Self-care involves both the ability to care for oneself and the performance of activities necessary to achieve, maintain, or promote health and well-being. Both concepts are part of Orem’s Self-Care Deficit Theory, in which the practice of those activities aimed to maintain life, health and well-being is known as self-care itself, and the ability to engage in the operations required for self-care is defined as self-care agency (Orem, Reference Orem1971; Reference Orem1995).
Self-care agency consists of three types of components: foundational, enabling, and operational (Orem, Reference Orem1971; Reference Orem1995). Foundational components are the most basic capabilities for self-care regarding sensation, perception, memory, and orientation. Enabling capabilities are the power components of self-care. These enabling components are specific capabilities necessary for the realization of self-care activities and presupposes them in time, such as the ability to acquire knowledge about self-care resources, or the physical energy for self-care. The last component, operational capabilities are the productive operation of self-care, for example injecting insulin to manage diabetes.
Several studies have found significant associations between self-care agency, health promotion behaviors and well-being (Cocchieri et al., Reference Cocchieri, Riegel, D’Agostino, Rocco, Fida, Alvaro and Vellone2015; Sundsli, Espnes, & Söderhamn, Reference Sundsli, Espnes and Söderhamn2013) supporting the Orem’s self-care agency definition. Regarding older people such significant associations take on a greater meaning, inasmuch as health promotion is a key factor for achieving an active and healthy ageing (World Health Organization, 2015). Self-care agency, besides health promotion and disease management, offers the possibility for an independent and autonomous living (Räsänen, Kanste, Elo, & Kyngäs, Reference Räsänen, Kanste, Elo and Kyngäs2014) which is one of the major constituents of healthy ageing (Paúl, Ribeiro, & Teixeira, Reference Paúl, Ribeiro and Teixeira2012). In this sense, self-care agency may be one of the major factors involved in active and healthy ageing, becoming a concept especially relevant for older adults (Lommi, Matarese, Alvaro, Piredda, & De Marinis, Reference Lommi, Matarese, Alvaro, Piredda and De Marinis2015). In the last decades, as a consequence of the demographic change, the proportion of older population is experiencing a rapid increase, which has many important health consequences, including the increase of long-term health problems, chronic conditions, and disability, among others. These conditions can be better managed with a greater capacity of self-care, which can lead to a greater control and management of health, and an increased likelihood of performing activities associated with health promotion (WHO, 2015). For that reason, it is important to measure self-care ability among older adults, particularly in the healthcare field. Moreover, the validation of self-care instruments in older adults may help to achieve the challenge of considering self-care as a variable to measure when caring for older patients.
One of the main instrument to assess self-care agency is the Appraisal of Self-care Agency scale (ASA) (Evers et al., Reference Evers, Isenberg, Philipsen, Brouns, Halfens, Smeets and Stinson1986). This scale was developed based on Orem’s theory and aims to measure the power components of self-care agency. The ASA scale has been widely used among general population (Damásio & Koller, Reference Damásio and Koller2013; Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010) and among older people and chronic patients (Fernández & Manrique-Abril, Reference Fernández and Manrique-Abril2011; Fex, Flensner, Ek, & Söderhamn, Reference Fex, Flensner, Ek and Söderhamn2012, Guerra-Stacciarini & Pace, Reference Guerra-Stacciarini and Pace2014).
The ASA is a 24-item scale and each item is responded to on a five-point Likert type scale ranging from 1 (totally disagree) to 5 (totally agree) and with a total score that ranges from 24 to 120. The higher the score, the better the self-care agency. In 2010, Sousa et al. proposed a revised version, known as Appraisal of Self-Care Agency – Revised (ASA-R). This short version consists of 15 items that are scored as in the original scale and with a total score that ranges between 15 and 75. Both versions of the scale have been validated in studies conducted in Brazil (Damásio & Koller, Reference Damásio and Koller2013), Colombia (Manrique-Abril, Fernández, & Velandia, Reference Manrique-Abril, Fernandez and Velandia2009), Hong Kong (Fok, Alexander, Wong, & McFadyen, Reference Fok, Alexander, Wong and McFadyen2002), Mexico (Gallegos, Reference Gallegos1998), The Netherlands (van Achterberg et al., Reference van Achterberg, Lorensen, Isenberg, Evers, Levin and Philipsen1991), Norway (Lorensen, Holter, Evers, Isenberg, & van Achterberg, Reference Lorensen, Holter, Evers, Isenberg and van Achterberg1993), Switzerland (Söderhamn, Evers, & Hamrin, Reference Söderhamn, Evers and Hamrin1996), and United States (Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010) but it has not been validated for Spanish population yet.
