


The importance of health technology assessment (HTA) in the decision-making processes for publicly financed health services has increased in recent years (Reference Garrido, Kristensen, Nielsen and Busse1). A substantial number of jurisdictions worldwide have implemented HTA, especially as it applies to transparent processes for drug reimbursement (Reference Cleemput, Franken, Koopmanschap and le Polain2). There is an impressive tradition of HTA in Europe, starting with HTA activities in Sweden in the 1970s and quickly followed by the development of formal and informal programs in other European countries (Reference Banta, Kristensen and Jonsson3).
Central and Eastern European (CEE) countries have followed a similar route of implementing HTA processes into decision making (Reference Gulacsi, Rotar and Niewada4) especially when they accessed into the European Union (EU) and were obliged to implement Council Directive 89/105/EEC of 1988 otherwise known as “Transparency Directive,” which relates to the transparency of measures regulating the prices of medicinal products for human use and their inclusion in the scope of national health insurance systems. Poland belonged to this group of countries that implemented HTA in its healthcare system and has been even perceived as a leader among new member states in the field (Reference Nizankowski and Wilk5). The remaining CEE countries are much smaller and face more limitations in full HTA implementation because of correspondingly fewer resources and larger difficulties in building large capacities for HTA (Reference Kaló, Gheorghe, Huic, Csanádi and Kristensen6).
As the largest country in the CEE region with 38.5 million inhabitants compared to the second largest country in the region which is the Czech Republic with 10.5 million people (7), Poland has a unique role among Western and Eastern European countries. On the one hand, the Polish government is dedicated to making transparent decisions that result in the best allocation of financial resources and to allowing timely patient access to innovative medicines. On the other hand, the country's financial resources are very limited, its pharmaceutical market is mainly generic driven, and there is not always transparent pressure on decision makers from an innovative pharmaceutical industry (Reference Ozieranski, McKee and King8). As a result, Poland has evolved a balanced, data driven system that could be used as an example for countries looking to establish HTA within their country.
From an absolute lack of the usage of and reimbursement for innovative medicines (Reference Kaló, Gheorghe, Huic, Csanádi and Kristensen6) Poland has evolved into a late adopter of potentially valuable therapies through the implementation of an HTA process that uses a selective approach based on the clinical value of medicines as well as on cost-effectiveness criteria. A cost to quality-adjusted life-year (QALY) threshold has been embedded in Polish legislation that is equal to the tripled gross domestic product (GDP) value per capita or approximately 130,002 zloty (30,500 Euros) (9). In addition, HTA evaluations have steadily increased since the inception of the Polish HTA agency in 2005 and its formal implementation in 2006. Figure 1 shows this progression over the decade 2006–16.

Figure 1. Assessments by AOTMiT, 2006–16: Drug technologies, non-drug technologies, health programs, and dietary supplements. AOTMiT, Agency for Health Technology Assessment and Tariff System; HTA, health technology assessment.
The objective of this study is to illustrate and provide a better understanding of the role of HTA processes in decision making for drug reimbursement in Poland and how this approach could be considered by other countries of limited resources taking into account the historical perspective and the evolution of the HTA system and processes in Poland over the past decade and current developments.
RATIONALE FOR THE ESTABLISHMENT OF AN HTA AGENCY IN POLAND
In the first decade of the twenty-first century, pricing and reimbursement decisions for new medicines were issued in an untimely manner in Poland, resulting in a delay of several years for listing decisions for some drugs. In addition, there was no homogeneity in the rationale for negative ministerial decisions and no appeal mechanisms were in place. Therefore, when Poland accessed into the EU in 2004, there was substantial political pressure from the EU Commission to implement a transparent criteria for drug reimbursement and to allow timely patient access to innovative medicines. After becoming an EU member, Poland adopted the EU acquis communautaire, or the accumulated body of European law, as part of the Polish legal order, including the previously cited “Transparency Directive.” The three main guarantees of the Directive regarding individual pricing and reimbursement decisions are that: (i) decisions must be made within a specific timeframe (90/180 days); (ii) decisions must be communicated to the applicant and contain a statement of reasons based on objective and verifiable criteria; (iii) and decisions must be open to judicial appeal at the national level (10).
