



Radiation emergencies, either intentional or unintentional, pose a real threat to the United States. Types of radiation emergencies include a nuclear event involving the explosion of a nuclear weapon or improvised nuclear device; detonation of a radiological dispersal device, colloquially known as a “dirty bomb”; a radiological exposure device, which is a hidden sealed source releasing radiation; nuclear power plant accidents; and accidents occurring in the transportation of radioactive materials. Concerns about the use of nuclear warfare against the United States—originally dating back to the Cold War—are now increasing. The National Security Strategy states that the American people face no greater or more urgent danger than a terrorist attack using a nuclear weapon.1 In a 2017 announcement, the Science and Security Board warned, “World leaders are failing to act with the speed and on the scale required to protect citizens from the extreme danger posed by climate change and nuclear war. The probability of global catastrophe is very high, and the actions needed to reduce the risks of disaster must be taken very soon.”2 Given the current intensifying geopolitical tensions between countries in possession of nuclear weapons and radiological dispersal devices, the need for a health care workforce with the specific knowledge, skills, and abilities to respond to radiation/nuclear public health emergencies of international concern is of critical importance. Plans for US medical response have been described previously,Reference Coleman, Hrdina and Bader3–Reference Hrdina, Coleman and Bogucki5 and, in 2016, Burkle and DallasReference Burkle and Dallas6 proposed a framework for developing a nuclear global health workforce.
Adding to the risk of a radiation event, according to Ready.gov, 3 million Americans live within 10 miles of a nuclear power plant,7 putting them directly within the plume exposure pathway should there be an accidental or intentional radiation or nuclear release. Potential exposure from the transportation of nuclear waste via rail, plane, and highway threatens communities across the United States. In any of these potential events, nurses will be critical to an effective response to the resulting public health emergency.8–Reference Karam and Veenema11 Schools of nursing (SONs) are responsible for developing a competent nursing workforce prepared to assess a population’s public health emergency needs and respond to an event according to the circumstance.12, 13
Study Purpose
The purpose of this study was twofold: to explore the current capacity of US SONs and nurse educators for preparing the next generation of the nursing workforce for preparedness and response to radiation/nuclear events resulting in a public health emergency and to broadly examine perceptions of risk. The research team established a partnership with the American Association of Colleges of Nursing (AACN) and the Organization for Associate Degree Nursing Schools and Programs (OADN) to conduct this study. Specifically, this research project considered the following:
1. What content (relevant to knowledge, skills, and abilities) is being taught to students regarding preparedness and response to radiation emergencies / nuclear events?
2. Do schools/programs of nursing have the faculty expertise to teach this content?
3. How do schools/programs of nursing perceive risk of a radiation emergency or nuclear event?
4. Do schools/programs of nursing have existing radiation emergency / nuclear event response plans?
5. Do schools/programs of nursing test or exercise their radiation/nuclear response plans?
6. What would motivate US SONs to include content on radiation emergency/nuclear events in their curricula?
METHODS
This study employed a cross-sectional survey administered in May 2018 to a purposive sample of administrators and faculty at AACN and OADN member schools. Participants were asked to click on a web link to access a multi-item survey in Qualtrics Research Suite Software. The survey contained 26 multiple choice questions and 2 open-ended questions divided into 4 separated sections (eg, demographic data, radiation content and faculty expertise, radiation response plans, and perception of risk). Participation was voluntary, responses were anonymous, and all surveys included information detailing the purpose of the study and contact information for the research team. Study participants were provided the option to identify the zip code of their school of nursing. Invitations to participate in the study were sent via email to member schools and faculty by AACN (880 surveys) and OADN (2421 surveys). The email invitation was sent out 3 times by OADN and twice by AACN over a period of 3 weeks.
