


Introduction
Cochlear implants (CIs) provide significant benefits for speech perception and language development for children with severe to profound hearing loss (i.e., losses of 70 dBHL or greater), with the body of research indicating that age-appropriate language is more likely to be acquired by children when CIs are implanted at a younger age (e.g., Ching et al., Reference Ching, Dillon, Button, Seeto, Van Buynder, Marnane and Leigh2017; Colletti, Reference Colletti2009; Nicholas & Geers, Reference Nicholas and Geers2013). One study by Niparko and colleagues (2010) reported a language advantage for children implanted by 18 months compared with those implanted between the ages of 18 and 36+ months, while other studies have reported language outcome advantages for children implanted at even younger ages (e.g., Artieres, Vieu, Mondain, Uziel, & Venail, Reference Artieres, Vieu, Mondain, Uziel and Venail2009; Holt & Svirsky, Reference Holt and Svirsky2008), including infants implanted under 12 months (e.g., Ching et al., Reference Ching, Dillon, Button, Seeto, Van Buynder, Marnane and Leigh2017; Cuda, Murri, Guerzoni, Fabrizi, & Mariani, Reference Cuda, Murri, Guerzoni, Fabrizi and Mariani2014; Dettman, Pinder, Briggs, Dowell, & Leigh, Reference Dettman, Pinder, Briggs, Dowell, & Leigh and R2007; Houston & Miyamoto, Reference Houston and Miyamoto2010; Leigh, Dettman, Dowell, & Briggs, Reference Leigh, Dettman, Dowell and Briggs2013).
However, although early cochlear implantation provides children with the opportunity to become familiar with the sounds of the ambient language in a time frame that facilitates early vocabulary development, there is likely to be some delay, compared to the vocabulary development of children with normal hearing (NH) (Välimaa, Kunnari, Laukkanen-Nevala, Lonka, & The National Clinical Research Team, Reference Välimaa, Kunnari, Laukkanen-Nevala and Lonka2018). The vocabulary and grammar of children with CIs may ‘catch up’ to that of their peers within a few years, as indicated by the vocabulary knowledge they show or age-expected scores they achieve in language assessments, but for a proportion of children with CIs it does not (e.g., Geers, Moog, Biedenstein, Brenner, & Hayes, Reference Geers, Moog, Biedenstein, Brenner and Hayes2009; Szagun, Reference Szagun2001), and delay in different aspects of language may be found (Duchesne, Sutton, & Bergeron (Reference Duchesne, Sutton and Bergeron2009). As with children with NH, for those children with CIs whose language development remains significantly delayed, there may be a poorer quality of life, based on the reported impact of children's early language skills on later social, behavioural, and academic outcomes (e.g., McKean et al., Reference McKean, Reilly, Bavin, Bretherton, Cini, Conway and Mensah2017).
Research on the growth of communicative development in children implanted with CIs in infancy is important because it has the potential to provide insights into possible reasons for variability in language outcomes. A clearer understanding of predictive factors for positive outcomes can inform the design and implementation of appropriate early intervention and parenting programmes, thereby helping to facilitate optimal outcomes for a larger number of children with CIs.
As shown in the language acquisition literature, while there is variability in the early communicative development and subsequent language development for children with NH (Fenson et al., Reference Fenson, Marchman, Thal, Dale, Reznick and Bates2007), the path to language typically follows a developmental continuum. Children become attuned to the sound patterns of the surrounding language during their first year (Werker & Tees, Reference Werker and Tees1984) and this provides them with cues to spoken vocabulary development (Werker & Yeung, Reference Werker and Yeung2005). Vocabulary development is a precursor to language (e.g., Bates & Goodman, Reference Bates, Goodman and MacWhinney1999), that is, the patterns of combining words and grammatical elements (Levine, Strother-Garcia, Golinkoff, & Hirsh-Pasek, Reference Levine, Strother-Garcia, Golinkoff and Hirsh-Pasek2016). However, prior to acquiring and using words, children use non-linguistic means to communicate, both vocal (e.g., cries) and non-vocal (gestures and facial expressions). A body of research has reported on early vocalisations of children with NH (e.g., Kuhl & Meltzoff, Reference Kuhl and Meltzoff1996). Other research has focused on gesture use, showing it to be a precursor to and predictor of early vocabulary in hearing and deaf children (e.g., Acredolo & Goodwyn, Reference Acredolo and Goodwyn1988; Goldin-Meadow, Reference Goldin-Meadow2015; Iverson & Goldin-Meadow, Reference Iverson and Goldin-Meadow2005; Rowe & Goldin-Meadow, Reference Rowe and Goldin-Meadow2009; Volterra, Iverson, & Castrataro, Reference Volterra, Iverson, Castrataro, Schick, Marschark and Spencer2006). Gesture use has also been reported as a predictor of early vocabulary development for young children with CIs (e.g., Bavin et al., Reference Bavin, Sarant, Leigh, Prendergast, Busby and Peterson2018).
