postnatal stages. Any pregnancy with such adverse outcomes would result in a systematic selection out of our children sample. We thus compile a sample of all the possible pregnancies that, if successful, would have resulted in a child aged 0 to 12 in 2007. These are pregnancies that resulted in any of the outcomes such as live births, miscarriages, stillbirths, or child deaths between 1995 and 2007. Using this newly constructed sample, we estimate three separate models: the likelihood of a child surviving (alive in 2007 – at the time of the survey), a prenatal death (stillbirths and miscarriages), or postnatal death (child no longer alive at the time of survey). The results, as shown in table 8, indicate that the pregnancy outcomes of the disaster-exposed communities are not statistically different from their counterparts. Thus we rule out the possibility of mortality selection among pregnancies due to shock exposure.
Table 8. Mortality selection of pregnancies

Notes: Estimates of the exposure to natural disasters on mortality selection of pregnancies. In column 1 the dependent variable equals 1 if the pregnancy resulted in a live birth and the child was alive at the time of the IFLS 4; 0 otherwise. In column 2 prenatal death is an indicator set to 1 if the pregnancy resulted in a miscarriage or a stillbirth as recorded in IFLS 4; 0 otherwise. Column 3 lists the results for dependent variable postnatal death which is equal to 1 if the pregnancy resulted in a live birth but the child was no longer alive by the time of IFLS 4; 0 otherwise. All regressions control for pre-disaster locality (urban/rural), mother's height measured in centimeters, mother's years of education completed, mother's employment status (binary), monthly household expenditure per capita, rooms per person, availability of consumer durables and quality of the housing. Standard errors (in parentheses) are robust to heteroscedasticity and are clustered at the community level. All regressions include religion dummies, birth year, birth month, and starting round municipality of residence fixed effects.
Source: IFLS panel. Sample: All pregnancies that, if successful, would have resulted in children aged 0–12 in 2007.
4.4 Heterogeneous effects and other robustness checks
In order to unpack the gender differential observed in table 3, we explore two potential factors: the role of agriculture and the preference for sons. Both these factors could have a differential impact on the way the child receives nutrition, care and other resources. In the context of this study, we find evidence only suggestive of the role of agriculture and do not find overwhelming evidence of son preference. The latter is consistent with Levine and Kevane (Reference Levine and Kevane2003) who reveal there are no ‘missing daughters’ in Indonesia. We refer the reader to Note A1 in the online appendix for a further discussion of these results. Another useful method of disaggregation is to study the age of exposure. The most sensible separation of ages would be age 0 (in-utero) to 2, since the seminal work in early childhood literature – Almond and Currie (Reference Almond and Currie2011) – shows the importance of first 1,000 days. In our study, the disaggregation by age does not have statistical power to estimate an effect, hence we are limited to only the aggregate effect of the children exposed.
The binary outcome models in this study are measured using linear probability estimation which could yield potentially biased results. We thus employ a logit model and the results remain robust (available upon request). Finally, we test the validity of the height standardization methodology using the WHO method which is frequently used in the economics literature. Our main results are qualitatively similar to this measure (available upon request). We only report the CDC methodology results following Cornwell and Inder (Reference Cornwell and Inder2015), since Indonesian children are likely to be shorter than the WHO reference group average.
5. Conclusion
Understanding the effects of shocks and unpacking their mechanisms has become more prominent in recent economic literature. Our attempt is to establish causal links between natural disaster exposure and child health using a panel dataset from Indonesia. This paper extends our understanding along three dimensions. Firstly, we study exposure to a series of disasters in a literature that typically focuses on one event. This is relevant for Indonesia given the frequency of natural disasters and the serial correlation between events (e.g., landslides after floods) which makes separate identification problematic. Secondly, we provide evidence of persistent adverse effects in the medium term (lasting 7 to 12 years after exposure) by applying the panel nature of our data. Lastly, we investigate whether the lack of access to credit – either through the availability of a formal bank or family remittances – puts children at a further disadvantage.
We find that girls exposed to multiple natural disasters are persistently at a disadvantage, being 0.19 standard deviations shorter and 7 per cent more likely to be stunted (too short for their age). We find no lasting effect on boys. Even in the presence of consumption smoothing mechanisms like access to credit or remittances, this adverse effect on girls is still prevalent. From a public policy perspective, establishing coping mechanisms beyond credit access, could expedite the recovery process in disaster-affected communities.
Although we concentrate on child stature due to the age constraints of the sample, further studies could look into other potential areas as these children grow older and as more data become available. For instance, school performance, labor and marriage markets would be an interesting endeavor to undertake once sufficient time has elapsed. As many of the children in developing countries are increasingly exposed to natural disasters and extreme weather patterns, understanding coping strategies is likely to become highly relevant for human capital accumulation.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1355770X20000182.
Acknowledgements
The author thanks Marc Rockmore, Paul Christian, Catherine Porter, Martina Kirchberger, Susana Ferreira, and two anonymous referees for their insightful comments. This paper benefited from feedback from the conference participants of the Midwest International Development Economics Conference at the University of Wisconsin - Maddison, Pacific Trade and Development Fellowship for Young Scholars at Australian National University - Canberra, and Center for the Study of African Economies at University of Oxford - UK. The previous version of this paper was entitled ‘The Long-run Effects of Yogyakarta Earthquake on Child Health’. This version replaces the earlier version.









