



A 14-year-old boy was referred to the paediatric cardiology department for investigation of desaturation on transcutaneous pulse oximetry during a cardiopulmonary exercise test. Oxygen saturations were recorded at 76%. His resting oxygen saturations were 94%. The patient had a history as a patient of the cardiology department. He had a small perimembranous ventricular septal defect that had closed spontaneously, and a follow-up transthoracic echocardiogram performed at age 4 had been reported as normal.
At age 5, he developed viral-induced nocturnal cough and was diagnosed with asthma. His parents reported progressive exercise intolerance since ambulant. His exercise tolerance had been attributed to poor level of fitness, although he was not overweight and was active. He had been hospitalised at ages 11 and 12 years with wheezing and chest tightness; chest X-ray at that time showed a hyperinflated chest and a normal cardiac contour, with normal pulmonary vascular markings. His oxygen saturations were 84%.
In the few months before cardiac diagnosis, he presented with hypoxia, chest tightness, and shortness of breath, and was diagnosed with severe asthma. Pulmonary function testing showed normal forced expiratory volume in one second to forced vital capacity ratio and total lung capacity; however, single breath diffusion capacity for carbon monoxide (DLCOcSB) was significantly reduced (z score −2.4). Cardiopulmonary exercise testing demonstrated low peak oxygen consumption (VO2), significant desaturation with exercise, but a normal cardiovascular and ventilatory response to exercise. Ventilatory equivalents for VO2 and VCO2 were elevated throughout the test. These findings raised the possibility of a right-to-left shunt.Reference Sun, Hansen and Oudiz 1
On examination, he had digital clubbing. The precordium was quiet to palpation, and no murmurs were evident. There were no Harrison’s sulci, chest deformity, auscultatory wheeze, or ronchi to suggest chronic severe asthma. His haemoglobin level was 167 g/L.
A transthoracic echocardiogram demonstrated a mildly hypoplastic tricuspid valve and right ventricle. On review, this was evident on the previous echocardiogram as well, obtained 10 years earlier. No other abnormalities were initially noted. A contrast study was undertaken with injection of agitated saline through a vein in the right arm. Echocontrast was demonstrated entering the left atrium. There was an area of clearing of echocontrast proximal to the superior atrial septum in the right atrium, suggesting pulmonary venous (non-contrast) flow across an atrial communication from left to right (Supplementary video clip 1). He subsequently underwent a CT angiogram, cardiac MRI, transoesophageal echocardiogram, and cardiac catheterisation. An atrial septal defect was identified on the CT and MRI, and mild right ventricular hypoplasia was confirmed; in addition, a transoesophageal echocardiogram demonstrated the presence of bidirectional shunting at the atrial level. A thin cord of tissue could be seen extending from the origin of the inferior caval vein to the coronary sinus (Fig 1, Supplementary video clip 2), and three-dimensional reconstruction demonstrated a cor triatriatum dexter (Fig 2). There was no obstruction to flow on colour flow imaging, pulse wave doppler interrogation, or direct pressure measurement during cardiac catheterisation. During atrial septal defect occlusion, using a sizing balloon, right atrial pressure increased from 9 to 11 mmHg. The atrial defect was occluded by deployment of a 15-mm Amplatzer Septal Occluder Device (St. Jude Medical Australia).
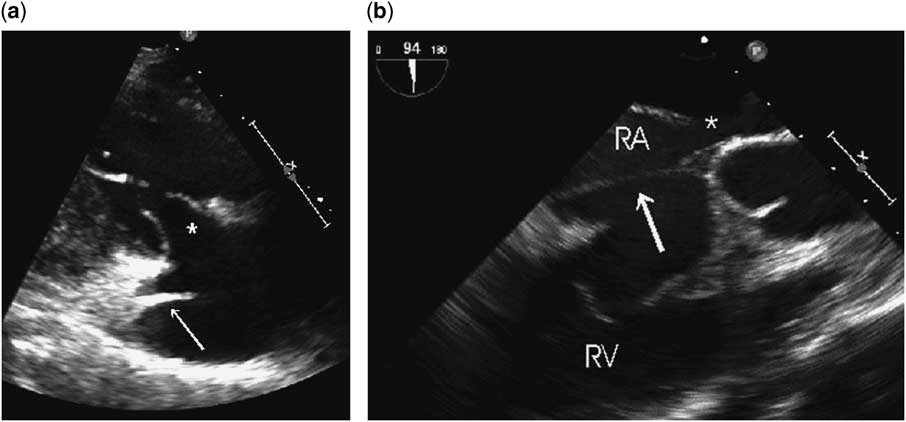
Figure 1 ( a ) Transthoracic echocardiography. Parasternal long-axis, tricuspid view. This still frame of the right atrium shows a cord of tissue that joins the atrial septum superior to the coronary sinus and the inferior caval vein (arrow). The tricuspid valve (*) leaflets appear slightly restricted in diastole, although the annulus is of normal diameter. ( b ) Transoesophageal echocardiography. Still frame at 90° shows the relationship between the atrial septal defect (*), the tricuspid valve, and the incomplete cor triatriatum dexter (arrow). RA=right atrium; RV=right ventricle.

