“If you don’t know where you are going, any road will get you there.”–
Lewis Carroll
Introduction
The number of state hospital beds occupied by forensically committed psychiatric patients is rising, even as the overall number of state hospital beds continues to decline. 1 However, the standard treatment planning process for forensic psychiatric patients committed by the criminal justice system has not been reformulated to address the unique needs of this rapidly growing forensic population. The integration of forensic issues into the recovery movement has not been clearly articulated in the literature. A literature search (using the keywords treatment plan forensic, treatment plan inpatient psychiatry, multidisciplinary forensic treatment plan, recovery oriented treatment plan, forensically driven discharge criteria, and treatment goals forensic) produced few articles that explicitly and directly address the unique aspects of treatment planning for the forensic patient.Reference Hart, Sturmey, Logan and McMurran 2 – Reference Davis 5 As most forensic state hospital admissions either target violence risk mitigation or trial incompetency, treatment planning should be focused on these two areas.
Treatment Planning for Violence Risk Mitigation
Most of the time, forensic patients lack the “medical necessity” justification that exists for community patients who are admitted for acute inpatient stays; for patients from a variety of commitments categories, such as Not Guilty by Reason of Insanity (NGRI) or Mentally Disordered Offenders (MDO), hospitalization is based on a “likelihood” of violence, not an “imminent” danger. These patients, therefore, require a forensic risk evaluation that involves multiple static and dynamic factors, which range from previous violence to current negative attitudes to future exposure to destabilizers, in addition to more traditional clinical indicators such as positive symptoms.Reference Douglas, Hart and Webster 6 , Reference Hare 7 Additionally, discharge is often dependent on the opinion of forensic evaluators and finders of fact, rather than the treatment team. 8 , 9 Treatment planning for individuals who are committed to a forensic hospital until they can be safely treated in the community should therefore focus upon violence risk assessment and mitigation, rather than multiple foci related to attainment of recovery, as the former approach hastens transfer to the next level of care, lessens risk to other patients and staff, and prevents the accumulation of further legal charges. In this respect, violence, conceptualized dimensionally as a specific syndrome with multiple etiologies, should be the focus of care.
Treatment Planning for Restoration of Trial Competence
Competency evaluations number in the tens of thousands per year,Reference Skeem, Golding, Berge and Cohn 10 , Reference Fogel, Schiffman, Mumley, Tillbrook and Grisso 11 and anecdotal evidence suggests that the number of patients referred to state hospitals for restoration is rising. Research at the University of California–Davis indicates that patients determined to be incompetent can be separated into 6 groupsReference McDermott, Warburton and Woofter 12 (see Table 1). Using this schema, the case formulation should focus on the primary barrier to competency, and discharge criteria should focus on the elimination of that barrier. Like the treatment of violence, incompetency should be viewed dimensionally and as the primary focus of forensic treatment for this commitment category.
Table 1 Competency groups

A Forensic-Focused Treatment Planning Model
Forensic-focused treatment planning should target the legal reasons for admission and discharge based on the commitment specific statutory language, and forensic interdisciplinary plans of care should focus on the factors that prevent discharge from a legal perspective. The goal of a forensic-focused treatment plan is thus to identify, organize, and track foci and treatment that specifically relate to either the barrier to competency, or the etiology and dynamic risk factors for violence, or in some cases both. While the forensic admission and discharge criteria should be the foundation for treatment planning, treatment should proceed with an understanding of the increasing complexity of the new forensic patient that results from the interplay between psychiatric illness, substance abuse, cognitive impairment, and criminogenic thinking. However, not all domains need to be addressed in every forensic patient; for example, a treatment plan that targets substance use in a patient found incompetent to stand trial may not be as critical as interventions focused on the primary barrier to competency.
There are three primary components to consider when developing a Forensic-Focused Treatment Plan:
-
1. Forensic case formulation
-
2. Forensically driven discharge criteria
-
3. Forensic interdisciplinary plans of care
Each component is developed one at a time to generate the information sequentially needed to develop the next component on the list. First, information from the forensic case formulation is used to generate the forensically driven discharge criteria. Second, discharge criteria are used to generate the objectives and interventions that make up a forensic interdisciplinary plan of care (see Figure 1). Finally, the cycle continues such that information in all 3 components is updated on a regular basis as clinically indicated in order to continue progress toward discharge.