Growth in the use of gestures, nonword vocalisations, single words and multiword utterances, that is, four early means of communication in children with NH was examined by Greenwood et al. (Reference Greenwood, Walker, Buzhardt, Howard, McCune and Anderson2013). The measure used was the Early Communication Indicator (ECI; Carta, Greenwood, Walker, & Buzhardt, Reference Carta, Greenwood, Walker and Buzhardt2010; Greenwood, Carta, Walker, Hughes, & Weathers, Reference Greenwood, Carta, Walker, Hughes and Weathers2006), a standardised play-based measure of timed interactions between a child and familiar adult for children 6–42 months of age. The ECI is a well-established measure. It can be frequently repeated, more so than other early communication measures (e.g., the Preschool Language Scale or the Ages and Stages Questionnaire), and so is particularly well suited for analysing growth over time rather than proficiency at a single point in time. Based on growth curve modelling, Greenwood et al. (Reference Greenwood, Walker, Buzhardt, Howard, McCune and Anderson2013) found that a sample of children without any identified disabilities used both gestures and nonword vocalisations at 6 months of age. The use of nonword vocalisations rapidly increased through to 18 months and then decreased as the children began replacing them with words. Single words emerged at 12 months, and these continued to increase to about 34 months. Multiword utterances began to emerge at about 18 months; they overtook single word use as the children became more fluent in using phrases and sentences. These results indicated a developmental trajectory, with progression from the use of gestures and nonword verbal vocalisations to single words and then to multiword utterances as the children started to combine the words following the patterns detected in the input language. Importantly, however, each means of communication continued to be used as a new skill emerged; for example, gestures continued to be used when words appeared. As discussed by Goldin-Meadow (Reference Goldin-Meadow2014), new functions develop for gestures when words replace them, and thus when the two are combined they provide an additional representational format that can promote learning.
Rate of early vocabulary growth has been identified as a predictor of later vocabulary development for children with NH. Rowe, Raudenbush, and Goldin-Meadow (Reference Rowe, Raudenbush and Goldin-Meadow2012), for example, using modelled growth estimates, found that acceleration and velocity of growth in children's vocabulary at 30 months predicted the children's later vocabulary. Thus, variability in the growth rates of early vocabulary for young children with CIs might help to explain some of the variability in their later language outcomes. Tomblin, Barker, and Hubbs (Reference Tomblin, Barker and Hubbs2007) reported a more rapid rate of development of early language for children implanted with CIs in infancy rather than as toddlers. In other research, Szagun and Stumper (Reference Szagun and Stumper2012) reported a faster rate of language growth for children implanted before 24 months of age, and Niparko et al. (Reference Niparko, Tobey, Thal, Eisenberg, Wang and Quittner2010) reported that for both comprehension and expression of children who were implanted at younger ages there was significantly faster growth.
More research is needed, however, to help to identify the extent to which young children with CIs follow or diverge from the typical trajectories and growth reported for children with NH in the early stages of communicative development. The results of such research could be of benefit to parents, teachers, and clinicians in assisting young children with CIs to develop communication skills in their progression to language.
The current CI study is unique in its use of the ECI, with observations conducted in the child's home to provide a context in which to observe the early communicative exchanges between child and parent. We are not aware of any previous research that has used the ECI to measure the developmental trajectory from prelinguistic means of communication to early vocabulary in a CI sample. The ECI has strong psychometric properties (Greenwood, Walker, & Buzhardt, Reference Greenwood, Walker and Buzhardt2011) and also explicit coding criteria to facilitate discrimination among various types of communicative means (see ‘Materials and methods’ section below for details). Analyses were conducted on the data collected from the CI sample in the current study to determine growth patterns in the children's use of four communication means over a 15-month period. Subsequent analysis was conducted to compare the growth patterns of the CI sample to those of a sample of children with NH. In the analyses we included two potential influencing factors that have previously been shown to impact on vocabulary development, for both children with NH and children with CIs. Child gender was included based on past research with young children with NH (e.g., Fenson et al., Reference Fenson, Marchman, Thal, Dale, Reznick and Bates2007; Reilly et al., Reference Reilly, Wake, Bavin, Prior, Williams, Bretherton and Ukoumunne2007), and in children with CIs (Cuda et al., Reference Cuda, Murri, Guerzoni, Fabrizi and Mariani2014; Geers et al., Reference Geers, Moog, Biedenstein, Brenner and Hayes2009; Välimaa et al., Reference Välimaa, Kunnari, Laukkanen-Nevala and Lonka2018). Maternal education was also included as a possible moderator. Quality of linguistic input to a child has been associated with level of maternal education in past research, with a higher education level predicting larger vocabularies in young children with NH (e.g., Fernald, Marchman, & Weisleder, Reference Fernald, Marchman and Weisleder2013; Hoff, Reference Hoff2003; Rowe, Reference Rowe2012), and similar findings have been reported in research with young CI samples (e.g., Cuda et al., Reference Cuda, Murri, Guerzoni, Fabrizi and Mariani2014; Szagun & Stumper, Reference Szagun and Stumper2012; Välimaa et al., Reference Välimaa, Kunnari, Laukkanen-Nevala and Lonka2018).
A third possible influencing factor included in the analyses of the ECI data from the CI sample was time to achieve consistent use of the CIs. This variable has previously been reported as a predictor of early vocabulary of children with CIs (Bavin et al., Reference Bavin, Sarant, Leigh, Prendergast, Busby and Peterson2018). It was selected in preference to time since surgery or time since CI switch-on because it is a more accurate representation of actual CI use. Time since surgery is problematic because the time interval between surgery date and fitting of the sound processor can vary across CI centres. Time since switch-on is also problematic because, as often reported by clinic staff (and parents), families vary in how well they adapt to using the new device, particularly immediately after implantation. While some parents are vigilant, ensuring that their infant wears the device regularly, others are not.
The current study focused on extending the limited body of past research on early communication with children implanted at a young age. Specifically, we investigated the progressive development of early communication skills for children with CIs implanted in infancy, the effect of three factors (gender, maternal education, and time to achieve consistent CI use) on early communication growth, and whether a similar pattern of growth would be found for the CI sample and children with NH. We addressed the following research questions:
1. What are the associations between the use of early gestures, nonword vocalisations, single words, and multiword utterances over a 15-month period in a sample of children implanted with CIs in infancy?
2. What are the communication growth trajectories for the CI sample?
3. Do child gender, maternal education, and time taken to reach consistent use of the CIs significantly affect outcomes?
4. To what extent are the growth trajectories of children in the CI sample similar to those of a sample of children with NH from similar backgrounds?