The psychometric properties of the original scale –ASA- were evaluated by the authors (Evers et al., Reference Evers, Isenberg, Philipsen, Brouns, Halfens, Smeets and Stinson1986) with content validity (panel of experts) and reliability (α ranged from .77 to .92). Subsequently, other researchers assessed its reliability (α ranged from .72 to .90) (Fok et al., Reference Fok, Alexander, Wong and McFadyen2002; Manrique-Abril, Fernandez, & Velandia, Reference Manrique-Abril, Fernandez and Velandia2009; Sousa, Zauszniewski, Zeller, & Neese, Reference Sousa, Zauszniewski, Zeller and Neese2008; Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010). Recent studies have also examined the psychometric properties of the 15-item ASA-R. In 2013, Damásio and Koller analyzed the convergent validity demonstrating adequate levels, and an adequate α coefficient for each subscale (higher than .78). On the other hand, Sousa et al. (Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010) found a reliability (α = .89) higher than those reported on the original scale.
Regarding the dimensional structure of ASA several factor solutions have been found. According to the authors, the scale is a one-dimension measure (Evers et al., 1986). The same structure was reported by Sousa et al., (Reference Sousa, Zauszniewski, Zeller and Neese2008) through an exploratory factor analysis (EFA) with a sample of 141 American adults. Previously, Söderhamn and Cliffordson (Reference Söderhamn and Cliffordson2001) obtained a five-factor structure of the Swedish version of the scale using confirmatory factor analysis (CFA) with a sample of 125 older people. In 2002, Fok et al. performed an EFA of the Chinese version of ASA which was modified including 8 more items to the original scale. The results found a seven-factor structure. Later, Manrique-Abril et al. (Reference Manrique-Abril, Fernandez and Velandia2009) obtained a nine-factor solution using EFA in a sample of 201 of Colombian chronic patients.
On the other hand, the structure of the 15-item version of ASA has been also analyzed -using EFA and CFA- by two studies which found the same factor solution. The authors of the 15-item ASA-R (Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010) obtained a three-factor structure in a sample of 629 individuals from the United States. The resultant factors were labeled: 1) Having capacity for self-care, 2) Developing capacity for self-care, and 3) Lacking capacity for self-care. This factor solution accounted for 61.7% of the total explained variance. Later, Damásio and Koller (Reference Damásio and Koller2013) conducted a study with a similar sample (N = 627) of Brazilian population. A three-factor structure was reported for ASA-R, explaining 53.54 % of the total variance. Both studies have also demonstrated an excellent construct validity of the instrument.
However, no studies of factor analysis of ASA or it revised 15-item version in Spanish population have been carried out so far. Therefore, the aims of the present study are: a) to adapt and validate the ASA-R scale for use in Spanish population; b) to examine the dimensionality, validity and reliability –using CFA- of the ASA-R scale in a sample of Spanish older people for whom self-care agency is a determinant factor; and c) to establish the convergent validity of the ASA-R using the Short Form Health Survey Version 2 (SF-12v2).
Method
Participants
Consecutive patients who visited two healthcare centers from two districts of Valencia (Spain) were approached between March 2015 and August 2015. Those that met inclusion criteria (being 65 years or older Footnote 1 , living independently, lacking any cognitive impairment, and being able to provide informed consent), were invited to participate in the study. Of them, 69.7% accepted. Home visits were then scheduled -through a phone call- with each participant. Data were collected at the participant’s homes by one interviewer and each home visit lasted between 20 minutes and 30 minutes.
