


Conventionally, fluoroscopy is used for catheter navigation during invasive electrophysiological procedures. Prolonged exposure to fluoroscopy is potentially hazardous for patients and laboratory personnel. Catheter ablation procedures reportedly increase long-term cancer risk by 0.02%.Reference Clay, Campbell, Strieper, Frias, Stevens and Mahle 1
First introduced in 1997, the novel non-fluoroscopic catheter-based endocardial mapping systems allow users to obtain a three-dimensional electroanatomical map of the cardiac chambers and identify the critical ablation site more accurately.Reference Gepstein, Hayam and Ben 2 – Reference Eckardt and Breithardt 4 The EnSite NavX system is one of these methods and does not require the use of manufacturer-specific catheters, which enable the use of both radiofrequency and cryothermal technology, as well as various “cooled tip” radiofrequency ablation technology.Reference Eckardt and Breithardt 4 – Reference Von Bergen, Bansal, Gingerich and Law 6
EnSite NavX system (St. Jude Medical, St Paul, Minnesota, United States of America) can significantly decrease or even eliminate fluoroscopy exposure during the catheter ablation of supraventricularReference Tuzcu 5 , Reference Smith and Clark 7 and ventricular tachycardia substrates.Reference Ferguson, Helms and Mangrum 8 – Reference Justino 10 The few studies conducted among children reported a success rate of 60% for conventional ventricular tachycardia ablation and up to 90% with the use of EnSite NavX system.Reference Schneider, Kriebel, Jung, Gravenhorst and Paul 3 , Reference Von Bergen, Bansal, Gingerich and Law 6 , Reference Morwood, Triedman and Berul 11 The aim of this study was to demonstrate the utility of an EnSite NavX system in the catheter ablation of idiopathic ventricular tachycardia in children.
Patients and methods
Study population
This single-centre retrospective cohort study evaluated all patients under 18 years of age who underwent ablation for idiopathic ventricular tachycardia using EnSite NavX system. A total of 17 consecutive children who were admitted to our institution between January, 2010 and February, 2012 with recurrent symptomatic episodes of monomorphic idiopathic ventricular tachycardia were included. The demographic, procedural, and follow-up data were collected. The patients with ventricular tachycardia related to congenital heart disease, primary electrocardiograms abnormalities – Brugada syndrome, catecholaminergic ventricular tachycardia, long QT syndrome – and primary cardiomyopathies – hypertrophic, dilated – were excluded.
All patients had 12-lead electrocardiograms and 24-hour ambulatory electrocardiograms taken before the ablation procedure. Out of 17 patients, 10 demonstrated a left bundle branch block pattern, while seven had a right bundle branch block pattern during ventricular tachycardia on the surface electrocardiograms. Indications for ablation were syncope or near-syncope in two patients; recurrent palpitations with antiarrhythmic medications not being effective, tolerated, or desired in 14; and patient's and parents’ choice in one. There was one patient who previously underwent a failed ablation attempt at a different centre.
Electrophysiological study and catheter ablation
Antiarrhythmic medications were discontinued at least five half-lives before the electrophysiological studies. All patients and/or their legal guardians gave consent for the procedure. General anesthesia was used in 15 patients and deep sedation was used in two. EnSite NavX system was used for catheter navigation, three-dimensional mapping, and activation mapping in addition to a conventional electrophysiological system. The procedure was started without using fluoroscopy by inserting a 7 Fr sheath into the right femoral vein and two 6 Fr sheaths into the left femoral vein. The catheters were placed into the right atrium, coronary sinus, and the right ventricle using the guidance of the EnSite NavX system. Three-dimensional images of the superior and inferior vena cava, right atrium, coronary sinus, and right ventricle anatomies were obtained. If the origin of ventricular tachycardia was in the left ventricle, a decapolar catheter was inserted through the femoral artery into the left ventricle. All patients underwent a basic electrophysiological study. The 12-lead electrocardiograms of all patients were reviewed for any ventricular ectopy and non-sustained or sustained ventricular tachycardia in order to ensure that the targeted morphology was identical to the clinical tachycardia. Activation, voltage, and pace mapping were utilised as needed. If ventricular tachycardia did not occur spontaneously and could not be induced with standard programmed ventricular stimulation, 0.125 mg isoproterenol was administered as an intravenous bolus or dobutamine infusion was started at 5 mg/kg/minute (up to 20 mg/kg/minute). Except for in one case where a 7 Fr 6-mm tip cryoablation catheter was used for the parahissian origin of ventricular tachycardia, 7 Fr 4-mm tip radiofrequency ablation catheters were used. The ablation sites were marked, and additional applications of energy were delivered at and around the sites after initial application. The ablation was considered successful if there were no spontaneous or isoproterenol-induced ectopic beats or ventricular tachycardia 30 minutes after the procedure. To reduce the risk of thromboembolic complications associated with radiofrequency ablation, intravenous heparin was administered at 75 U/kg if the left ventricle was entered. Heparin doses were adjusted to achieve a goal activated clotting time level of 150–200 seconds. Following the procedure, patients who had an ablation performed within the left ventricle were placed on aspirin therapy for 6 weeks.