Survey Development
The radiation nuclear survey is a rapid, self-administered questionnaire. The survey’s questions were derived from previously published studiesReference Veenema, Walden and Feinstein14, Reference Charney, Lavin and Bender15 addressing workforce development for radiation and nuclear events and input from subject matter experts in radiation medicine and nursing and nuclear emergency preparedness. The survey was pretested by 5 graduate nursing students to ensure that the questions were clearly articulated and that the response options were relevant, comprehensive, and mutually exclusive.
Ethical Considerations
This study and the supporting survey instrument were approved by The Johns Hopkins University Institutional Review Board and were reviewed and approved by AACN and OADN leadership prior to distribution.
Analysis
Survey response data were analyzed using applicable data analysis features available in Qualtrics Research Suite Software. A summary report was generated using the Reports feature and was exported in comma-separated values format to Microsoft Excel for data analysis. The following 2 survey questions offered respondents the opportunity to provide open-ended responses: “If the total number of hours spent on radiation/nuclear content is 1 hour or less, why is this not being taught?” and “What would it take for your school to add radiation/nuclear content to your curriculum?” Three members of the research team (T. G. Veenema, S. Schneider-Firestone, R. P. Lavin) conducted a sequential thematic assessment and analysis of the narrative data. Responses were independently coded and categorized in Microsoft Excel. Team members then met to discuss and compare their findings in order to determine the major themes.
Perceived Risk Versus Actual Risk
For the study participants who provided their zip code, we analyzed whether or not they were aware of their proximity to nuclear power plants. In order to interpret these results within the context of perceived risk versus actual risk, and to more accurately quantify the total relative risk to these schools resulting from the presence of existing sources of radiation hazards, we expanded our model to also include proximity to nuclear waste and nuclear research facilities. We also looked at the proximity of fault lines to these sites whereupon seismic activity could contribute to structural damage resulting in the release of radiation. Within the framework of all-hazards preparedness, this information would be part of an emergency operations plan at the local, state, regional, or tribal area.
Determination of Nuclear Facility Locations
In order to determine the proximity of SONs to nuclear power sites, it was necessary to obtain the physical addresses of both nuclear power reactors and nuclear research and test reactors. A list of nuclear power reactors is publicly available on the US Nuclear Regulatory Commission website.16 An internet search was conducted to obtain the street address, state, and zip code for each of the 99 active nuclear power reactors. Additionally, there are 31 sites operating research/test reactors in the United States. For the purpose of this study, we included the 5 research/test sites that generated the highest amount of power: National Institutes of Standards and Technology (20 000 kW); University of New Mexico (10 000 kW); Massachusetts Institute of Technology (5000 kW); University of California, Irvine (2300 kW); and Rhode Island Atomic Energy Commission (2000 kW). A list of nuclear research and test reactors was obtained from Data.gov, which contains location information (city and state) for 31 sites.17 Finally, high-level nuclear waste sites were also mapped. Additional location information, including street address and zip code for each of the sites, was collected from an internet-based mapping service.17
Geographic Data
The dataset used for this investigation consists of georeferenced digital layers, with zip code as the most detailed spatial reference level, retrieved from the publicly available US Census Bureau 5-Digit ZIP Code Tabulation Area (Census 2010) cartographic boundary files.18 Analyses were performed at the zip code level to match the data provided by survey respondents. The study area consisted of all zip codes within the United States, which consisted of 33 144 zip codes at 1:500 000 resolution.
Zip code data were imported into Esri ArcGIS v 10.5.1. Analyses were conducted in 3 steps: (1) joining national survey data to zip code polygons via a data join based on GeoID number, (2) identifying and geocoding national nuclear power facilities and nuclear research sites with addresses listed publicly on the internet, and (3) analyzing respondent characteristics within 50 miles of a nuclear site (research or power plant).