The final sample consisted of 488 home-dwelling older adults. From those, 307 were women (62.9%). Ages ranged from 65 to 92, with an average age of 77.4. More than half of the sample was married (56%) and 30% was widow, and had, at least, completed primary studies (78.7%). The majority of the sample had a net monthly household income lower than 1200€ (60%).
Instruments
Appraisal of Self-Care Agency – Revised (ASA-R; Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010)
This 15-item scale is a revised version of the original 24-item ASA scale (Evers et al., Reference Evers, Isenberg, Philipsen, Brouns, Halfens, Smeets and Stinson1986). It measures the self-care agency using a 5-point Likert scale. As there was no official Spanish version of the ASA-R at the time the study was conducted, a Spanish version (see Appendix 1) was developed using back translation method. The back translation method used was based on the methodology proposed by Brislin (Reference Brislin1970), which is one of the most widely used translation method, particularly in translating international scales, questionnaires and other diagnostic and research instruments. The back translation method has also been promoted by bodies such as the WHO Footnote 2 . The process followed in our study was: 1) Two bilingual translators, both familiar with the scale terminology, translated the items of the original English version of the ASA-R scale into Spanish (forward translation). This translation was not a literal translation of each item but a conceptual translation; 2) as a second step, other two different bilingual translators translated the Spanish version of the ASA-R back to English (back translation), not finding any discrepancies. The back translation step followed the same approach as the forward translation (first step) emphasizing the conceptual equivalence and not linguistic or literal equivalence. Since no discrepancies were found, the authors of this study verified the semantic equivalence of the translated Spanish version of ASA-R scale to the original English version of the scale.
Moreover, after the back translation procedure, the Spanish version of ASA-R was tested for suitability (grammar and reading comprehension) in a sample of 5 older adults.
The Spanish version of 12-items Short-Form Health Survey Version 2 (SF-12v2; Vilagut et al., Reference Vilagut, Valderasa, Ferrera, Garina, López-García and Alonso2008) is a reliable and valid instrument for measuring health status, physical and mental well-being. It consists of 12 items which are rated on a 5-point Likert scale. The items are condensed in eight dimensions of health outcomes, including general health, physical functioning, role physical, role emotional, bodily pain, mental health, vitality and social functioning. It also offers a physical component summary and a mental component summary, which had demonstrated high internal consistency in our sample (.88 and .73, respectively).
Procedure
The questionnaire was administered by trained interviewers in person at the participant’s homes. This study was approved by the Ethics Committee of Consorcio Hospital General Universitario de Valencia.
Data analysis
Firstly, CFA was carried out using the EQS program (version 6.2) to test the fit of the 15-item ASA-R Three-Factor Model (Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010) for the whole sample (N = 488). Generalized Least Squares (GLS, ROBUST) was employed to estimate the model. The specification ROBUST corrects the presence of normality violations (Bentler, Reference Bentler2006).
The goodness of fit of the model to the data was evaluated through the estimated factor loadings which are significant when associated t-values are greater than 1.96, and using the following statistics: Satorra-Bentler Chi-square (S-Bχ2), Root Mean Square Error of Approximation (RMSEA), Standardized Root Mean Square Residual (SRMR), Goodness of Fit Index (GFI), Adjusted Goodness of Fit Index (AGFI), Comparative Fit Index (CFI), and Non-Normed Fit Index (NNFI). According to Jöreskog and Sörbom (Reference Jöreskog and Sörbom1996) overall model fit is acceptable if: the probability of S-Bχ2 > 0.05, RMSEA is closer to 0, and GFI and AGFI are close to 1. The acceptable criterion values for the other fit indices are: SRMR < 0.08, CFI ≥ 0.95, and NNFI ≥ 0.95 (Hu & Bentler, Reference Hu and Bentler1999).
