Introduction
It is important to promote laryngeal elevation, necessary for swallowing, in patients with dysphagia in order to strengthen the muscle groups elevating the larynx, including the suprahyoid muscles.Reference Pearson, Langmore, Yu and Zumwalt1,Reference Pearson, Hindson, Langmore and Zumwalt2
The Shaker exercise,Reference Shaker, Kern, Bardan, Taylor, Stewart and Hoffmann3 a type of head-lift exercise, is the most commonly used method to strengthen the suprahyoid and tongue muscles. Its efficacy has been demonstrated in many studies related to dysphagia.Reference Antunes and Lunet4 However, the Shaker exercise could be difficult for elderly individuals to perform, as the action of lying down and then lifting the head requires considerable effort. A previous study involving the Shaker exercise in elderly individuals reported that many participants (30–50 per cent) dropped out.Reference Easterling, Grande, Kern, Sears and Shaker5 Some studies have reported that the sternocleidomastoid muscle group experiences fatigue faster than the suprahyoid and the infrahyoid muscles during head-lift exercises such as the Shaker exercise.Reference Ferdjallah, Wertsch and Shaker6,Reference White, Easterling, Roberts, Wertsch and Shaker7 White et al.Reference White, Easterling, Roberts, Wertsch and Shaker7 reported that early fatigue of the sternocleidomastoid muscle might limit the therapeutic efficacy of the Shaker exercise, as it does not have a role in the swallowing process.
Thus, laryngeal elevation training without lifting the head is useful, as it is associated with less physical strain compared with the head-lift exercise. In Japanese clinical practice, the swallowing forehead exercise,Reference Nagao, Tanaka, Fujishima, Shigematsu, Hojo and Koyama8 the chin push–pull manoeuvreReference Iwata, Nagashima, Hattori, Terashima, Shimizu and Kihara9 and laryngeal elevation training are commonly used as interventions for dysphagia. Several previous studies have demonstrated the efficacy of these training methods on swallowing function.Reference Sugiura, Fujimoto, Ando, Shimoda and Nakashima10,Reference Iwata, Terashima, Nagashima, Hattori, Horibe and Okada11 These training methods are reported to decrease the chin–hyoid bone distance by 11.1 per cent and the chin–thyroid cartilage distance by 8.4 per cent. They have also been reported to increase the sternum–thyroid cartilage distance by 12.0 per cent. Thus, the hyoid bone and the thyroid cartilage, which move closer to the sternum as a result of ageing, moved closer to the chin after the training. This change is expected to improve swallowing by promoting an earlier start of the swallowing process.
However, very few studies have evaluated the efficacy of laryngeal elevation training without lifting the head, and the effect of this exercise on variables directly evaluating the swallowing function has not been sufficiently investigated. Objective assessment of swallowing function is essential for analysing the efficacy of interventions in dysphagia. Hyodo et al.Reference Hyodo, Nishikubo and Hirose12 developed the Hyodo score, which is an objective and convenient scale for videoendoscopic assessment. The Hyodo score is widely used in clinical practice and studies in Japan.Reference Chiba, Sano, Ikui, Nishimura, Yabuki and Arai13–Reference Kumai, Miyamoto, Matsubara, Samejima, Yoshida and Baba16 Such objective criteria may be useful in generating reproducible evidence regarding the efficacy of the intervention performed to improve the swallowing function.
The present study aimed to investigate the effect of laryngeal elevation training without lifting the head on swallowing function, assessed using the Hyodo score, in patients with dysphagia.
Materials and methods
Participants
Patients with a chief complaint of dysphagia who visited the Nishiyama ENT Clinic between June 2018 and December 2019 were recruited. The inclusion criteria were: (1) patients with pharyngeal phase dysphagia caused by ageing or stroke; (2) incomplete upper oesophageal sphincter opening with post-deglutitive aspiration, or incomplete upper oesophageal sphincter opening with pre-deglutitive and post-deglutitive aspiration, as defined on videofluoroscopy; (3) patients with vallecular residue and/or hypopharyngeal (pyriform sinus) residue; and (4) patients able to comply with the protocol, willing to perform the exercise programme and able to attend the study session.