Emergency Planning Zones
To facilitate a preplanned strategy for protective actions during an emergency, the US Nuclear Regulatory Commission designates 2 emergency planning zones (EPZs) around each nuclear power plant (plume and ingestion). The exact size and shape of each EPZ is a result of detailed planning, which includes consideration of the specific conditions at each site, unique geographical features of the area, and demographic information.19 The research team elected to use the ingestion exposure pathway EPZ, which has a radius of about 50 miles from the reactor site. This EPZ is designed to avoid or reduce the dose from potential ingestion of radioactive materials. These actions include a ban of contaminated food and water.19 Therefore, in the data analysis, a 50-mile buffer area was placed around each geolocated nuclear plant / research site. The Selection by Location tool was used to select zip codes of survey respondents living inside the buffer area. Analyses were run in relation to the answers from respondents in these zip codes to survey questions regarding curriculum on radiation, hours taught, and knowledge of proximity to nuclear sites (within 50 miles).
Additional information regarding fault lines,20 as well as 1-year 2018 minor and moderate seismic hazard forecasts,Reference Petersen, Mueller and Moschetti21 were obtained, and the corresponding shapefiles were imported into ArcMap for location comparison to nuclear sites as previously mapped.
Federal Emergency Management Agency Regions
To maintain consistency with the National Response Framework and Federal Emergency Management Agency (FEMA), the authors elected to use the FEMA regions for organizing and mapping comparisons. Once a presidential disaster declaration has been issued, FEMA can provide assistance under the Stafford Act (Robert T. Stafford Disaster Relief and Emergency Assistance Act, Public Law 100-707). To help coordinate responsibilities, FEMA’s organizational structure includes 10 regional offices, each headed by a regional administrator.22 Each of FEMA’s regional offices maintains a Regional Response Coordination Center. The Regional Response Coordination Centers are 24/7 coordination centers that expand to become an interagency facility staffed by Emergency Support Functions in anticipation of a serious incident in the FEMA region or immediately following an incident. Operating under the direction of the FEMA regional administrator, the Regional Response Coordination Centers coordinate federal regional response efforts and maintain connectivity with state emergency operations centers, state fusion centers, federal executive boards, and other federal and state operations and coordination centers that have the potential to contribute to development of situational awareness. Organizing the data by FEMA region increases the data’s relevance to emergency planners and managers.
RESULTS
Of the 3301 individuals who received surveys, 790 responded and 679 completed the survey. The survey response rate was 71.5% (AACN member schools) and 2.1% (OADN member schools and faculty), for an overall response rate of 20.6%. All survey questions were optional for this anonymous survey, and 605 respondents voluntarily elected to provide the zip code location of their school (Figure 1).

FIGURE 1 Points Pictured on This Image Represent the Total Number of Nationwide Survey Respondents (n = 605) Who Provided a Zip Code and Could Be Geocoded With ESRI ArcMap v. 10.5.1
Nursing School Program and Survey Respondent Role
Respondents were asked to indicate all nursing degree programs offered by their SON. Respondents could select more than 1 answer; 1681 selections were made for this question. Respondents indicated that their SONs offered the following programs:
associate degree 5.7% (95)
baccalaureate degree 35.0% (589)
master’s entry into practice degree 12.8% (215)
graduate degree 31.7% (533)
professional certificate 14.8% (249)
Respondents were asked to indicate their role in the nursing program (Table 1).
TABLE 1 Role of Survey Respondent at School of Nursing

Radiation/Nuclear Emergency Preparedness Content
Survey respondents were asked the total number of hours spent teaching radiation/nuclear emergency preparedness in their school’s curriculum. The results reveal that 75.1% of respondents answered that they teach either 0 or ≤1 hour of radiation/nuclear emergency preparedness content in their SON curriculum (Figure 2). Respondents who spent 0 or ≤1 hour on radiation/nuclear content in their curriculum were then asked why it was not being taught. Respondents could select multiple answers. The primary reasons cited were “inadequate time in the curriculum” (26.4%), “topic not mandated in BS or MS Essentials document” (18.8%), “topic not mandated by State Board of Nursing” (14.3%), “no qualified faculty to teach” (11.5%), and “no perceived risk of this type of event for our area” (10.4%).

