


Introduction
Ear lobule deformities are more commonly acquired following trauma. Complete agenesis of the lobule is documented but is very rare. The ear lobule is an important reference point for symmetry of the face and its loss causes an obvious aesthetic abnormality. Although relatively uncommon in the UK, many cases occur overseas, particularly in India, where amputation occurs as part of ritual punishment.Reference Rao and Rao1
An Ovid Medline search was performed from inception to December 2006. The medical subject headings ‘ear’, ‘reconstructive surgical procedures’ and ‘ear deformities’ were searched for similar cases. Although several methods for reconstruction of an ear lobule have been described in the literature, our search revealed this to be a novel report of a bi-lobar post-auricular flap repair.
Case report
A 27-year-old West Indian woman was referred with a history of having lost the lower part of her left ear lobule during childhood. The exact mechanism of injury was not known to the patient who had no recall and who could give no details of the trauma. She had subsequently tried to disguise her disfigurement by having the ear pierced and by wearing a large earring. However, the pinna had become infected and the remaining tissue had then torn resulting in an unsightly deformity of the lower part of the left ear.
She had been diagnosed as having type 2 diabetes three years prior to her referral and there was a past history of asthma. She had otherwise been fit and well. Examination showed an almost complete absence of the lobule on the affected side with split skin immediately superior to this (Figure 1). The right ear appeared normal with no evidence of any hypertrophic reaction or keloid as a result of her previous ear-piercing. A soft tissue X-ray of the contralateral ear was performed which was then sterilised to act as a template for the reconstruction. Under general anaesthetic the post-aural skin was infiltrated with local anaesthetic and a pedicled flap was elevated based on the post-auricular fold. The lower part of this flap was fashioned to provide a new lobule with skin cover on both surfaces (Figure 2). This was sewn into position using 5/0 Vicryl Rapide having freshened the edges of the lower part of the pinna. The pedicle was covered with Silastic® sheeting and the post-aural area buttressed with a dental roll prior to application of a mastoid dressing.

Fig. 1 Pre-operative appearance.
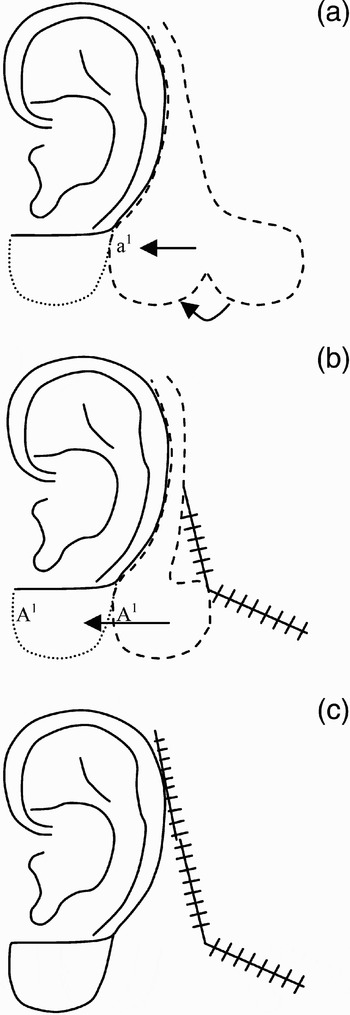
Fig. 2 (a) Post-auricular bi-lobar flap created. Leading edge (a) everted and sutured onto (a1). (b) Pedicled flap (A1) advanced. Skin incision closed. (c) Division of pedicle and closure of remaining incision.
Two weeks following the initial surgery the pedicle was divided and returned to the underlying scalp. The result at three months is shown in Figure 3.

Fig. 3 Post-operative appearance at three months.
Discussion
Reconstruction of a deficient ear lobule tends to be very successful due to the presence of a strong arterial supply through branches of the post-auricular and occipital arteries. Some authors have described flaps based on named branches of these vessels,Reference Krespi, Ries, Shugar and Sisson2, Reference Park and Chung3 but these larger flaps seem to be more important in auricular reconstruction where a much larger volume of tissue reconstruction is required. Many different types of ear lobule repair have been documented in the past. These broadly fall into three categories: (Reference Rao and Rao1) pre-auricular flap reconstruction,Reference Kumar and Shah4, Reference Mohan, Appukuttan and Srinivasan5, Reference Savaci, Tosun and Hosnuter6 (Reference Krespi, Ries, Shugar and Sisson2) post-auricular flap reconstruction,Reference Krespi, Ries, Shugar and Sisson2, Reference Park and Chung3 and (Reference Park and Chung3) tissue expansion using a tubed flap or Zulu method.Reference Sarig, Ben-Bassat, Taube, Kahanowitz and Kaplan7, Reference Cort and Fayman8 The main advantage of a post-auricular approach is that it avoids pre-operative tissue expansion and provides an aesthetically appealing scar that is hidden in the post-auricular skin crease and hair line.Reference Alanis9 Other previously documented post auricular flaps have only reconstructed one surface of the ear lobule and have required a split skin graft for the opposite surface.Reference Savaci, Tosun and Hosnuter6
The bi-lobar post-auricular skin flap used in this case avoids problems associated with other forms of repair and has the advantage of a well-hidden scar with the donor site providing skin of similar consistency, thickness and pigmentation. There is direct closure of the donor site and as a result hospitalisation and post-operative care are kept to a minimum.