The Polish HTA Agency, Agencja Oceny Technologii Medycznych i Taryfikacji (AOTMiT; the Agency for Health Technology Assessment and Tariff System), was created formally in 2005 and in operation by 2006. The need to implement Council Directive 89/105/EEC of 1988 otherwise known as “Transparency Directive” played an important role in decision to establish the agency (Reference Sagan, Panteli and Borkowski11). AOTMiT, first known as the Agency for Health Technology Assessment (AOTM), was established through an Ordinance of the Minister of Health in 2005 and began to function in 2006 as an advisory body to the Minister of Health.
In 2009, the AOTMiT position was reinforced with the revision of the “Basket Law” regarding healthcare services financed from public funds, and HTA was officially anchored in the Polish pricing and reimbursement process. The pragmatic HTA model was affirmed in which AOTMiT is mainly the assessor of reports for innovative drugs, however, may also serve as a producer of reports for medical procedures. In parallel, agency funding increased with the introduction of fees for the assessment and appraisal of HTA dossiers submitted by pharmaceutical companies for innovative drugs.
Over the past decade, AOTMiT has mainly assessed drug technologies and several non-drug technologies. Since 2009, the evaluation of health programs developed by regional governments has become a separate, substantial task performed by a dedicated team of internal and external analysts. The next milestone for the HTA process in Poland was the entrance of the Reimbursement Law in 2012 on the reimbursement of medicinal products, special purpose dietary supplements and medical devices (Reference Kawalec, Sagan, Stawowczyk, Kowalska-Bobko and Mokrzycka12). At this time, Poland had managed to fully implement the Transparency Directive to its legal system. In 2015, the agency competencies were broadened, adding the valuation of health services, otherwise known as the “tariff system” (taryfikacja), and the agency changed its name from AOTM to AOTMiT. Key milestones in the evolution of AOTMiT are illustrated in Figure 2.

Figure 2. Key milestones in AOTMiT evolution. AOTMiT, Agency for Health Technology Assessment and Tariff System; AOTM, Agency for Health Technology Assessment; MoH, Ministry of Health; HC, health care; HTA, health technology assessment.
CAPACITY BUILDING IN THE FIELD OF HTA
One of the critical activities to increase the transparency and competence of the Polish pricing and reimbursement system was the twinning project between Poland's AOTMiT and Ministry of Health (MoH) and France's Haute Autorité de Santé (HAS) and MoH, which included substantial participation from international experts. This project, took place from October 2006 through April 2008 (Reference Zagorska, Krol and Lipska13). The aim of the project was to enhance the transparency and competence of the Polish drug reimbursement decision-making process (Reference Lipska14).
The twinning project produced workshops and conferences. Specific proposals were put forth for a transparent and clear pricing and reimbursement process in Poland, including a set of recommendations regarding the role of AOTMiT and MoH, separate tracks for generic and innovative drugs as well as guidance for the applicants based on HTA guidelines. These proposals were implemented to the Polish legal system by means of amending the Basket Law regarding healthcare services financed from public funds in June 2009 (Reference Zagorska, Krol and Lipska13) and later on the implementation of Reimbursement Law in 2012.
DRUG REIMBURSEMENT PROCESS IN POLAND
The Reimbursement Law that entered into force in 2012 regulates drug reimbursement in Poland and asserts leadership of the MoH in the process. The Reimbursement Law introduced some order and transparency to the system; however, it is not free from defect, and in 2015, the newly elected Polish government began an investigation into potential modifications of this law, although it is currently too early to specify the ultimate legal ramifications of these modifications.
As the principal owner of the pricing and reimbursement process in Poland, the MoH has the responsibility to coordinate all of its elements, starting with the receipt of pricing and reimbursement applications from marketing authorization holders and ending in the formulation of pricing and reimbursement decisions. These decisions must be made within a specific timeframe set out in the Transparency Directive; that is, 90 days from receipt of application for decisions on prices; 90 days for decisions on reimbursement; and 180 days for both pricing and reimbursement decisions.
The process for innovative drugs begins with the sponsor submitting a pricing and reimbursement application to the MoH (Figure 3). The elements of the application dossier are precisely listed in the Reimbursement Law, and these include: general data regarding the applicant; a commitment to ensure continuity of supply in case the drug is reimbursed; marketing authorization data; a proposal of reimbursed indication(s), price, reimbursement limit, a risk-sharing scheme (the Reimbursement Law specifically points toward outcome based schemes and financially based schemes mainly discounts or price volume arrangements); a proposal of drug program if relevant; international price comparisons; and proof of payment for the application procedure with the MoH and AOTMiT (9).