The exclusion criteria were: (1) head and neck cancer; (2) lack of cognition; (3) patients who could not lift their head and flex their neck; (4) patients unable to exercise independently or with a caregiver; (5) absent pharyngeal swallow on videoendoscopy or videofluoroscopy; (6) aspiration during swallowing; and (7) neurodegenerative disorders such as multiple system atrophy.
The study was approved by the ethical committee of the Kanagawa Prefecture Medical Association and was performed according to the ethical standards laid down in the Helsinki Declaration of 1975, as revised in 2008.
Procedure
This study was an observational study. Participants were evaluated after providing written informed consent. All participants performed the swallowing forehead exercise and chin push–pull manoeuvre for two months. They also underwent respiratory muscle training if it was therapeutically necessary. Videoendoscopy for the assessment of swallowing function, the peak expiratory flow test and the hand grip strength test were performed at the initial visit (before the start of the intervention (time 1)) and two months after the start of the intervention (time 2). We also measured participants’ height and weight at the same two time points in order to calculate body mass index (BMI).
Intervention
Participants were instructed about the intervention by our dysphagia treatment team, consisting of ENT physicians, nurses and speech therapists. At the initial visit, the team members instructed the participants on how to perform the swallowing forehead exercise and the chin push–pull manoeuvre. The physicians verbally confirmed participants’ progress at every visit (once a month).
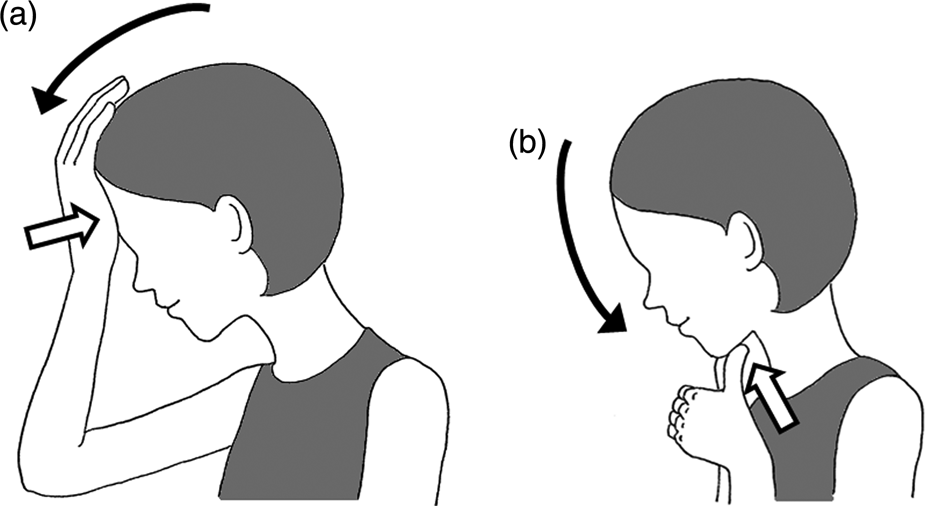
For the swallowing forehead exercise, participants were instructed to lower their head, peering down at their abdomen, and to push their forehead using the carpal region for 5 seconds (Figure 1a). For the chin push–pull manoeuvre, participants were instructed to keep the mandible pulled firmly toward the chest and to push their mandible strongly using their thumb for 5 seconds (Figure 1b). Participants performed these exercises 3 times a day (before every meal) in sets of 10.

Fig. 1. Laryngeal elevation training used in this study: (a) the swallowing forehead exercise, and (b) the chin push–pull manoeuvre.
Measurements
Hyodo scoring using videoendoscopy
All participants were seated in the upright position in a chair during videoendoscopy for the assessment of swallowing function. Videoendoscopy was performed using the ER-530S2 video endoscope system (Fujifilm, Tokyo, Japan) by an otorhinolaryngologist who was a dysphagia expert with over 30 years’ experience in videoendoscopy.