Discriminant and convergent validity of the model were assessed using Average Variance Extracted (AVE). Discriminant validity of the construct considered occurs when the square root of the AVE between each pair of factors is higher than the estimated correlation between those factors. On the other hand, AVE values higher than 0.5 indicate good convergent validity (Hair, Black, Babin, & Anderson, Reference Hair, Black, Babin and Anderson2010).
Finally, the reliability (internal consistency) of the scale was demonstrate by Composite Reliability (CR) indices > 0.7 (Hair et al., Reference Hair, Black, Babin and Anderson2010). Convergent validity of the scale was tested through Pearson’s correlation between the ASA-R factors and the SF-12 subscales.
Results
Dimensionality
CFA was used to test the fit of the 15-item ASA-R Three-Factor Model. Three dimensions were obtained: having capacity for self-care, developing capacity for self-care and lacking capacity for self-care. As presented in Table 1, all fit measures revealed appropriate values: the probability associated with S-Bχ2 was higher than 0.05 (0.436), RMSEA was closer to 0 (0.006), SRMR was lower than 0.08 (0.065), GFI and AGFI were close to 1 (0.924 and 0.921), and CFI and NNFI were higher than 0.95 (0.996 and 0.995). Thereby, indicating that the 15-item three-factor model (Figure 1) had a very good fit.
Table 1. Goodness of fit indexes of the model (N = 488)

Note: S-Bχ2 = Satorra–Bentler Chi-square; p = probability of S-B χ2; RMSEA = Root Mean Square Error of Approximation; SRMR = Standardized Root Mean Square Residual; GFI = Goodness of Fit Index; AGFI = Adjusted Goodness of Fit Index; CFI = Comparative Fit Index; NNFI = Non-Normed Fit Index.

Figure 1. Structural model of ASA-R.
As shown in Table 2, convergent validity of the three-factor model was demonstrated in two ways. First because the AVE for each of the factors was higher than 0.5, and also because factor loadings were significant and higher than 0.5 (Hair et al., Reference Hair, Black, Babin and Anderson2010). On the other hand, discriminant validity was established because the square root of the AVE between each pair of factors is higher than the estimated correlation between those factors, as given in Table 3.
Table 2. Analysis of dimensionality, convergent validity and reliability of ASA-R

Note: AVE = Average variance extracted; CR = Composite reliability; ** p < .01.
Table 3. Discriminant validity of ASA-R

Note: Diagonal: Square root of AVE; below the diagonal: correlation estimated between the factors; **p < .01.
Reliability of ASA-R scale
Reliability was demonstrated because the CR indices of each factor were higher than 0.7 (Hair et al., Reference Hair, Black, Babin and Anderson2010), as shown in Table 2.
Convergent Validity of ASA-R scale
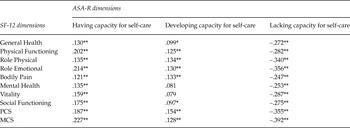
Convergent validity was tested using Pearson’s correlations between the resultant three ASA-R dimensions and the SF-12 subscales. Table 4 shows the Pearson’s correlation results in which the positive dimensions of ASA-R -having capacity and developing capacity for self-care- were positively correlated with SF-12 subscales, while the lacking capacity for self-care dimension showed a negative correlation with SF-12.
Table 4. Convergent validity of ASA-R with the SF-12

Note: PCS: Physical Component Summary; MCS: Mental Component Summary *p < .01; **p < .05.
Discussion
The present study was intended to analyze the psychometric properties of the ASA-R scale in a sample of Spanish older people (>65 years), population in which self-care ability is particularly relevant due to its influence on healthy aging. The CFA of the 15-item ASA-R Three-Factor Model revealed that the three-factor model fitted well to the data. Moreover, the items loaded on the same factors as in the solution found in the two studies that have examined the psychometric proprieties of the ASA-R (Damásio & Koller, Reference Damásio and Koller2013; Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010). Therefore, our findings support the 15-items ASA-R model found in the only two previous studies.