Figure 3. The pricing and reimbursement application process for new drugs in Poland. P&R, pricing and reimbursement; AOTMiT, Agency for Health Technology Assessment and Tariff System; HTA, health technology assessment; MoH, Ministry of Health; reimb., reimbursement; n/a, not applicable; re., regarding.
The MoH first examines the application from a formal perspective and, if necessary, informs the applicant on the need to complete or modify any of its elements. The applicant then has 7 days to update the dossier, and this delay stops the 90/180-day clock. Once the application is complete, the MoH refers it to AOTMiT for a recommendation as to whether the drug meets the criteria specified in the Polish HTA guidelines and should be financed from public funds.
The President of AOTMiT has 60 days to present its recommendation to the Minister. The internal process at AOTMiT begins with an assessment by an analytical team that results in an evaluation report called a verification analysis (analiza weryfikacyjna). Both an application dossier and a verification analysis are based on Polish HTA guidelines (15) (which are described in Supplementary Material 1). The evaluation report compiles the reimbursement decisions and conditions from other countries. It also includes an assessment and critical review of the pharmacoeconomic dossier submitted by the applicant; that is the clinical, economic, budget impact, and rationalization analyses, which are submitted if the budget impact analysis demonstrates an increase of reimbursement costs and show scenario(s) for releasing public funds in the amount corresponding to the increase in budget impact.
The evaluation report, which is available for comments 7 days from its publication online, is then presented to the Transparency Council for appraisal, which issues its opinion in the form of a position (the composition and tasks of the Transparency Council in comparison to previous Consultative Council are described in Supplementary Material 2). The recommendation of the Agency is issued by its President based on the position of the Transparency Council and the formal assessment criteria; it comprises the rationale for the recommendation including conditions for drug reimbursement such as possible restrictions and/ or risk-sharing schemes.
The current strong position of the Transparency Council in the HTA decision process is unquestionable and according to Instytut Arcana, the concordance between the Council's and the Agency President's recommendation is high. Indeed, from 1 January 2012 through 13 December 2014, the President's recommendation differed from the Council's position for 7 percent of cases (Reference Skóra and Wilk16). However, more recent research indicates a growing divergence between the Council's and Agency President's judgments in the past 3 years (17).