5. Are there differences in the impact of child gender and maternal education between the two samples?
Materials and methods
Participants
CI sample
The children in the CI sample (n = 33, male = 17 (51.5%)) were recruited prior to receiving their CIs from five CI clinics across four states in Australia (Victoria, New South Wales, Queensland, and South Australia). Human research ethics approval was obtained from the relevant committees associated with the clinics and university (see ‘Acknowledgements’ for details). All eligible families were provided with information about the study by the staff at the clinic they attended. The families were from urban and rural locations and from across the socioeconomic spectrum. They were eligible to participate in the study if: (1) their child had severe to profound hearing loss and had been assessed as appropriate for CIs; (2) the main language spoken in the home was English; and (3) their child did not have other identified disabilities. Families indicated if they would like more information about the study. If so, they were contacted by a member of the research team who provided more details, answered any questions, and obtained written informed consent to participate in the study. An initial home visit was then arranged and at that visit demographic information was collected. Because of their other family commitments, two families decided not to participate after receiving further information about the study. One additional child initially included was later identified with developmental delay and so was not included in the final sample of 33.
The median age of the children at implantation was 9 months. Ninety-four percent of the sample were implanted between 6 and 16 months (22 between 6 and 10 months, with an additional 9 by 16 months, and 2 at 21 months). Most (85%) had bilateral implants; the other 15% had unilateral implants and a hearing aid in the other ear. Switch-on time was approximately two weeks after surgery (m = 16 days, SD = 5 days).
All children had hearing parents, and spoken language was the medium of communication; no parents in the sample communicated using Australian Sign Language (Auslan). Families could, however, access available internet resources on Auslan signs and also DVDs and an Auslan dictionary distributed by Deaf Children Australia. In our observation sessions we observed that some parents used one or more Auslan signs (identified as such by a fluent user of Auslan), sometimes in conjunction with a spoken word. Examples included the signs for ‘baby’, ‘ball’, and ‘star’. Parents frequently indicated that they stopped using the signs that they had learned once their child started using spoken words; our observation data supported this.
Over the time period covering the ECI observations, families accessed some early intervention services for deaf or hard of hearing children. The services varied across locations and families in terms of frequency and content, with some services focusing on an auditory–verbal approach and others a total communication approach. Some families switched providers, or at times suspended the services, and a few accessed more than one. The data we have are not sufficient to quantify the hours of intervention services each family received.
Comparison data
To address the fourth and fifth research questions, ECI data collected from 375 children with NH were used for comparison. The children were aged in the range 4.5 to 40.2 months, mean = 16.4 months (sd = 9.3), with 48.8% male (n = 183). The data were collected at baseline in one session as part of another study, the Early Home Learning Study (EHLS), a cluster randomised controlled trial of a community-based parenting programme (see Hackworth et al., Reference Hackworth, Berthelsen, Matthews, Westrupp, Cann, Ukoumunne and Nicholson2017; Nicholson et al., Reference Nicholson, Cann, Matthews, Berthelsen, Ukoumunne, Trajanovska and Hackworth2016). The families recruited for the EHLS were, like those in the CI sample, from urban and rural locations and from across the socioeconomic spectrum. They lived in the same state as the majority of the CI sample. The ECI data were collected as part of the EHLS at baseline, before any intervention commenced.
Measures
CI sample
The Early Communication Indicator (ECI)
The ECI was used to collect data during 6-minute observation sessions of play between a child and familiar adult. The data collected comprised the child's use of gestures, nonword vocalisations, single words, and multiword utterances. For analysis, a weighted total ECI score was calculated following the ECI coding system: 1 was assigned for each gesture and each vocalisation, (i.e., prelinguistic communication), 2 for each single word (spoken or signed), and 3 for each multiword utterance. These values were then summed to create a growth-based total communication metric that reflects the reduction in gestures and vocalisations that occurs over time as children acquire more advanced spoken communication. Weighted total scores can be used to generate individual child growth relative to benchmark norms based on a sample of 5,883 children (Greenwood et al., Reference Greenwood, Walker and Buzhardt2011).
In the current research, six ECI sessions were conducted over a 15-month period. Details of the protocol and scoring are provided in the ‘Procedure’ section below.
Maternal education
Maternal education, classified into four levels, was used to investigate its impact on the children's early communication growth. The percentages for each category were: category 1: 16.5% of mothers had not completed high school; category 2: 19.8% had completed high school; category 3: 23.1% had undertaken some additional training; and category 4: 39.6% had a university degree.
Time to achieve consistent use of CIs
Time to achieve consistent use of the CIs was used in analysis of the CI data. This variable had four levels. Based on parent report about when during the day and in which activities their child used the CIs, and when they did not, time taken to achieve 90% usage was classified as (1) up to a week, (2) between 1 week and 3 months, (3) 3 to 6 months, and (4) 6 to 12+ months. The percentages in each category were 39.9% in category 1, 33.3% in category 2, 9.09% in category 3, and 15.15% in category 4.
NH data
For maternal education the breakdown was: category 1: 16.5% had not completed high school; category 2: 19.8% had completed high school; category 3: 23.1% had undertaken some additional training; and category 4: 39.6% had a university degree.