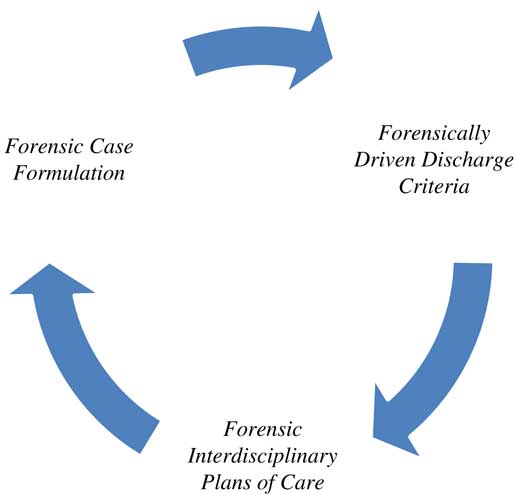
Figure 1 Forensic focused treatment plan cycle.
Forensic case formulation
Integrating forensic data into a case formulation can prove challenging, but there is some guidance in the literature.Reference Hart, Sturmey, Logan and McMurran 2 – Reference Davis 5 , Reference Skeem, Golding, Berge and Cohn 10 – Reference McDermott, Warburton and Woofter 12 In particular, the research literature supports the utility of structured risk assessment, etiology, and diachronicity as helpful components of a forensic case formulation.Reference Hart, Sturmey, Logan and McMurran 2 , Reference Nolan, Czobor and Roy 13 , Reference Quanbeck, McDermott, Lam, Eisenstark, Sokolov and Scott 14
For patients, such as those found “not guilty by reason of insanity” or classified as a “mentally disordered offender,” whose sole discharge criterion is often simply the ability to be safely treated in the community, utilization of a structured clinical risk assessment that delineates risk factors into historical, clinical, and risk management domains can provide a useful framework.Reference Douglas, Hart and Webster 6 An examination of past violence to determine the etiology (psychotic, impulsive, predatory)Reference Nolan, Czobor and Roy 13 , Reference Quanbeck, McDermott, Lam, Eisenstark, Sokolov and Scott 14 allows for further refinement of the formulation. Recent guidelines for treatment based on etiology have been developed.Reference Stahl, Morrissette and Cummings 15 A critical component of a forensic case formulation, identified by Hart et al, is the concept of diachronicity.Reference Hart, Sturmey, Logan and McMurran 2 This means that the forensic case formulation includes information from the patient’s past and present, which generate predictions about the potential future clinical outcomes. The amount of historical information available to forensic clinicians in the form of documentation and evaluations completed during previous hospitalizations varies greatly from case to case, but a case formulation is incomplete and perhaps inaccurate without adequate historical information, especially related to past violence and criminal history. The reliability of information coming from patient self-report should be verified by collateral information whenever possible.
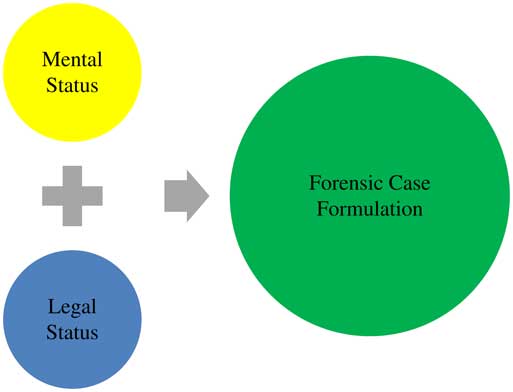
Patients who have been sent for competency restoration have met discharge criteria when they have sufficient present ability to consult with their lawyers with a reasonable degree of rational understanding and have a rational as well as factual understanding of the proceedings against them. 16 Therefore, there is utility in organizing case formulations for these patients into those categories identified by UC Davis, because it provides a focus for treatment on the primary barrier to competency (eg, psychopharmacology intervention for a psychotic barrier to competency). For example, while issues related to substance use or a history of violence may be present, they do not represent a barrier to being discharged as competent, and ironically, incorporating multiple foci of treatment can prolong lengths of stay and ultimately impede upon constitutional rights. 17 The value of a forensic case formulation in these cases is to help clinicians determine what the barriers to regaining competency are and which treatments will be most effective in helping to quickly eliminate those barriers (see Figure 2). Doing so will prioritize forensic outcomes such as restoration of trial competence or mitigation of violence risk as the first steps in a continuum of care that eventually leads to the patient’s ability to resolve forensic issues and return to the community for recovery-oriented care.