The recommendation of the President together with the Position of the Transparency Council and the verification analysis are referred by the Minister to the Economic Commission affiliated with the MoH for pricing and listing negotiations with the sponsor. The Commission is made up of twelve representatives of the Minister of Health and five representatives of the public payer (National Health Fund). The output of the negotiations is twofold: resolution of the Economic Commission and the minutes from the negotiations.
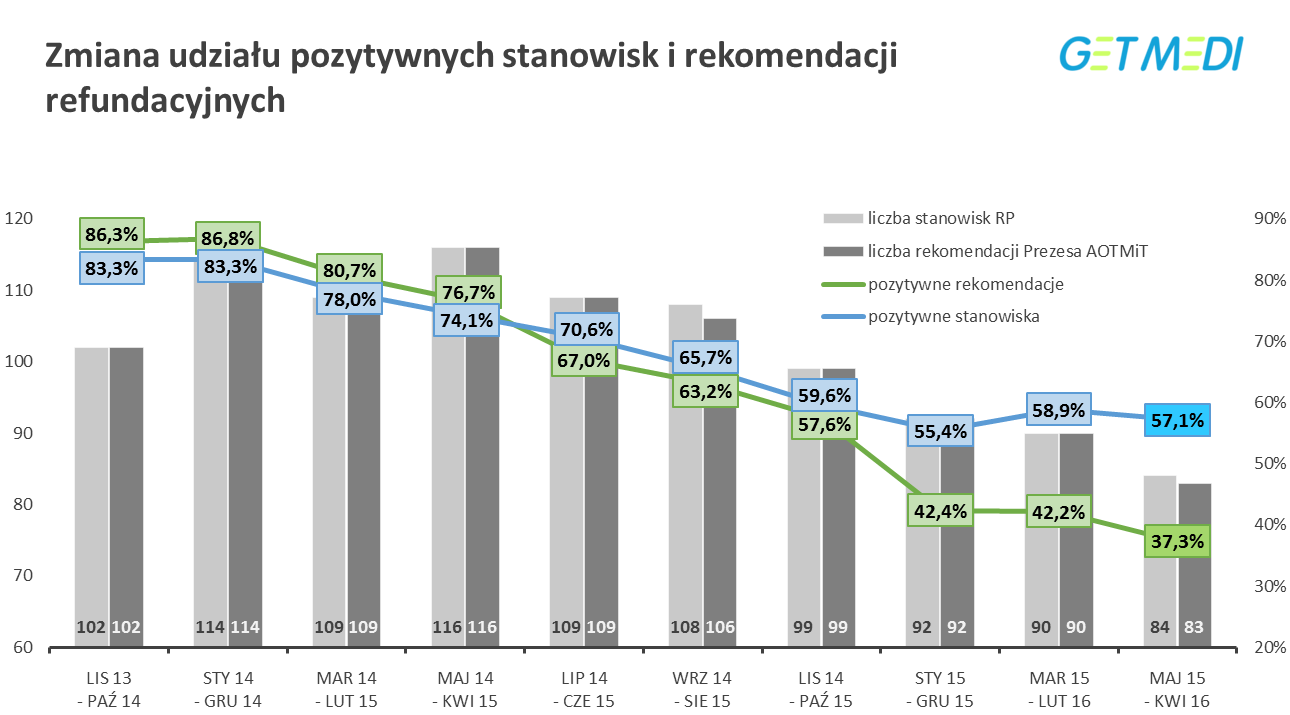
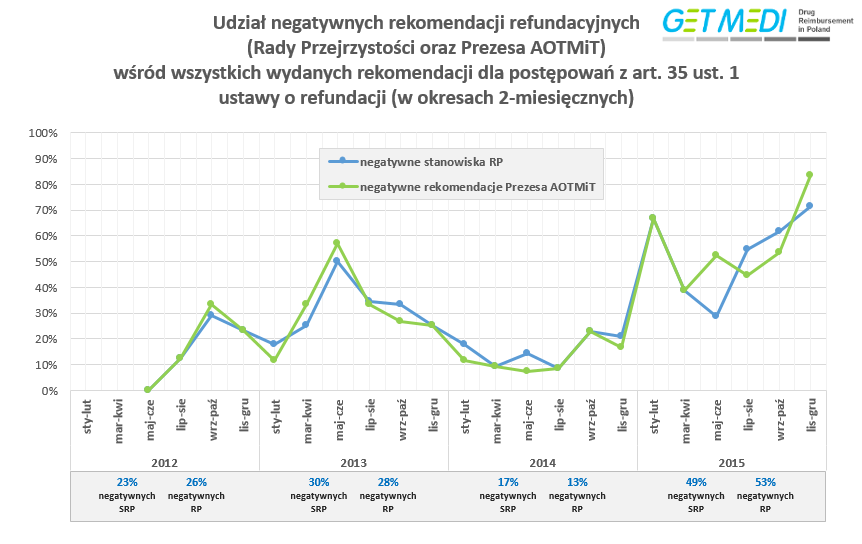
The process may be affected by unanticipated interventions from individuals in particular government officials. The most illustrious case is that of the 2015 intervention by the Deputy Health Minister in the form of a letter where the Agency is urged not to value the clinical efficacy over cost-effectiveness (18). This intervention led to an increase in negative recommendations from approximately 20 percent in the end of 2014 to more than 70 percent the beginning of 2015 (19).
Having received the Agency's and Commission's output, the Minister of Health makes an independent reimbursement decision. The Minister's decision is discretionary and is based on legal reimbursement criteria. The Minister must disclose all evidence assembled before issuing the final decision, and the applicant has the right to file its position. The decision is subject to appeal within 14 days by the Sponsor. It is worth noting that research suggests the concordance between the ministerial decision on reimbursement of innovative medicines and AOTMiT recommendations is low, and only one third of positive HTA recommendations result in positive reimbursement decisions from the MoH (Reference Skóra and Wilk16). However, the MoH can also decide that a medicine given a negative opinion is reimbursed, as seen recently (September 2016) with a chronic obstructive pulmonary disease (COPD) medicine that received a positive reimbursement decision by the Minister of Health despite a prior negative recommendation by the President of AOTMiT (20).
The Minister publishes the reimbursement list once every 2 months in the Official Journal of the Minister of Health. The list contains information such as the medicine's category and level of reimbursement, its price, and patient co-payment level, as well as the date of entry into force of the reimbursement decision and its validity.