We used the Hyodo score, a videoendoscopic score system developed by Hyodo et al.,Reference Hyodo, Nishikubo and Hirose12 to evaluate the swallowing function. The Hyodo score consists of four parameters: the degree of salivary pooling at the vallecula and at the pyriform sinuses, glottal closure reflex induced by the contact of the endoscope with the epiglottis or the arytenoids, initiation of the swallowing reflex assessed by the ‘white-out’ timing, and pharyngeal clearance after swallowing blue-dyed water (Table 1). Each parameter was scored on a four-point scale (0 = normal, 1 = mild impairment, 2 = moderate impairment and 3 = severe impairment). The first parameter indicates the sensory and motor functions. The second and third parameters indicate the sensory function. The fourth parameter indicates the motor function of swallowing. The Hyodo score is expressed as the sum of scores for all four parameters, ranging from 0 to 12. A Hyodo score of more than 6 is considered a strong predictor of aspiration.Reference Chiba, Sano, Ikui, Nishimura, Yabuki and Arai13
Table 1. Hyodo scoring systemReference Hyodo, Nishikubo and Hirose12,Reference Chiba, Sano, Ikui, Nishimura, Yabuki and Arai13

Respiratory function
The peak expiratory flow test was performed using the Assess NE-PF2 peak flow meter (Health-Scan Products, Cedar Grove, New Jersey, USA) to measure the air flowing out of the lungs. The peak expiratory flow is considered to reflect the efficacy of respiratory muscle training. Troche et al. reported that improvement in expiratory muscle strength was associated with improvement in swallowing function.Reference Troche, Okun, Rosenbek, Musson, Fernandez and Rodriguez17 Thus, the peak expiratory flow was used to adjust the efficacy of respiratory muscle training in this study.
Hand grip strength
Hand grip strength was assessed using the Tanita Hand Grip Meter 6103 (Tanita, Tokyo, Japan) with the participants in the sitting position.
Hand grip strength has been used as an indicator of whole-body muscle strength in many studies.Reference Ikeda, Murata, Otao, Kai, Murata and Tominaga18–Reference Morimoto, Suga, Tottori, Wachi, Misaki and Tsuchikane20 It has been reported to be associated with swallowing function.Reference Mendes, Nascimento, Mansur, Callegaro and Filho21–Reference Sugaya, Goto, Okami and Nishiyama23 Thus, hand grip strength was used as a co-variate in the present study.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics software, version 25.0 (IBM, Armonk, New York, USA). Pearson's correlation coefficient was used to evaluate the association between the Hyodo score and other variables. A linear mixed model was applied to compare the Hyodo score between the time points using compound symmetry and treating time points as fixed effects and individual variations as random effects. Peak expiratory flow, hand grip strength, and BMI at time 1 and time 2 were also included in the model as time-varying co-variates. A p-value of less than 0.05 was considered statistically significant.
Results and analysis
Descriptive results
Altogether, 110 patients met the listed requirements. We excluded participants with missing data on the Hyodo score at time 2 (n = 53). Thus, the final analysis included 57 participants. Among these, 36 participants (63.2 per cent) were men. The age and disease duration (mean ± standard deviation (SD)) were 78.5 ± 11.4 years (range, 49–97 years) and 12.8 ± 17.1 months (range, 0.3–120 months), respectively. For some patients, there were no data on peak expiratory flow (valid data: n = 36 at time 1 and n = 27 at time 2), hand grip strength (valid data: n = 40 at time 1 and n = 30 at time 2) or BMI (valid data: n = 50 at time 1 and n = 32 at time 2).
The mean ± SD values for the Hyodo score, peak expiratory flow, hand grip strength and BMI, at time 1 and time 2, are presented in Table 2. Correlation analysis showed that the Hyodo score at time 1 significantly correlated with: peak expiratory flow (r = −0.40, p = 0.02), hand grip strength (r = −0.35, p = 0.03) and BMI (r = −0.34, p = 0.02). The Hyodo score at time 2 was significantly correlated only with hand grip strength (r = −0.53, p = 0.003). Age and disease duration showed no significant correlation with the Hyodo score at any time point.