Procedure
CI sample
The first session was held shortly after the initial home visit, and the remaining five observations at approximately 3-monthly intervals thereafter. For 25 (76%) of the infants, the first ECI observation was conducted soon after implantation. Due to changes in planned surgical schedules, four infants received their CIs after their first ECI session, three infants after their second, and one after their third session. The ECI was administered by a trained ECI assessor in the family home following the standardised ECI protocol and using the standard set of toys (Greenwood et al., Reference Greenwood, Carta, Walker, Hughes and Weathers2006), a Fisher Price toy house, a few small objects that fit into the house (e.g., table, chair), and several Little People figurines. The toys were set up on the floor where they could be easily reached by both adult and child and both could have eye contact. The camera captured the behaviours of both the child and adult play partner. At the beginning of the session the adult was asked to interact with the child: to follow the child's lead during play, respond to the child's attempts to communicate, comment about the child's actions throughout, but not to ask too many questions (in order to give the child a chance to demonstrate their communicative ability). The same adult participated in all six sessions. Each session was timed and video-recorded for later scoring.
Coding was completed using the Eudico Linguistic Annotator (ELAN) editing program (https://tla.mpi.nl/tools/tla-tools/elan/). This allowed the coder to view the videos, listen to the audio, and record the use of each of the four behaviours on separate coding lines. Nonword vocalisations, gestures, single words, and multiword utterances in each session were coded according to the ECI coding definitions and guidelines (Walker & Carta, Reference Walker, Carta, Carta, Greenwood, Walker and Buzhardt2010; <https://igdi.ku.edu/eci/>). The definitions of each category are quite specific and scoring needs to be undertaken by qualified coders. To be coded as one of the four communication means, there needed to be an attempt by the child to communicate with the play partner. Nonword vocalisations are defined as nonword utterances, noting that crying and involuntary sounds (such as a sneeze) are not coded as nonword vocalisations. Gestures include a child's movements that are attempts to communicate with the partner (including giving, taking, pushing, and reaching and others). Gestures are distinguished from single words, which are defined as voiced or signed words, recognised and understood by the coder. Multiword utterances comprise two or more different words readily understood by the coder, but the utterance does not need to be grammatically correct. Total Weighted Communication Rate was calculated for each session for each observation.
Two researchers were certified to code the ECI observations. The videos were also coded by a fluent user of Auslan for any use of signs. Six of the 33 children in the CI sample used an Auslan sign (or more) during the six ECI sessions. One child used a total of 12 signs over two sessions, three children used one sign in one session, one used two signs in one session and another used four signs in one session. As indicated previously, Auslan signs were included in the single word count, following the ECI conventions.
Comparison data
Similar to the CI sample, ECI assessments for the children with NH were collected in the child's home by trained researchers following standardised protocols and using the standard set of toys. The familiar adult was the primary caregiver, the mother for 96.5% (362), the father for 2.4% (9), and another family member for 1% (4). All coding for the EHLS data was completed by researchers at the Juniper Gardens Children's Project. Maternal education was categorised into four levels in the same way as for the CI sample.
Analytic methods
To address our first research question, on associations between the four key communication elements, we used multivariate growth curve models in the multilevel modeling framework (Curran, Obeidat, & Losardo, Reference Curran, Obeidat and Losardo2010). The approach allowed us to examine the correlations of the means (i.e., intercepts) at different measurement occasions between two communication scores. It is superior to raw-data-based correlations analysis and less influenced by missing data because it tolerates different numbers of observations for individuals and accommodates unequal time intervals separating occasions (Raudenbush & Bryk, Reference Raudenbush and Bryk2002). In this analysis, the correlations between the four ECI key skill elements were estimated. Specifically, we examined the correlations between the estimated means of the prelinguistic elements (gestures and nonword vocalisations centred at 3 months post CI switch-on) and the linguistic elements (single words and multiword utterances, which were centred at 15 months post CI switch-on). The second research question was concerned with growth in the ECI weighted total rates for the CI sample. Controlling for child age in months at the first wave, a multilevel linear growth model was used to estimate the average and the individual growth rates of the communication scores across the six waves. A growth rate is also known as a linear slope, which presents the amount of change in the communication scores between waves. To address the third research question, we examined the effects of the covariates, gender, maternal education, and time to achieve consistent use of the CIs, on the child communication scores.
For the fourth research question, the ECI growth trajectories for the CI and NH samples were compared using a multilevel quadratic growth curve model. The NH sample was treated as the reference group; the unit of time was child's age in months, and for all comparisons age was centred at the mean age of 18 months. The same statistical strategy was used to compare each of the four elements between the two samples (i.e., using a multilevel quadratic growth model). In a quadratic model there are three major growth parameters: intercept, linear slope, and quadratic slope. The intercept represents the average ECI score across individuals at the mean age; the linear slope represents the average growth rate across the range of time; and the quadratic slope refers to the change rate in the linear slope across time. To address question 5, gender and maternal education were then included in the model as moderators. Specifically, we examined the two-way interactions of sample by gender or maternal education, and three-way interactions of sample by linear slope (or quadratic time) by gender or maternal education.
The statistical program Mplus (version 7.4; Muthén, & Muthén, Reference Muthén and Muthén1998–2012) was used to estimate the multivariate growth curve models in the first analysis, and the R software package (version 3.4.2; R Core Team, 2017) was used for multilevel grow curve modelling in the other analyses.
Results
CI sample
Prelinguistic and linguistic means of communication
Table 1 shows the mean scores for the ECI weighted total rate and the four key skills at each of the six waves of data collection for the CI sample. Growth in weighted total rate for each child with CI is shown in Figure 1. To explore associations between the prelinguistic and linguistic skills for the CI sample, multivariate growth curve models were used to estimate the correlations between the six pairs of elements. As shown in Table 2, the prelinguistic skill elements at 3 months post switch-on correlated more strongly with single words at 15 months post switch-on than with multiword utterances. Gestures showed a stronger correlation with single words than did nonword vocalisations.

Figure 1. ECI weighted rate: individual ECI growth trajectories for CI sample - estimated (n=33). The bold line indicates the mean growth rate. Numbers indicate child IDs.