Furthermore, the 15-item ASA-R scale has showed to be a reliable and valid instrument to assess self-care agency. Regarding convergent validity, correlations between the ASA-R and the SF-12 showed a positive correlation between ASA-R positive factors (F1 and F2) and SF-12 subscales and a negative correlation between SF-12 subscales and the negative ASA-R factor, as found by Damásio and Koller (Reference Damásio and Koller2013).
All SF-12 dimensions were positively related to having capacity for self-care. The relationship between self-care agency and well-being has been established in several studies (Damásio & Koller, Reference Damásio and Koller2013; Sundsli, Söderhamn, Espnes, & Söderhamn, Reference Sundsli, Söderhamn, Espnes and Söderhamn2012; Reference Sundsli, Söderhamn, Espnes and Söderhamn2014). This association may be explained because people with greater self-care capacities are more able to care for themselves and carry out health-promoting behaviors, having a positive impact on both physical and mental health, and consequently in well-being. At the same time, there is also evidence that indicates that interventions promoting well-being can improve health-promoting behaviors (Peterson et al., Reference Peterson, Charlson, Hoffman, Wells, Wong, Hollenberg and Allegrante2012). That can be explained because people who have greater well-being are more likely to engage in health-promoting behaviors which may increase the perception of self-care ability (Damásio & Koller, Reference Damásio and Koller2013). Thus, the relation between self-care and well-being is likely bidirectional and synergistic, as it is between health and well-being (Boehm, Vie, & Kubzansky, Reference Boehm, Vie and Kubzansky2012).
On the other hand, developing capacity for self-care showed a positive correlation with general health, physical functioning, role physical, bodily pain, role emotional, social functioning and both physical and mental component summaries. Except from role emotional and social functioning, this factor was more closely related to the SF-12 physical dimensions which could be explained because its items are more related to physical and preventive actions, such as changing old habits to improve health (item 8) or taking measures to ensure safety (item 9). However, Damásio and Koller (Reference Damásio and Koller2013), who tested the convergent validity of ASA-R using SF-36, found no correlation between this factor and these physical dimensions.
Finally, the negative association between lacking capacity for self-care and the all SF-12 dimensions indicated that this factor is directly related with a poor perception of health, as stated in other studies (Damásio & Koller, Reference Damásio and Koller2013; Pender, Murdaugh, & Parsons, Reference Pender, Murdaugh and Parsons2011). Moreover, the correlation coefficient values of this Factor 3, as well as Factor 1 were higher than those from the other Factor 2, indicating that these factors seem to be more determinant for physical and mental health.
In conclusion, this study is considered an important contribution to the study of the ASA scale, as it shows that ASA-R is a reliable and valid instrument to assess the self-care agency among Spanish older population.
However, there are several limitations in this study. Although the sample size was adequate to carry out psychometric analysis of ASA-R, it is based only on a Spanish region which does not permit the results to be generalized for Spanish population. Another limitation is the lack of prior research studies testing the psychometric properties of ASA-R. Only two studies (Damásio & Koller, Reference Damásio and Koller2013; Sousa et al., Reference Sousa, Zauszniewski, Bergquist-Beringer, Musil, Neese and Jaber2010) have analyzed this instrument and neither of the two is based on older adult’s population, which makes difficult to compare our results with previous findings.
As future recommendations, the authors suggest to conduct replication and extension studies on the validity of the Spanish version of the ASA-R in other Spanish regions, as well as with general population and not only in older adults. Regarding the use of this scale in research, the Spanish version of ASA-R can be used to collect baseline and outcome data when implementing interventions in Spanish population aimed to enhance the capability to perform health-promotion behaviors or to manage chronic conditions; and in clinical practice, this version of the scale can be a useful instrument to detect patients within the Spanish healthcare system with low ability to self-care, which may be an indicator of poor health behaviors or inadequate management of chronic diseases.
Appendix 1
Escala de Valoración de la Capacidad de Autocuidado (ASA-R)

Appendix 2
Descriptive statistics

Appendix 3
Items correlation matrix