Figure 2 Cor triatriatum dexter three-dimensional image. A still frame from a cropped reconstruction of a three-dimensional full volume acquisition of data during transoesophageal echocardiography. The circumferential membrane can be easily seen in the mid-right atrium. RA=right atrium; TV=tricuspid valve.
An exercise stress test was undertaken on day 7 after atrial septal defect closure, with echocardiography before and after closure. Exercise tolerance was subjectively much improved. The tricuspid valve gradient increased from 3 to 7 mmHg, and right ventricular systolic pressure increased to 36 mmHg+right atrial pressure following exercise. Oxygen saturation remained normal.
Follow-up echocardiography after 3 months demonstrated mild tricuspid hypoplasia with a 2 mmHg mean inflow gradient and laminar colour flow through the right atrium. There was no right atrium pressure gradient across the tissue cord.
Discussion
In this case report, we document a rare cause of exercise-induced hypoxia: bidirectional shunting across a secundum atrial septal defect, due to an incomplete cor triatriatum dexter or prominent eustachian valve, and mild hypoplasia of the right ventricle.
Diagnosis of the cardiac cause for hypoxia was delayed due to an unappreciated atrial septal defect on two previous transthoracic echocardiograms, possibly because there was very little flow across the defect at rest on colour flow imaging. The exercise-induced symptoms were instead attributed to asthma. On careful history, there was no exercise-induced wheezing, no response to bronchodilator therapy before exercise, and episodes of wheezing had been only associated with viral illness. Furthermore, pulmonary function testing was inconsistent with asthma.
Cor triatriatum, or tripartite atria, constitute 0.1–0.4% of congenital heart lesions, although incomplete defects may go undiagnosed in the absence of symptoms. Cor triatriatum sinister, or bipartite left atrium, is the more common of this rare defect. Cor triatriatum dexter is due to the persistence of a normal embryological state: during development, the right atrium is partitioned into two by the right valve of the right horn of the sinus venosus, which connects the inlet of the inferior caval vein to the coronary sinus, and directs oxygenated blood across the oval fossa to the left atrium. In normal development, the valve regresses, leaving as remnants the crista terminalis superiorly and eustachian valve of the inferior caval vein and the Thebesian valve of the coronary sinus inferiorly.Reference Anderson 2 Cor triatriatum dexter is often associated with other heart defects including atrial septal defects.Reference Verel, Pilcher and Hynes 3 Abnormalities documented include complete or almost complete persistence of the valve, cor triatriatum dexter, a prominent eustachian valve with partial septation of the right atrium, or a giant redundant membrane able to occlude the inferior caval vein, an atrial septal defect, or the tricuspid valve orifice.Reference Yavuz, Nazli and Kinay 4 , Reference Bejiqi, Retkoceri and Bejiqi 5 Management may include balloon dilation of the membrane or excision.
In this case, there was no pressure gradient across the membrane; however, there was mild hypoplasia of the right ventricle and tricuspid valve and bidirectional flow across the atrial septal defect. In anatomical studies of tricuspid stenosis or atresia, abnormal prominence of the eustachian valve has been found in up to 80% of cases, including cor triatriatum dexter in 25%.Reference Schutte, Rowland and Allen 6 We hypothesise that abnormal foetal flow directed predominantly across the atrial septal defect was the likely cause of ventricular hypoplasia. Limited right ventricular compliance led to increased right-to-left shunting with exercise, mimicking exercise-induced asthma.
Summary
Right-to-left shunting across the atrial septum is a rare cause of exercise-induced hypoxia. Contrast echocardiography is likely to detect or exclude this lesion. A careful history, examination, and pulmonary function testing may highlight inconsistencies with other common diagnoses of exercise-induced symptoms such as asthma.
Acknowledgement
None.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.
Ethical Standards
Consent was obtained from the patient’s parents and assent from the patient. The authors assert that all procedures contributing to this work comply with the NHMRC National Statement on Ethical Conduct in Human Research (2007) and with the Helsinki Declaration of 1975, as revised in 2008.
Supplementary Material
For supplementary material referred to in this article, please visit http://dx.doi.org/10.1017/S1047951115001870