Table 1. CI sample (n = 33): Means, SDs, and range of scores for ECI total rate (weighted) and the four skill components by session
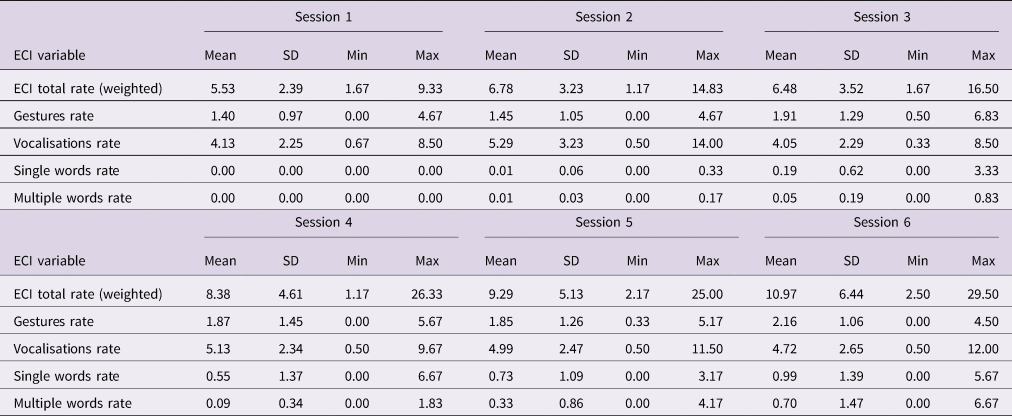
Notes. All ECI variables are expressed as a rate per minute: vocalisation and gestures scores = 1, single words are weighted as 2, and multiword utterances as 3.
Table 2. Estimated means for correlations between prelinguistic and linguistic elements for CI sample (n = 33)

Growth trajectories
The second analysis was conducted on the data shown in Table 1 in order to determine the expressive communication growth trajectories of the CI sample. As shown in Table 3, when controlling for start age, the growth rate was significant (estimate = 1.02, SE = 0.23, p < .001). The individual growth rates for each child in the CI sample and mean growth rate are illustrated in Figure 1.
Table 3. CI sample (n = 33): estimated growth rate: ECI weighted total rate

Notes. All ECI variables are expressed as a rate per minute: vocalisation and gestures scores = 1, single words are weighted as 2, and multiword utterances as 3.
Impact of covariates
To determine whether gender, maternal education, or time to consistent CI use had a significant effect on the intercept and slope of the growth trajectory for the CI sample, the analyses were repeated with these three variables included. The reference groups were: female gender, maternal education category 1 (not completed high school), and time-to consistent use category 1 (within a week). The results showed no significant effect of gender or maternal education for the weighted total communication score, nor for any of the four components. However, for time to consistent use, one significant effect on the intercept was found. For gestures, there were significantly more gestures used if a child had consistently used their CI within a week of switch-on (category 1) compared to between a week and 3 months (category 2) (estimate = 0.77, SE = 0.26, t = 0.299, p = .006). No other results for time to consistent CI use were significant.
Comparison of CI and NH samples
Growth trajectories
The means, SDs, and range of scores for the ECI key skills for the CI sample are shown in Table 1 and those for the NH sample in Table 4. Figure 2 illustrates the estimated growth curves for both samples. As indicated in Table 5, for the weighted total communication rate, a significant difference in linear growth rate was found between the CI and NH samples (–0.350, SE = 0.055, p < .001). This result implies that, on average, the children with CIs had a significantly slower growth rate than those in the NH sample. However, the differences in intercept and quadratic slope of the two samples were not statistically significant (see Table 5). That is, the mean weighted total ECI scores at 18 months of age and the changes in quadratic slopes did not differ significantly between the two samples.

Figure 2. ECI weighted rate: growth curves for the CI sample (n=33) and the EHLS sample (n=375).
Table 4. EHLS sample (N = 375): means, SDs and range of scores for the ECI
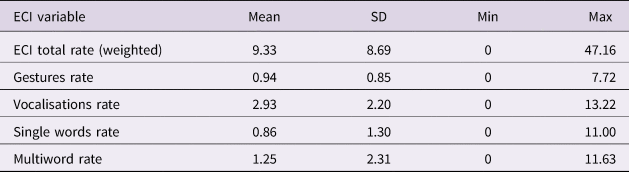
Notes. All ECI variables are expressed as a rate per minute: vocalisation and gestures scores = 1, single words are weighted as 2, and multiword utterances as 3.
Table 5. Comparison between the two samples: ECI weighted totals for each component of the ECI

Notes. The first three rows represent the intercept (centred at 18 months), linear slope, and quadratic slope for the NH sample. The last three rows represent the differences in intercept, linear slope, and quadratic slope between the CI and NH samples. All ECI variables are expressed as a rate per minute: vocalisation and gestures scores = 1, single words are weighted as 2, and multiword utterances as 3. NH used as the reference group for the differences (Diff).
The group similarities and differences across the four key skill elements of the ECI are also shown in Table 5. For gestures (see Figure 3A), the intercept of the two samples was found to be significantly different (0.809 responses per minute, SE = 0.116, p < .001). That is, at 18 months the children with CIs used 0.809 more gestures per minute than the children in the NH sample. A significant difference between the samples in linear growth rate for gestures was also found (0.030, SE = 0.010, p = .003), implying that, on average, the children with CIs had a more rapid growth rate than the NH sample. No significant difference was found in quadratic slope.