FIGURE 2 Total Number of Hours Spent Teaching Radiation/Nuclear Emergency Preparedness
Thematic analysis of the 168 open-ended responses revealed that respondents indicated that “it never occurred to them to teach radiation/nuclear content” (20.7%); respondents “were not sure why their school did not teach radiation/nuclear content” (22.6%), “they teach other disaster preparedness but not this topic specifically” (12.8%), or “they believe it is taught elsewhere on campus” (12.6%). Nearly 1 in 3 respondents (31.3%) indicated that “this topic is not relevant to their school,” “there is no perceived risk of this type of event in their area,” or “the topic is not relevant to nurses.”
Survey respondents indicated that certain circumstances would warrant including content in their curricula to address nursing workforce preparedness to respond to a radiation or nuclear emergency (Figure 3). When asked “what would it take for your school to add radiation/nuclear content to your curriculum?” respondents said “course content developed by experts made available for free to schools to adopt” (18.0%), “a requirement added to Essentials for BSN, MSN education” (17.7%), and “the NCLEX [National Council Licensure Exam] included questions specific to radiation/nuclear emergencies” (17%). Also of note, respondents said that they would add this content if it was “mandated by SON accrediting bodies” (15.4%), it was “mandated by their state board of nursing” (13.2%), and “funding was available to develop course content and course faculty” (10.5%). Interestingly, only 4.8% of respondents stated that “a radiation/nuclear event occurs on US soil” would be required for them to include the content in their curriculum. In the 71 open-ended responses under “other,” respondents said that they would add this content to the curriculum if they “had more information and/or an awareness was created on the need for the topic” (16.9%) or if they “had justification or evidence that this content should be a priority and thus included” (12.7%).

FIGURE 3 What Would It Take to Add Radiation/Nuclear Emergency Preparedness to the Curriculum?
The amount of time that SONs spend educating students on skills and competencies that they would be expected to perform independently of other health professionals in the event of a radiation or nuclear emergency was identified (Figure 4). Respondents indicated that the following relevant topics were covered in ≤1 hour, or not covered at all (with percentage of respondents who answered that question):