Follow-up
As a standard, all patients underwent continuous telemetry monitoring, a 12-lead electrocardiogram, 24-hour ambulatory electrocardiogram, and echocardiography before they were discharged. All patients were also hospitalised following the ablation procedure per standard practice. Echocardiograms were obtained when they were felt to be clinically indicated. If ablation was performed in the left ventricle during the procedure, the patient received acetylsalicylic acid at 3–5 mg/kg for 6 weeks after discharge. All patients were examined at our outpatient clinic for symptoms suggestive of arrhythmia 1, 3, and 6 months after the procedure and then every 12 months. At each visit, a 12-lead electrocardiogram and 24-hour ambulatory electrocardiogram monitoring were performed.
Statistical analysis
Statistical Package for the Social Sciences 15.0 for Windows (SPSS, Chicago, Illinois, United States of America) was used for the data analysis – reliability, construct validity, and internal consistency. The mean values and intervals were specified as ± standard deviation. The comparison of categorical variables was performed using the χ2 test and Fisher's exact test. Continuous variables were analysed using the Mann–Whitney U-test for non-normally distributed variables. The difference was considered to be significant if the p-value was below 0.05.
Results
Patient characteristics and radiation exposure
All demographic and clinical characteristics of patients are presented in Table 1. In a 2-year period, 17 patients (age range: 7.8–17.9 years) underwent electrophysiological studies and ablations due to ventricular tachycardia or frequent ventricular ectopy. Despite antiarrhythmic treatment, 76% of patients (13/17) had recurring palpitation attacks. Left ventricular function was within normal limits in all patients. The origin of ventricular tachycardia was the right ventricular outflow tract in nine patients, left posterior fascicle in five, epicardial left ventricular lateral wall in one, parahissian region in one, and left aortic cusp in one. The mean procedure duration was 169.3 ± 43.2 minutes (range: 100–240 minutes); the mean fluoroscopy time was 8 ± 10.8 minutes (range: 3–36 minutes). The mean radiation exposure was 33.1 ± 56.4 mGy. No fluoroscopy was used in six patients, all of whom had origin of ventricular tachycardia in the right ventricular outflow tract (Fig 1). Fluoroscopy duration was significantly longer in the patients with left ventricular ventricular tachycardia (p = 0.01). The patient with the origin of ventricular tachycardia near the left coronary cusp had the longest fluoroscopy and procedure times (36 and 240 minutes, respectively) owing to coronary angiography and the epicardial mapping of ventricular tachycardia. No fluoroscopy was used for venous or arterial access in any patient.
Table 1 Demographic and clinical characteristics of the study population.