Figure 2 Forensic case formulation components.
Forensically Driven Discharge Criteria
The term “discharge criteria” is somewhat of a misnomer, given that a forensic mental health system is only the first step along a continuum of care. Typically, discharge criteria are generated from the case formulation and directly influence the development of interdisciplinary plans of care. However, in the forensic setting, discharge criteria flow from the statutory language under which the patient is admitted. The case formulation should provide, primarily, an analysis of an individual’s mental condition as it relates to that legal status. So the discharge criteria need to reflect resolution of the mental health/criminogenic dimensions that have bearing on the patient’s legal status. Many stakeholders are involved in developing discharge criteria; however, unlike civil settings, it is ultimately the committing court that makes a decision regarding discharge. It is therefore suggested to design discharge criteria that speak directly to the statutory language (see Table 2) and are organized following the structure in the forensic case formulation.
Table 2 Statutory language for incompetent to stand trial

Forensic Interdisciplinary Plans of Care
The principles of good treatment planning apply to forensic plans. KennedyReference Kennedy 18 identifies several mechanics that are essential to treatment planning. Focus statements, objectives, and treatment interventions, developed by a multidisciplinary team of clinicians, should come together to form interdisciplinary plans of care, which serve as the functional components of a forensic-focused treatment plan. In treatment plans, focus statements should clearly articulate the problem. Whether it is medication noncompliance in a patient with psychotic aggression or a need to develop pro-social thinking, a succinct focus statement is crucial to gaining understanding among all readers. Objectives that are behavioral, observable, and/or measurable ensure that forensic clinicians can appropriately track the patient’s progress toward meeting desired outcomes. Attaching reasonable target dates to objectives provides a mechanism by which to establish the continued review of progress. Group, individual, and milieu treatment interventions are also important in establishing exactly what therapeutic modalities and strategies that staff will provide in order to assist the patient in meeting their goalsReference Kennedy 18 (see Table 3).
Table 3 Forensic interdisciplinary plans of care

Unlike civil treatment plans, forensic care plans should focus on mitigation of dynamic risk factors or elimination of the specific barrier to competency, depending on the commitment language.
Conclusions
No significant literature explicitly discusses the unique treatment planning needs for forensic psychiatry patients. Due to the increasing number of such forensic patients, there is a need for a new conceptual treatment planning model that takes into account the criminal justice requirements that must be met in order for patients to either be safely treated in the community or returned to court for trial. More research must be conducted on the efficacy of a model that incorporates a forensic viewpoint when assembling a case formulation, discharge criteria, and interdisciplinary plans of care for these patients.
Disclosures
Robert Schaufenbil, Rebecca Kornbluh, and Katherine Warburton do not have anything to disclose. Stephen M. Stahl, MD, PhD is an Adjunct Professor of Psychiatry at the University of California, San Diego School of Medicine, Honorary Visiting Senior Fellow at the University of Cambridge, UK and Director of Psychopharmacology for the California Department of State Hospitals. Dr. Stahl receives research support from Avanir, CeNeRx, Forest, Genomind, Lilly, Janssen, Mylan, Mylan Specialty, Otsuka, Pamlab, Servier, Shire, Sunovion, and Takeda; is a consultant/advisor to Avanir, BioMarin, Depomed, Forest, Genentech, Genomind, GlaxoSmithKline, Jazz, Merck, Navigant, Novartis, Noveida, Neuronetics, Orexigen, Otsuka, Pamlab, Reviva, Roche, Shire, Sunovion, Taisho, Teva, and Trius; is on the speakers bureaus of Arbor Scientia, Genomind, Janssen, Lilly, Pamlab, Pfizer, Sunovion, and Takeda; and is a board member at Genomind and RCT Logic.