preparedness and training of nurses for a nuclear power plant accident (80.5%),
community plan for distribution of potassium iodine to appropriate populations and alerting system (84.0%),
radiation response functional roles for nurses (78.3%),
decontamination options (76.1%), and
nursing management of patient with radiation sickness (77.3%).
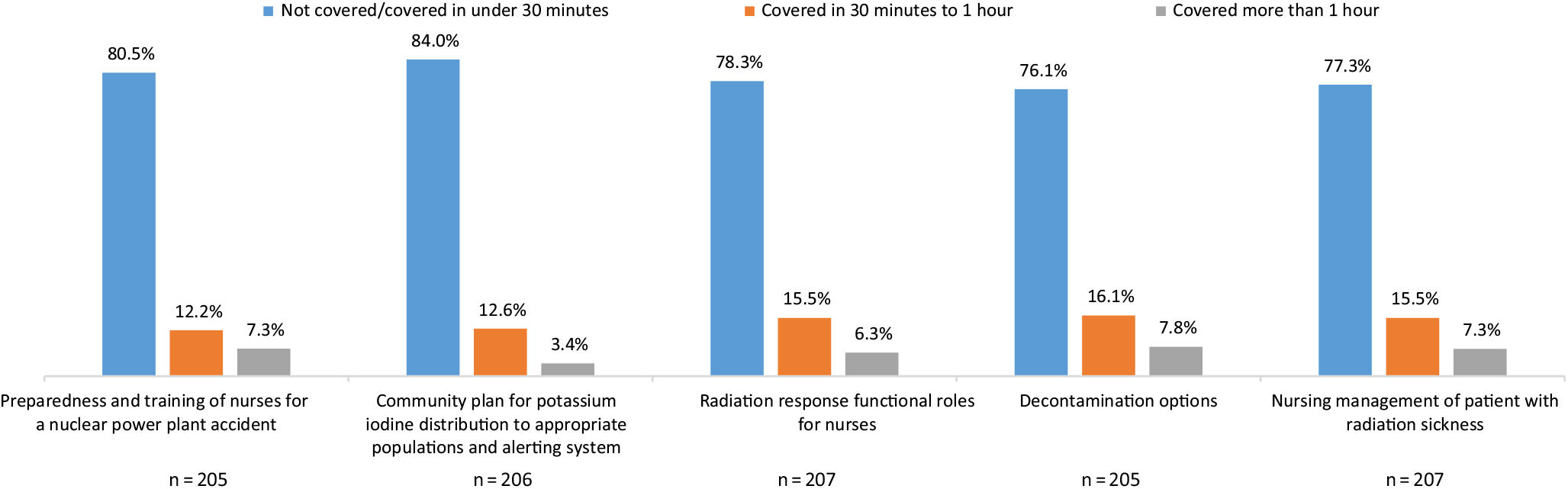
FIGURE 4 Nursing Roles and Responsibilities
Perceived Risk Versus Actual Risk
Of the 605 survey respondents who provided a zip code for the location of their SONs, 295 were located within an EPZ (47.2%; Figure 5). Respondents were asked to respond “yes” or “no” to the statement, “our school is located within 50 miles of a nuclear power plant,” to determine if they knew whether their SON was located within an EPZ associated with a nuclear power plant. A total of 228 respondents answered “no” to this question, and of those respondents, 106 were correct. However, 121 respondents (53%) responded incorrectly, and said that their school was not located within the 50-mile EPZ of a nuclear power plant when, in fact, it was. Furthermore, 18 of the respondents who were unaware that their school was located within 50 miles of a nuclear reactor indicated that “there was no perceived risk of this type of event [radiation/nuclear emergency] in our area,” when asked why radiation emergency content was not taught in their SON.

FIGURE 5 Sources of Nuclear Radiationa Surrounded by Representations of the 50-Mile-Radius Emergency Planning Zone (EPZ) Around Each Siteb
Geographic information system analysis revealed that 3 FEMA regions contain a high concentration of both SONs and nuclear radiation sources. The FEMA region maps in Figures 6, 7, and 8 show respondents who were located within the 50-mile EPZ of a nuclear reactor or other significant radiation source but were unaware of this risk. Additionally, when fault lines and seismic risk were mapped, data revealed substantial geographic risk to SONs located in these areas. Finally, while SONs report that “radiation/nuclear emergency preparedness is important (92.5%),” only 12.5% report having a radiation/nuclear emergency management operations plan, only 6% have ever drilled or tested their plan, and less than 10% of faculty report knowing what to do in the event of a radiation/nuclear emergency.