ECHO = echocardiography; F = female; LBBB = left bundle branch block; LV = left ventricle; M = male; RBBB = right bundle branch block; SF = shortening fraction
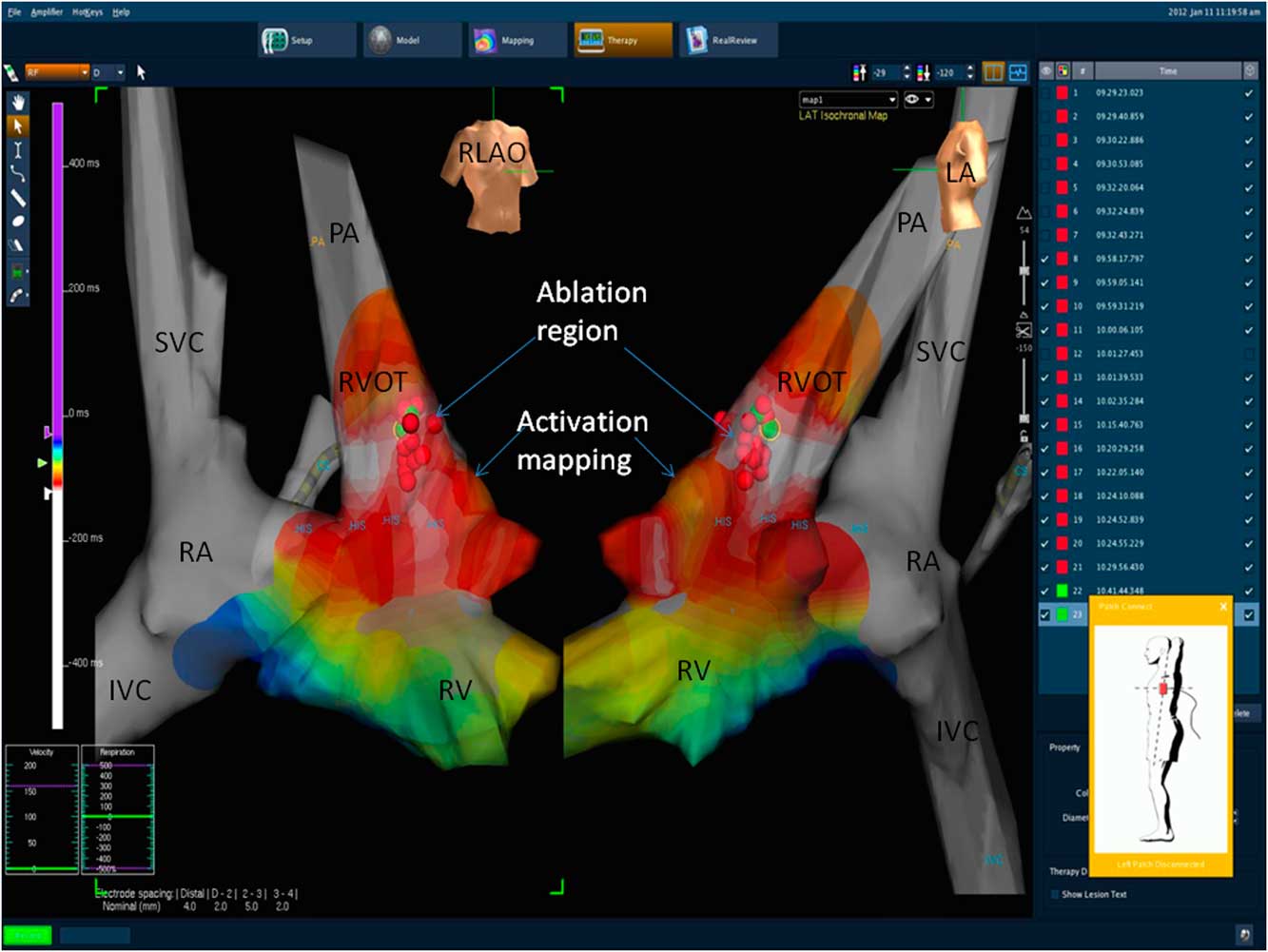
Figure 1 Right ventricular outflow tract tachycardia ablation and activation mapping using the EnSite NavX system. IVC = inferior vena cava; LA = lateral position; PA = pulmonary artery; RA = right atrium; RLAO = right lateral oblique position; RV = right ventricle; RVOT = right ventricular outflow tract; SVC = superior vena cava.
Procedure characteristics and results
All ablation procedure characteristics are presented in Table 2. Radiofrequency ablation was used in 16 patients and cryoablation in one. For radiofrequency ablation, the mean number of applications was 9.1 ± 7.46 (1–29 lesions). The mean radiofrequency application duration was 377.4 seconds (range: 31–600). The mean cycle length was 399.20 ± 95.39 ms, while the mean earliest local activation time was 32 ± 9.9 ms (range: 23–58 ms). The number of radiofrequency applications was significantly higher in the patients with left ventricular tachycardia (p = 0.03). Other procedure parameters and local activation times did not vary significantly between the patients with right ventricular and left ventricular tachycardia (p > 0.05 for each).
Table 2 Procedure results.