DRUG REIMBURSEMENT CRITERIA
The current (since 1 January 2012) and previous (binding up to 31 December 2011) drug reimbursement criteria are described in Table 1. Previously, the law stated that the Minister of Health should take the above-mentioned criteria into account after receiving the recommendation of the AOTMiT President. Currently, agency recommendations reflect an improvement in the order and transparency of the drug pricing and reimbursement decision process in Poland. Moreover, reimbursement verdicts are now published in the form of “administrative decisions” and enable an appeal mechanism for the applicant. Formerly, reimbursement decisions were issued in bulk and there were years where no one single reimbursement decision was published by the Minister. Today's reimbursement decisions are drug related and are disseminated in the form of the Minister's Communique in bimonthly intervals.
Table 1. Comparison of Current (Since 1 January 2012) and Previous Drug Reimbursement Criteria in Poland (Binding up to 31 December 2011)

Drug decisions include formal information regarding the applicant and the drug as well as the classification into a reimbursement category or drug program. In parallel, they include data on the relevant level of funding, price, reference group, and risk-sharing schemes.
DISCUSSION
Before the establishment of AOTMiT, new innovative drugs were not even considered for reimbursement from public funds in Poland due to budgetary constraints, and even more importantly, there was a lack of objective criteria. In fact, there were several corruption scandals around reimbursement processes in Poland, based on very subjective criteria for drug reimbursement in the late 1990s. At that time, regularly submitted reimbursement applications were not evaluated at the MoH, due to the lack of appropriate procedures, objective criteria, and defined timelines.
Successful Implementation of HTA in Poland
The evolution started in 2005 from an unquestionable lack of objective reimbursement criteria and progressed by means of a capacity and institutional building exercise with the French institutions HAS and MoH and international experts between 2006 and 2008 up to the full implementation of the EU Transparency Directive into the Polish legal system through the Reimbursement Law in January 2012.
The twinning project between AOTMiT, Polish MoH, and French partners HAS and MoH played a key role in HTA capacity building and the implementation of evidence based criteria into drug reimbursement decision making in Poland.
Today, HTA has been successfully implemented into the decision-making processes for drug reimbursement in Poland, and is based on a solid legal foundation that includes the Reimbursement Law. However, there are some current political tensions regarding the scope of activities performed by AOTMiT, which has been recently expanded to include new tasks dedicated to tariffs. Although these tasks have been defined as a political priority by the Polish government, there is a concern that this work may devalue the importance of HTA activities and processes developed by AOTMiT.
Capacity and expertise in HTA has been steadily increasing for stakeholders at AOTMiT and among those producing HTA reports and working in academic centers and industry, especially during the EU-funded twinning project between Poland and France. AOTMiT management teams should be aware of the potential risk of the loss of highly trained staff, who may believe that the HTA functions have been devalued, to higher paying positions within the pharmaceutical industry, and look to mitigate against potential loss of expertise and experience. The issue of experts’ movements between private and public institutions in the Polish reimbursement system, known as “institutional nomads,” has been investigated by Ozierański and King (Reference Ozierański and King21).
Room for Improvement
Because transparent HTA processes have been implemented by AOTMiT in recent years and efficacy and safety profile seem to contribute most to final Agency's recommendations (Reference Niewada, Polkowska, Jakubczyk and Golicki22), drug reimbursement decision making based on objective verifiable criteria will likely continue regardless of political pressures. However, attention must continue to be paid to the quality of the HTA processes in place at the agency and to continuous capacity building to avoid potential compromise.
It is worthwhile to note that the transparent well-designed HTA system in Poland has got several gaps that enable mostly political, not evidence-based, interventions from individuals at different stages of reimbursement processes (Reference Ozierański and King21), notably from the AOTMiT's President (7 percent recommendations are not coherent with Transparency Committee [TC] positions) and the Minister of Health (only one-third of positive HTA recommendations result in positive reimbursement decisions) (Reference Skóra and Wilk16).
Previous research indicates that the concordance/agreement between AOTMiT President and TC measured by V-Cramer equals 0.549, where 0 corresponds to no association and 1 to complete association (23). The association between AOTMiT President recommendations and MoH reimbursement decisions is even much lower amounting to 0.314 measured by V-Cramer association (24).