FIGURE 6 Area Representing Federal Emergency Management Agency Regions I, II, and III, Encompassing Highlighted States in the Northeastern United Statesa
FIGURE 7 Area Representing Federal Emergency Management Agency Region IX, Encompassing Highlighted States in the Western United Statesa,b

FIGURE 8 Area Representing Federal Emergency Management Agency Region V, Encompassing Highlighted States in the Midwestern Great Lakes Regiona
DISCUSSION
The United States preparedness goal is to be “a secure and resilient nation with the capabilities required across the whole community to prevent, protect against, mitigate, respond to, and recover from the threats and hazards that pose the greatest risk.”23 This goal represents the foundation of the National Preparedness System and is based on an all-hazards approach to identifying risks at the community, region, or national level that include both natural and human-caused disasters or emergencies. Communities with active nuclear reactors are at risk for exposure to radiation from unintentional or deliberate release or detonation of radiation. A large-scale radiation or nuclear event will create a public health emergency of international concern, with potentially thousands or even hundreds of thousands of victims seeking evaluation and care. While many lives may be lost, the possibility exists for many lives to be saved if health care services are rapidly available to the affected populations. These low-probability, high-consequence events will require specific radiation triage models,Reference Rea, Gougelet and Nicolalde24, Reference Casagrande, Wills and Kramer25 allocation of scarce resources,Reference Knebel, Coleman and Cliffer26 and the provision of highly specialized care. Victims of large-scale radiation exposure and/or blast injuries would present with trauma, burns, and/or acute radiation syndrome and would require many “nurse hours” for surgical and intensive careReference Casagrande, Wills and Kramer25 and surveillance and monitoring for long-term health impacts. The mental health impact of these events will create a substantial burden on the health care system. It is a certainty that nurses will be critical to the effectiveness of the health care and public health response.Reference Veenema and Thornton9, Reference Veenema and Thornton10, Reference Veenema and Karam27
In order for medical care and resources to be matched to the needs of the victims, a federal planning group developed a conceptual approach for responding to a nuclear detonation: the Radiation Treatment, Triage, and Transport response system.Reference Hrdina, Coleman and Bogucki5 Within this response framework, nurses will be needed across multiple clinical care settings as well as community reception centers and evacuation shelters. Additionally, institutions in the Radiation Injury Treatment Network, a collaborative of 81 hospitals and health systems committed to receiving marrow toxic victims of a large-scale radiation response, will be dependent upon their nursing workforce to render care.28
Educating health professionals—especially nurses, the largest group of health professionals in the United States (2 906 840 registered nurses as of May 2017)29—is a key component of the National Preparedness System and the National Security Strategy. However, the findings of this study reveal that over 75% of US SONs are not currently providing radiation content and further suggest that much of the current nursing workforce has not received adequate education and training regarding how to respond and care for patients and communities in the event of a nuclear and/or radiation emergency. This finding suggests that current federal and state radiation and nuclear preparedness plans may be built upon false assumptions of readiness, which has serious implications for national preparedness and response and for the National Health Security Strategy should an event occur.
The challenges of including radiation emergency and nuclear event content in nursing curricula are complex, as evidenced by the study findings. Nursing curricula must account for the National League for Nursing and AACN Essentials (bachelor’s, master’s, and doctoral), and many associate degree in nursing programs use the Accreditation Commission for Education in Nursing accreditation standards, as well as the BSN Essentials. Faculty frequently “teach to the test,” the National Council Licensure Exam. Other factors, such as faculty expertise (or lack thereof), faculty availability, faculty interest, and credit hours / time available in the curriculum, will directly influence what is taught in SONs. School of nursing faculty weigh the perceived need to teach radiation/nuclear preparedness against the need to cover the required content necessary for all nurses outlined in the AACN Essentials document.12
Ideally, SONs, like other community organizations, should have an emergency-operations management plan based upon a robust and updated hazard-vulnerability assessment. SONs should be both aware of and prepared for the hazards and risks in their own geographic area. This study suggests that over half of the US SONs that are located within 50 miles of an active nuclear reactor are unaware of this risk. The perceived lack of risk or exceptionally low risk of an event may explain the limited nuclear/radiation event-specific content in nursing education. Given that many respondents reported that it “never occurred to them to teach content on radiation/nuclear events,” it is not surprising that so few SONs provide content on the topic. These findings show not only that SONs perceive a low likelihood of these types of events occurring in the future, but also that until nurses are required to address this topic either in practice or on a licensure or certifying examination, this content will not be provided.