EAT = earliest activation time before onset of QRS complex; LV = left ventricular; RV = right ventricular; RF = radiofrequency
The six RV tachycardia patients who did not require fluoroscopy have not been included in these averages (when included, the average fluoroscopy time is 3.8 ± 7.4 minutes)
When analysed on an intention-to-treat basis, the acute success rate was 14 out of 17 (82.3%). In general, the success rate did not vary significantly between the patients with right ventricular and left ventricular tachycardia (p > 0.05), but the best results were achieved in the cases with left posterior fascicular ventricular tachycardia (5/5, 100%) (Fig 2). Out of patients in whom ablation was not successful, focus was right ventricular in two and left ventricular in one. In two of the failed procedures, ventricular tachycardia focus was epicardial. Epicardial ventricular tachycardia was suspected when there was a prolonged precordial maximum deflection index. In addition, it was also determined using three-dimensional mapping, activation mapping, and pace mapping during the electrophysiological study. In the third patient, ventricular tachycardia focus was near the bundle of His/right bundle branch and cryoablation was used to reduce the risk of permanent block. However, the patient developed transient episodes of right bundle branch block during cryomapping with a 6-mm tip catheter; the longest episode of right bundle branch block lasted for 5 minutes after cryomapping was stopped and the procedure could not be continued. Wenckebach cycle length was unchanged at the end of the procedure. No other complications were noted. Echocardiography performed after the procedure documented absence of aortic valve insufficiency following the retrograde approach. Pericardial effusion was not seen in any of the patients.

Figure 2 Left posterior fascicle ventricular tachycardia ablation using the EnSite NavX system. CS = coronary sinus; IVC = inferior vena cava; LLAO = left lateral oblique position; LV = left ventricle; PFR = posterior fascicle region; RA = right atrium; RLAO = right lateral oblique position; SVC = superior vena cava.
Follow-up
During the mean follow-up of 8.47 ± 7.64 months (range: 3–25), three out of 14 patients (21.4%) suffered tachycardia recurrence. Of these patients, two underwent a second successful procedure. In the third patient, the tachycardia focus was epicardial and in close proximity to the left main coronary artery. Further procedure was not attempted in that patient in order to avoid coronary artery injury, and the tachycardia was controlled medically. With the short-term follow-up considered, the success rate was 76.5% (13/17).
An analysis was performed to look at ablation success rates as a function of fluoroscopic times. The use of limited fluoroscopy was not a factor affecting acute or long-term success. The use of fluoroscopy and fluoroscopy durations was assessed and no difference was found between the group with acute success and the group with failed ablation attempt (p = 0.910, 0.867, respectively). The same analysis was performed for long-term success and the fluoroscopy use and durations were comparable between the groups with long-term success and recurrence (p = 0.725, 0.124, respectively).
Discussion
This study demonstrates the feasibility of a limited fluoroscopy approach using the EnSite NavX system for ablation of idiopathic ventricular tachycardia in children. Given the variety of cases in this study, including both left and right ventricular arrhythmias, this approach can be justified for many ventricular arrhythmias.
Electroanatomical mapping systems have been used longer than one decade for localisation of tachycardia substrates and ablation of electroanatomic systems. Electroanatomic mapping technologies can be subdivided into those that combine electrophysiological data with anatomic information, which mainly include CARTO (Biosence-Webster, Baldwin Park, California, United States of America) and, more recently, CARTOMerge (Biosence-Webster) and EnSite NavX (St. Jude Medical), and non-contact mapping (EnSite 3000; St. Jude Medical). The first two techniques localise catheter position in space by sensing changes in its position within a magnetic field (CARTO), or by sensing impedance changes between the catheter and reference points (EnSite). The non-contact mapping technique uses an endocardial multielectrode balloon (over 3300 electrodes) that allows to detect the tachycardia focus in cases where ventricular tachycardia is difficult to induce, even when there is only a single ventricular ectopic beat.Reference Schneider, Kriebel, Jung, Gravenhorst and Paul 3 , Reference Eckardt and Breithardt 4 In addition, EnSite NavX system has been shown to be helpful in reducing patient and operator exposure to radiation during mapping.Reference Eckardt and Breithardt 4 – Reference Von Bergen, Bansal, Gingerich and Law 6 In our institute, we use EnSite NavX because it allows electroanatomic mapping for ablation in tachycardia substrates and it reduces radiation exposure in the operators.