External factors can also influence the work of the Agency. The above mentioned 2015 intervention by the deputy minister of health (18) led to a surge in negative recommendations issued by the AOTMiT (19). The discretionary power of the Minister of Health affects the outcome of reimbursement decisions. The stated above case of the COPD medicine receiving a positive reimbursement decision despite negative AOTMiT recommendation is emblematic (20). Similar situations may result in substantial unpredictability of final reimbursement decisions.
“Pragmatic” Model
The HTA model that has been implemented in Poland can be called “pragmatic” because the pharmaceutical company is fully responsible for the preparation of a reimbursement dossier of good quality in line with HTA Guidelines and the assessment team in AOTMiT is responsible for critical review of that dossier (“analiza weryfikacyjna”). This is a similar approach to that implemented in Scotland by the Scottish Medicine Consortium in which through the use of very limited but extremely competent resources, all new active substances can be fully assessed based on the dossier submitted by the industry.
This is in comparison to the so-called “full model” HTA agency, such as that of the National Institute for Health and Care Excellence in England, in which the report on a new health technology is prepared by the HTA agency either internally or through external resources such as academic centers. A full model HTA agency requires substantial financial and human resources as a precondition that are not feasible for the Polish healthcare system.
Consideration of Polish HTA Model by New and Evolving Countries
The development of HTA activities in Poland can be perceived as a unique intermediate model of late adoption of innovative technologies, given the limited financial resources of the Polish healthcare system. The key success factors in this development were effective capacity building based on the use of international expertise, the implementation of transparent criteria into the drug reimbursement processes and the selective approach to the adoption of innovative medicines based on the cost-effectiveness threshold among a variety of other criteria.
The Polish experience in the implementation of HTA into the healthcare system could be used by countries that have limited resources seeking for potential solutions to implement HTA based on international models. There are three key aspects which underpin the process in Poland and would need to be considered by countries looking to adopt the Polish model: a policy framework, methodological developments, and capacity building. First, the creation of a policy framework with corresponding legal acts is recommended to be considered as the foundation of HTA implementation (e.g., “Basket Law,” “Reimbursement Law” in Poland). Second, this policy framework needs to be directly linked with methodological developments in the field of HTA, for example, HTA guidelines development and implementation (first HTA guidelines developed in Poland in 2007 with the update in 2009 and 2016). Third, capacity building in the field of HTA in a given jurisdiction with regards to both internal (HTA agency) and external resources (academia, pharmaceutical industry, patients organizations) based on international expertise needs to be considered as a key long term perspective success factor (in Poland both HTA agency employees and external institutions, e.g., academia have been trained by international experts within EU Transition Facility project). The way Poland approached these three key aspects of HTA implementation create potential value for international usage in particular in countries with limited financial resources.
The Polish experience is an example of pragmatic approach to implementation of an HTA model that could be considered by other countries looking to establish HTA systems. It is unique both in terms of potential learnings from the country with very limited resources in a healthcare system and also the adoption of methodological challenges related to HTA implemented into a healthcare system, in particular into a drug reimbursement system.
CONCLUSION
The role of HTA in the drug reimbursement process in Poland has increased substantially over the recent decade leading to a sensible and balanced system which has enabled the implementation of objective data driven criteria.
However, while Poland is regarded as a leader in Central and Eastern Europe, there is room for improvement, especially with regard to the quality of HTA processes, especially the consistency of HTA guidelines with Reimbursement Law, staff competence, and turnover. Moreover, the gap between Poland and the rest of Europe should be narrowed in terms of making innovative drugs accessible to patients as Poland lags behind other countries in reimbursing innovative oncology drugs (25).
As countries around the world look to establish their own HTA process and procedures the evolution of the HTA process in Poland may give some direction on how to balance differing priorities and ensure transparent and objective access to medicines for patients who need them.
SUPPLEMENTARY MATERIAL
Supplementary Material 1: https://doi.org/10.1017/S0266462317000563
Supplementary Material 2: https://doi.org/10.1017/S0266462317000563
CONFLICTS OF INTEREST
Dr. Lipska worked at AOTMiT between 2006 and 2011 as the Head of the Analytical Department and the Agency Deputy Director for HTA. Between 2006 and 2008, Dr. Lipska was the Polish Project Leader of the EU-funded Transition Facility Project between Poland (AOTMiT, MoH) and France (HAS, MoH). The other authors have nothing to disclose.







{kind=link}
{kind=link}
{kind=link}
{kind=link}