In the absence of faculty expertise, courses and tools are available to SONs and more continue to be developed. For example, the Public Health Foundation’s Public Health Preparedness and Response Program,30 the Centers for Disease Control and Prevention’s Preparedness and Emergency Response Learning Centers courses,31 A Decision Maker’s Guide: Medical Planning and Response for a Nuclear Detonation,32 and other resources at Radiation Emergency Medical Management33 are readily available. Additionally, the Society for the Advancement of Disaster Nursing website provides radiation and nuclear content, training materials, and access to subject matter experts.34 Interprofessional “Disaster Day” simulations, developed at Texas A&M Health Sciences Center,Reference Livingston, West and Livingston35 are examples of innovative methods for incorporating this content into existing curricula.
Twelve respondents (0.9%) indicated that they teach ≥10 hours of content on radiation emergencies and nuclear events; these represent outliers from the majority of the respondents. Several potential scenarios may serve to explain this phenomenon. First, these schools may actually teach ≥10 hours of content, either counting a combination of in-class didactic content and simulation or as part of interprofessional courses across health care schools (eg, medicine and public health). Additionally, the Centers for Disease Control and Prevention funded 9 universities36 to establish centers for emergency preparedness and emergency response, and it is possible that these 9 centers are represented in this dataset. Another possibility is that respondents may have misinterpreted the question itself and chose to count all radiation content presented to nursing students across their curriculum, such as radiation therapy for oncology, fluoroscopy, and other radiation-based interventions not related to a disaster event.
Limitations of the Study
This study involved self-reported data and is thus subject to the limitations associated with survey research. While the survey response rate for AACN SONs was robust (71.5%), the survey response rate for OADN schools was extremely low (2.1%). This fact may be due to the timing of the study. The web link to the online surveys was sent out via email in mid to late May, when most of the OADN SONs had finished their academic year. Because of the low response rate from OADN member schools, a comparison between groups was not conducted. Also of note, many study participants identified themselves as not involved in the curriculum decisions; as such, it is possible that their responses may not be accurate or may not accurately represent the reason why this topic is excluded or how to include it. With respect to the perceptions of risk versus actual risk, the geographic information system analysis was limited to the zip codes that were voluntarily provided. In actuality, the possibility exists that more SONs that responded were located within the EPZ of a nuclear power plant facility, test/research reactor, or waste-disposal site.
CONCLUSION
The cooperation of both the AACN and OADN in sending out the radiation nuclear survey provided the opportunity to analyze radiation/nuclear education across all levels of nursing education. The results reveal that US SONs are not providing radiation content and that the current and future nursing workforce may not have received adequate education and training regarding how to respond and care for patients and communities in the event of a nuclear and/or radiation emergency. A nurse who is well-trained to respond to radiation/nuclear events may be a scarce resource. Current federal and state radiation/nuclear preparedness plans may be built upon false assumptions of readiness, which would have serious implications for national preparedness and the National Health Security Strategy.
Further, our results suggest that nurse educators are not aware of the potential threat of radiological/nuclear sources. For SONs in high-risk geographic locations, it is essential that schools have radiation/nuclear emergency operations plans in place, that the plans are tested annually, that faculty are prepared to both teach and respond, and that radiation/nuclear curriculum content is integrated across teaching/learning opportunities. Academic accreditation agencies and licensing boards have the power to mandate such content in SONs, thus raising awareness across all nurse education programs and levels.
Until SONs do more to incorporate radiation/nuclear training into their curricula, the nation remains at risk for having an unprepared nursing workforce to respond to radiation and nuclear events.
Acknowledgments
Dr Veenema gratefully acknowledges the American Academy of Nursing, the American Nurses Association, and the American Nurses Foundation for their collective support of this study as part of her work as the 2017/2018 Distinguished Nurse Scholar-in-Residence at the National Academy of Medicine.
Additionally, the authors wish to thank the following individuals who graciously agreed to review the study instrument and provide email access to their membership:
Joan Stanley, PhD, CRNP, FAAN, FAANP (American Association of Colleges of Nursing) and Donna Meyer, MSN, RN, ANEF, FAADN, CEO, OADN (Organization for Associate Degree Nursing).