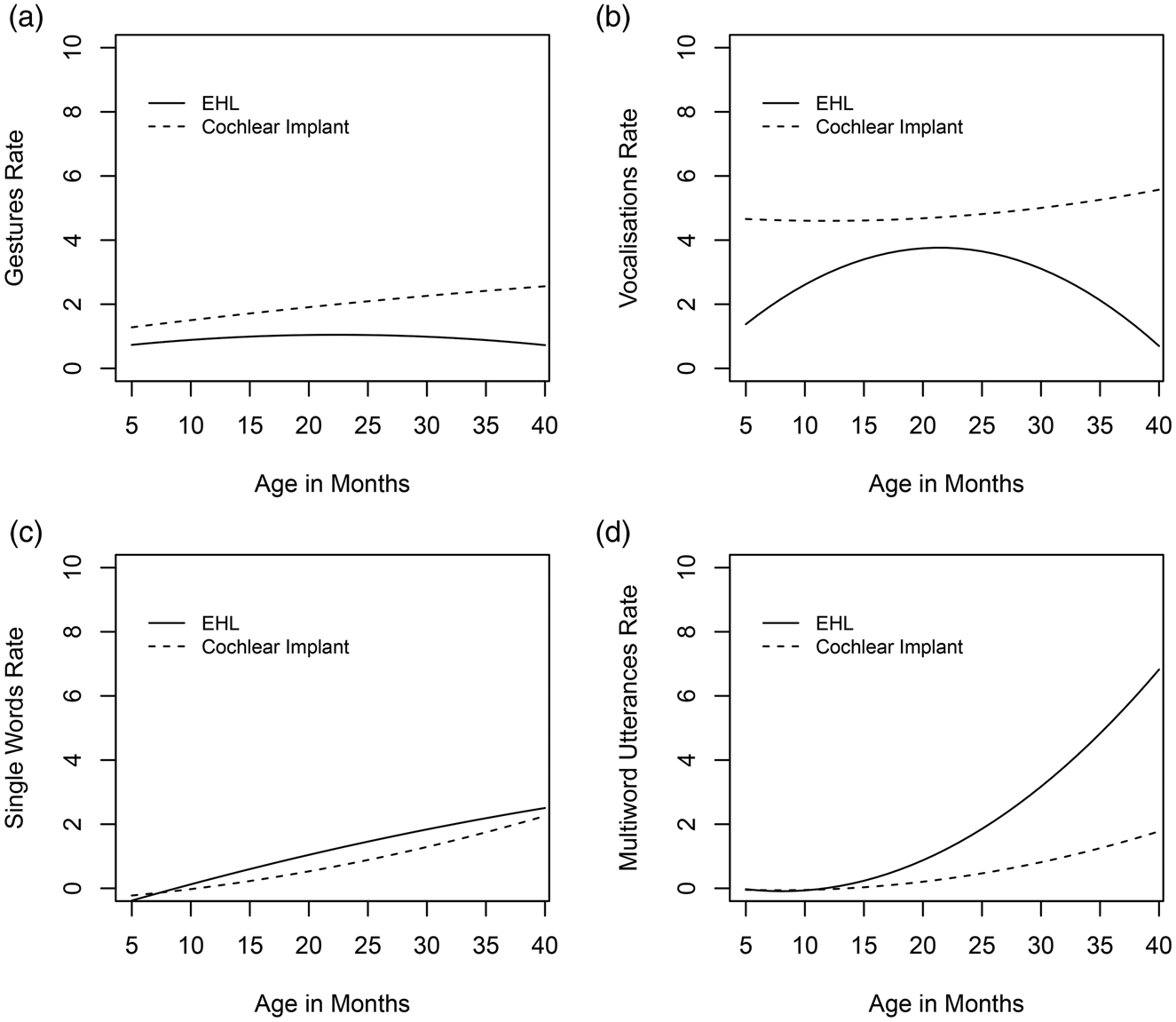
Figure 3. Similarities and differences across the four key skill elements of the ECI for the CI sample (n = 33) and the EHLS (n = 375). A = Gestures; B = Vocalizations; C = Single Words; D = Multi-word Utterances.
For nonword vocalisations (see Table 5 and Figure 3B), significant differences were found in both intercept and quadratic slope, but not in linear slope. The intercept difference was 0.978 nonword vocalisations per minute (SE = 0.277, p < .001), implying that the children with CIs used about one vocalisation more per minute than children in the NH sample at 18 months of age. The difference in quadratic slope of nonword vocalisations per minute was 0.010 (SE = 0.002, p < .001). Similar to the ECI's normative sample (Greenwood et al., Reference Greenwood, Walker and Buzhardt2011), the children in the NH sample had a decreasing slope of nonword vocalisations per minute over time, while those with CIs had an increasing slope.
Next, the groups were compared on single word use (see Figure 3C). Significant group differences were found for the intercept (–0.472, SE = 0.130, p < .001) and the linear slopes (–0.026, SE = 0.011, p = .019), but no significant difference was found for quadratic slope. In other words, the number of single words used by the children with CIs was lower than that for the NH group at 18 months of age, and there was also a slower average growth rate, but the acceleration rate (quadratic slope) was not significantly different between groups.
For multiword utterances (see Figure 3D), significant differences were found in all three growth parameters (i.e., intercept, linear, and quadratic slopes). The children with CIs used fewer than the NH children at 18 months of age (–0.467, SE = 0.195, p = .016). They also had a slower average growth rate, and a slower acceleration (–0.100, SE = 0.015, p < .001, for linear slope; and –0.005, SE = 0.001, p < .001, for quadratic slope).