Reducing long-term effects of radiation exposure in patients who undergo cardiac catheterisation and the laboratory personnel has always been on the agenda. The As Low As Reasonably Achievable principle and recent studies confirm that children who undergo longer exposure to radiation are at bigger long-term risk of developing malignancies.Reference Justino 10 , Reference Limacher, Douglas and Germano 12 , Reference Wagner 13 For this reason, it is essential that manufacturers of medical equipment and health workers follow the guidelines and exercise careful judgement. 14
The acute success rate in our study was 82.3%. The main causes of failed ventricular tachycardia ablation and high recurrence rates can be listed as follows: (1) inability to find the critical ablation zone using conventional mapping due to the lack of sufficient ventricular ectopy; (2) high-risk localisation of ventricular tachycardia origin – next to the bundle of His or coronary arteries; (3) deep endocardial or epicardial localisation of ventricular tachycardia origin; (4) inability to perform ablation because of unstable ventricular tachycardia.Reference Schneider, Kriebel, Jung, Gravenhorst and Paul 3 , Reference Eckardt and Breithardt 4 , Reference Morwood, Triedman and Berul 11 , Reference Wen, Taniguchi, Yeh, Wang, Lin and Wu 15 In addition, in adult patients with idiopathic ventricular tachycardia who undergo ablation using conventional methods, performing only pace mapping and earliest endocardial activation time has been shown to be the only independent predictor of ventricular tachycardia recurrence.Reference Wen, Taniguchi, Yeh, Wang, Lin and Wu 15 Furthermore, fluoroscopy-based anatomical mapping does not show endocardial contours clearly, thus prolonging and complicating the procedure. This in turn makes ablation of unstable ventricular tachycardia and short arrhythmias particularly challenging.Reference Eckardt and Breithardt 4
Although there are numerous studies of supraventricular tachycardia ablation in children using various three-dimensional mapping systems, there are only two that focus on ablation of idiopathic ventricular tachycardia.Reference Schneider, Kriebel, Jung, Gravenhorst and Paul 3 , Reference Tuzcu 5 – Reference Smith and Clark 7 In a study by Schneider et al,Reference Schneider, Kriebel, Jung, Gravenhorst and Paul 3 ablation was performed using the multi-electrode array balloon and non-contact mapping (EnSite 3000) method on 19 out of 20 patients with idiopathic ventricular tachycardia and the procedure was successful in 17 (85%). There were no complications except transient atrioventricular block in one patient, and the mean fluoroscopy time was 20.7 minutes. However, the inability to use the multi-electrode balloon in patients weighing under 15 kg and the long procedure duration (302 minutes in that study) appear to be the disadvantages of this method. In addition, during the unstable ventricular tachycardia ablation, multi-electrode balloon can lead to outflow tract obstruction, which can destabilise haemodynamics. Although EnSite NavX System does not seem to add an additional advantage in acute success rate, its major advantage is lower radiation exposure.
In a case series study by Von Bergen et alReference Von Bergen, Bansal, Gingerich and Law 6 where EnSite NavX was used for ventricular tachycardia ablation, fluoroscopy was used in two out of five patients and was not used in the three patients with right-sided ventricular tachycardia. The procedure was successful in all five patients and no complications were reported. In our study, fluoroscopy was used in 11 cases out of 17; in six patients with right ventricular tachycardia, only EnSite NavX system guidance was used. No additional imaging methods such as intracardiac ultrasonography were used in any of the patients. The mean procedure time was 169 minutes, whereas the mean fluoroscopy time was only 8 minutes. Similar to the medical literature,Reference Schneider, Kriebel, Jung, Gravenhorst and Paul 3 fluoroscopy duration was longer in the patient with epicardial ventricular tachycardia localisation in the left coronary cusp, as coronary angiography was also performed.
Considering the reported mean fluoroscopy times – 34.2–38.5 minutes for conventional ventricular tachycardia ablation methods in adults and 20.7 minutes for non-contact mapping in children with ventricular tachycardiaReference Schneider, Kriebel, Jung, Gravenhorst and Paul 3 , Reference Wen, Taniguchi, Yeh, Wang, Lin and Wu 15 – the fluoroscopy time of 8 minutes in our study was minimal in comparison, and fluoroscopy was avoided altogether in six out of 17 patients. The EnSite NavX system helps to minimise or avoid radiation without requiring multi-electrode balloon or any specific catheters, which is an advantage for children because of smaller body size. In addition, fluoroscopy may be needed as an adjunct to the NavX system when clinically indicated, such as confirming catheter or sheath position.
Study limitations
This study is limited by the inherent nature of a retrospective study involving a small patient number owing to the rare prevalence of the disease. In addition, the follow-up period was relatively short because the study was performed at a new institution, which limits the power of the results.
Conclusion
Catheter ablation of idiopathic ventricular tachycardia in children can be performed safely, effectively, and with short fluoroscopy duration using the EnSite NavX system. Potential long-term side effects of radiation exposure can be minimised for both patients and catheterisation laboratory personnel with the utility of the system in these procedures
Acknowledgements
None
Financial Support
None.