Table 2. Means and standard deviations of variables at each time point

BMI = body mass index
Linear mixed model results
The linear mixed model showed a significant main effect of time (F(1,31.7) = 10.8, p = 0.002). The effects of co-variates were not significant (peak expiratory flow: F(1,57.9) = 0.5, p = 0.49; hand grip strength: F(1,53.3) = 3.1, p = 0.08; and BMI: F(1,48.4) = 0.3, p = 0.61). The Hyodo score at time 2 was significantly lower than that at time 1. The estimated values for the Hyodo score at each time point are shown in Figure 2.

Fig. 2. The Hyodo scores (estimated values) at time 1 (initial visit) and time (2 months after the start of the intervention). Error bars indicate standard error.
Discussion
We observed a significant effect of laryngeal elevation training without highly loaded head lifting on the Hyodo score, which is an objective and convenient scale for videoendoscopic assessment. This result was obtained after adjusting for peak expiratory flow, which was improved by respiratory muscle training. Thus, we could extract the unconsolidated efficacy of the laryngeal elevation training used in the present study. Our results are consistent with the results of a previous study that showed the efficacy of similar laryngeal elevation training, which included the swallowing forehead exercise and the chin push–pull manoeuvre.Reference Sugiura, Fujimoto, Ando, Shimoda and Nakashima10,Reference Iwata, Terashima, Nagashima, Hattori, Horibe and Okada11 Additionally, our results provide new findings on the efficacy of the Hyodo score.
The swallowing forehead exercise and the chin push–pull manoeuvre used in the present study are low-load interventions. Hence, their convenience encourages compliance. Ageing decreases pharyngeal clearance,Reference Cook, Weltman, Wallace, Shaw, McKay and Smart24 which in turn increases the chances of aspiration. Weakened cough intensity in addition to increased aspiration elevates the risk of aspiration pneumonia.Reference Sohn, Park, Koo, Jang, Han and Im25 Considering the effects of ageing, a method that can be conducted every day, before every meal, anywhere, and without specialised equipment, is needed to treat or prevent deteriorated swallowing function in clinical practice. Laryngeal elevation training without head lifting can be performed by any individual in different situations. Thus, the results regarding the efficacy of this training may provide useful information to medical settings that conduct continuous swallowing training. Additionally, the Hyodo scoring using videoendoscopy is more convenient for studying the efficacy of training in dysphagia compared with videofluoroscopy, which is often used for swallowing function assessment. The present study is the first to demonstrate the reactivity of the Hyodo score to laryngeal elevation training in patients with dysphagia caused by ageing or stroke.
The present study has several limitations. The sample size of the study was small, limiting further analysis by gender, age, extent of disease and strength. Improving this limitation may clarify which patients would benefit from laryngeal elevation without head lifting. Although respiratory muscle training was added as a treatment for dysphagia in our participants, intervention using laryngeal elevation training alone may provide more accurate results than statistically adjusting for the effect of respiratory muscle training. The present study lacked a control group. A randomised, controlled protocol is warranted to evaluate the effect of laryngeal elevation training without head lifting on swallowing function to obtain more convincing evidence.
• Laryngeal elevation training without lifting the head is useful, as it is associated with less physical strain compared to the head-lift exercise
• Few previous studies have investigated the efficacy of laryngeal elevation training without lifting the head
• The effect of exercise on variables directly evaluating swallowing function has not been sufficiently investigated
• The Hyodo score is an objective, convenient scoring method for videoendoscopic assessment
• This study investigated the effect of laryngeal elevation training without highly loaded head lifting on swallowing function using the Hyodo score in dysphagia patients
• Training including the swallowing forehead exercise and chin push–pull manoeuvre can be used with Hyodo scoring to treat dysphagia
In conclusion, the present study demonstrated the significant effect of laryngeal elevation training without highly loaded head lifting on the Hyodo score, which is an objective and convenient scale of videoendoscopic assessment in patients with dysphagia caused by ageing or stroke. Such training, including the swallowing forehead exercise and the chin push–pull manoeuvre, in combination with assessment using the Hyodo score, is expected to be utilised in the clinical practice of dysphagia worldwide.
Competing interests
None declared