Interaction between sample and gender or maternal education
The analyses between the two sample were repeated with the variables gender and maternal education included. The results showed no significant effect of gender. Maternal education had more influence on the ECI growth rate for the CI sample than for the NH sample. Specifically, in the CI sample, the children whose mothers completed a university degree (category 4) showed significantly faster ECI score growth rate (i.e., linear slope) than the children whose mothers did not complete high school (category 1) (estimate = 0.39, SE = 0.18, t = 2.10, p = .036). However, in the NH sample the difference was not as marked as in the CI sample. A similar result was found for the use of single words. The growth rate for single words for the CI group was influenced more by maternal education than was the growth rate of the NH group (estimate = 0.011, SE = 0.04, p = .003). In addition, the impact of maternal education at age 18 months was even more evident for gestures. When maternal education was higher than category 1, children in the CI group used significantly more gestures at 18 months than did the NH sample (category 2: estimate = 0.92, SE = 0.39, p = .019; category 3: estimate = 0.87, SE = 0.39, p = .026; category 4: estimate = 1.05, SE = 0.36, p = .004).
Discussion
The current study provided a unique opportunity to explore how early communication grows over time for infants and toddlers (in Australia) who recently received CIs, how this growth compares to that of a cohort of similar children with NH, and potential moderators of the growth. Novel to the study was the use of the ECI, with an advantage being the use of direct observation of a child in the home with a familiar adult. Observation allows for identification of the frequency of preverbal and verbal measures of communication over time, and there is an advantage in having the same communicative partner across sessions to help keep the context similar. The availability of the existing NH data allowed for comparison with children drawn from similar geographic regions.
The results of the analyses showed that the use of prelinguistic means of communication by the CI group was more strongly correlated with single word use than with multiword utterances. Moreover, the use of single words was more strongly associated with gestures than with nonword vocalisations. This association between gesture use and single word use is supportive of a body of research findings reported in the literature on children's communicative development (e.g., Goldin-Meadow, Reference Goldin-Meadow2009, Reference Goldin-Meadow2014). Words are symbols for objects, attributes, and actions, and gestures can function similarly. Gesture use predicts vocabulary in children with NH and has been associated with subsequent single word use for children with mild to profound hearing loss (Roberts & Hampton, Reference Roberts and Hampton2018). It has also been identified as a predictor of vocabulary for young children with CIs (Bavin et al., Reference Bavin, Sarant, Leigh, Prendergast, Busby and Peterson2018). Thus, the promotion of gesture use cannot be assumed to be detrimental to the onset and early development of spoken words for children with CIs.
While the results showed growth in communication skills across the six observation sessions for the CI sample, the analysis of the total ECI scores showed slower linear growth for the CI group than for the NH group. This finding is consistent with having a congenital hearing loss and the resulting delay in accessing auditory input. Fagan, (Reference Fagan2014) reported that, within a few months of using CIs, children were better able to process the speech they heard. Auditory perception affects vocalisation types (Stoel-Gammon & Otomo, Reference Stoel-Gammon and Otomo1986; von Hapsburg, & Davis, Reference von Hapsburg and Davis2006), and with improved auditory perception a flow-on effect in the development of verbal communication can be expected.
Past research has shown a rapid growth in communication skills for children post implant (e.g., Niparko et al., Reference Niparko, Tobey, Thal, Eisenberg, Wang and Quittner2010). In the current study, progress post CI switch-on was found; the rate of use of nonword vocalisations and gestures was greater for the CI group than for the NH group. That is, more of these two components were used per time interval in the CI group. In addition, their gestures and vocalisations increased over time as the children processed more of the linguistic input. The CI group had an increasing slope of nonword vocalisations per minute while the NH group had a decreasing slope as their verbal communication skills developed, with words becoming more frequent. Greenwood et al. (Reference Greenwood, Walker, Buzhardt, Howard, McCune and Anderson2013) reported a similar finding for a sample of children without any identified disabilities; vocalisations increased to 18 months before decreasing as words replaced vocalisations. Thus, the NH group in the current study followed the typical developmental pathway to language, progressing from communicating with prelinguistic means to communicating with words and then combined words.
More single words and multiword utterances were produced by the NH sample overall. The CI group was only just beginning to combine words. In the final session the total number of multiword utterances ranged from 0 to 40, with only 14 children producing one or more, and only four of these children produced more than 10. Thus, the CI group was less advanced than the NH group. Analysis of individual growth rates over further sessions in follow-up research would permit examination of whether those children who showed faster rates of growth in their early communicative development were more advanced in language development than those whose growth rate was slower.
Child gender, one of the potential influencing factors included, did not have a significant impact on the communicative growth of the children with CIs. Gender differences in young CI samples reported in previous research has frequently measured vocabulary based on parent report, or early language structures. For example, Cuda et al. (Reference Cuda, Murri, Guerzoni, Fabrizi and Mariani2014) used a parent report vocabulary checklist with children with CIs at 36 months of age. Our output measure was based on early means of communication, non-linguistic and early words, used in play sessions at a younger age. Thus, some differences in findings about gender differences may depend on the measure used and nature of the data. Gender differences might become evident in our sample when the children's vocabularies are more developed. In Geers et al. (Reference Geers, Moog, Biedenstein, Brenner and Hayes2009), for example, the girls in the CI sample (aged eight to nine years) were advantaged over boys, in both vocabulary and language measures.
Maternal education impacted significantly on the CI results for both gesture use and word use in the current study, supporting past research findings that have shown an impact of parental education on children's language, including children with CIs and older than those in the current study (e.g., Cuda et al., Reference Cuda, Murri, Guerzoni, Fabrizi and Mariani2014; Sarant, Harris, Bennet, & Bant, Reference Sarant, Harris, Bennet and Bant2014). Interactions between an infant and parent (and others) provide contexts for language development (e.g., Levine et al., Reference Levine, Strother-Garcia, Golinkoff and Hirsh-Pasek2016; Wu, & Gros-Louis, Reference Wu and Gros-Louis2014; Hoff, Reference Hoff2003). When others respond to a child's gestures and vocalisations, they provide an opportunity for promoting further communicative interactions, and thus introduce the child to turn-taking as well as words and structures in which the words occur. As shown from past research, richness of the language input, in terms of both style of interaction and content, impacts on young children's communicative development; higher levels of socioeconomic status and maternal education are associated with richness of input and positive effects on a child's early language. Thus, important for early intervention programmes is identifying those who might need additional assistance to develop skills that have the potential to help facilitate their children's emerging communicative development, from prelinguistic to linguistic means.
Time to achieve consistent use of the CIs also had an impact on the results of the current study. For children achieving consistent use within the first week post switch-on, the ECI weighted total rate was significantly greater than for those who took up to 3 months, but no other significant differences were found between the categories. While CIs do not provide normal hearing, they do provide access to the auditory input, and an earlier opportunity to use auditory input to identify the sounds of the input language for infants implanted with CIs than for children implanted at an older age. Our results indicate an advantage for early communicative development if children are strongly encouraged to use their CIs consistently following switch-on. Variability in growth rates are likely when it takes longer to achieve consistent CI use. The latter may result from some initial resistance to unaccustomed auditory input and to wearing new equipment, or parents may be uncertain as to what constitutes ‘optimal use’ in the period immediately following implantation.
A strength of the study was the prospective longitudinal design (rather than cross-sectional), which allowed for analysis of growth in a child's communication skills. In addition, the children with CIs were implanted over a narrow age-range and at a very young age. As a consequence, their stage of development overall was not as wide is in many other studies with CI samples, so providing an advantage for comparing their communicative development. With a wider age-range, the older participants would have had more life experiences on which to draw in communicating with others.
A larger sample of children with CIs would provide more power to identify factors that moderate the impact of CIs on children's early communicative development and later language. The inclusion of other potential influencing factors could help further our understanding about children's communicative growth and the interactions amongst moderating variables in the early period following CI switch-on. Research findings have shown that both environmental and genetic factors help to explain children's language development (Dale, Tosto, Hayiou-Thomas, & Plomin, Reference Dale, Tosto, Hayiou-Thomas and Plomin2015; Fernald et al., Reference Fernald, Marchman and Weisleder2013; Ramirez-Inscoe, & Moore, Reference Ramirez-Inscoe and Moore2011), and, as argued by Pisoni and colleagues (Pisoni, Cleary, & Tobey, Reference Pisoni, Cleary, Geers and Tobey1999; Pisoni, Kronenberger, Chandramouli, & Conway, Reference Pisoni, Kronenberger, Chandramouli and Conway2016), some of the variability in language outcomes reported for users of CIs, even when implanted at an early age, may be explained by higher-level central processes (perception, attention, learning, and memory). Thus, including memory and attention measures in future research might assist in helping to identify the children who are likely to go on to achieve age-expected scores on standard tests and those who are not − information that would be valuable in guiding the allocation of resources and services.
The inclusion of additional language assessments (e.g., the Preschool Language Scale), and parental reports of children's communication during daily routines, in addition to direct observation, might add to understanding the developmental pathways to language outcomes for children who receive CIs in infancy. Following up the current sample could provide information about whether any of the children who showed slower growth in communication skills in the early years caught up to age expectations in language assessments in later years. Such information could help in identifying those children who are likely to need additional resources to assist them in developing good language skills, although, from studies with children with NH, it is clear that, while some children with late onset of oral vocabulary (late talkers) continue to be delayed in language development, others resolve (e.g., Rescorla & Dale, Reference Rescorla and Dale2013). In contrast, some who appear to be on track for oral language development initially may show problems in language later (e.g., Ukoumunne et al., Reference Ukoumunne, Wake, Carlin, Bavin, Lum, Skeat and Reilly2012), sometimes at the onset of formal schooling.
Despite a wide range of individual differences among the young CI population, understanding general patterns of expressive communication growth over time for children who recently received a CI can help to inform intervention delivery and to establish expectations for parents and caregivers. The children with CIs in the current study were less advanced than the NH group (controlling for age) in their progression from prelinguistic to linguistic means of communicating; however, the results suggest a similar pathway, and for some components there was faster growth. Further research investigating factors that influence the progression of early communication skills in very young children with CIs and later outcomes can help to extend our understanding of variability in their paths of development.
In conclusion, the findings of the current research have clear implications for early intervention programmes. Children, whether NH or CI recipients, use prelinguistic means to communicate initially, with their early gestures providing a bridge to verbal communication. The results of the current study illustrate the importance of fully informing parents of infants with CIs about ways of promoting communicative exchanges with their child. When children can communicate their needs and desires and draw the attention of others to something, it can encourage social interactions with exposure to linguistic input, whether in the oral or visual mode, and to experience of language routines in social contexts. By encouraging parents to respond to and encourage their child's early means of communication, early intervention programmes can assist parents of infants and toddlers with CIs in supporting their child's oral language development.
Acknowledgements
Many thanks to the families who participated so willingly, the staff who assisted in recruitment at the Cochlear Implant Clinics, and the research assistants, in particular, Madeline Armstrong, Elena Badcock, Elizabeth Button, Jess O'Reilly, and Katherine Landy. For the cochlear study, human ethics approval was obtained from La Trobe University HREC (11-014), the Royal Victorian Ear and Eye Hospital HREC (11/1005H), The Sydney Local Health District – RPAH Zone Ethics Committee (X11-0302 and HREC/11/RPAH/468), Queensland Children's Health Services HREC (HREC/11/QRCH/151), Mater Health Services HREC (Protocol Ref No.1850C), The Adelaide Women's and Children's Health Network HREC (HREC/12/WCHN/35), and the Victorian Government Department of Education and Early Childhood HREC (2011_001226). For the EHLS, human ethics approval was obtained from the Victorian Government Department of Education and Early Childhood Development (HREC 08/10).








