


Introduction
Vocal process granulomas are benign, inflammatory lesions located over the vocal process of the arytenoid cartilage. Other terms for this entity include laryngeal contact ulcer, contact granuloma, laryngeal granuloma, vocal fold granuloma and post-intubation granuloma.Reference Shin, Watanabe, Oda, Umezaki and Nahm1–Reference Miko4 Hoffman et al. suggest that contact ulcers represent an early stage of granuloma and that ‘vocal process granuloma’ is the most inclusive anatomical term for this pathological entity.Reference Hoffman, Overholt, Karnell and McCulloch5 We agree, and will use the term vocal process granuloma throughout this paper.
The differential diagnosis for vocal process granuloma is extensive and includes reactive, inflammatory, neoplastic and infectious aetiologies. There are many aetiologies of vocal process granuloma, including laryngopharyngeal reflux, vocal abuse, chronic throat clearing and cough, infection, and intubation trauma.Reference Delahunty and Cherry6–Reference Koufman9 The appearance of granulomas is varied and may include ulcerative, pedunculated, sessile, erythematous or white lesions. They may be uni- or bilateral. Histopathological analysis of vocal process granuloma reveals squamous hyperplasia with a proliferation of capillaries, fibroblasts, collagen fibres and leukocytes.Reference Wenig and Heffner10, Reference Luzar, Gale, Klopcic and Fischinger11
Many forms of treatment have been advocated for vocal process granuloma, including voice rest, anti-reflux medication, systemic corticosteroids, inhaled corticosteroids, voice therapy, antibiotics, botulinum toxin injection, medialisation laryngoplasty and surgical excision.Reference Hoffman, Overholt, Karnell and McCulloch5,Reference Koufman8,Reference Devaney, Rinaldo and Ferlito12–Reference Bloch, Gould and Hirano20 Treatment of vocal process granuloma, however, is frequently challenging, with discouraging and unpredictable results. Recurrence rates after surgical resection have been reported to be as high as 88 per cent.Reference Jaroma, Pakarinen and Nuutinen19, Reference Bloch, Gould and Hirano20 Treatment failure may be due in large part to the diversity of causes of vocal process granuloma.
A significant challenge to the evaluation of treatment success, however, is the absence of a universal staging system to accurately classify vocal process granuloma. Clinical experience suggests that small granulomas respond to conservative voice and anti-reflux therapy. Larger vocal process granulomas often require concurrent surgical excision. A valid grading system may assist with the accurate evaluation of treatment efficacy. The purpose of this investigation was to introduce, and to evaluate the intra- and inter-rater reliability of, an endoscopic grading system for vocal process granuloma.
Methods
Permission to conduct this study was obtained from the institutional review board at the University of California, Davis.
Digital images of vocal process granulomas were randomly abstracted from a clinical database of laryngeal photographs (iPhoto 6.0.3, Apple Computer Inc, Cupertino, California, USA). Granulomas were graded on a one to four system, as follows: grade one, sessile, non-ulcerative granuloma limited to the vocal process; grade two, pedunculated or ulcerated granuloma limited to the vocal process; grade three, granuloma extending past the vocal process but not crossing the airway midline in the fully abducted position; and grade four, granuloma extending past the vocal process and past the airway midline in the fully abducted position (see Table I and Figure 1). The granulomas were additionally graded as A if unilateral and B if bilateral. In the case of bilateral granulomas, the larynx was upgraded to the side with the largest lesion.
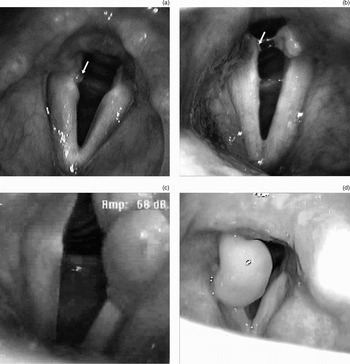
Fig. 1 (a) Grade 1A right vocal process granuloma (white arrow). The granuloma is sessile, non-ulcerated and limited to the vocal process. (b) Grade 2B left vocal process granuloma. The granuloma is sessile, ulcerated and limited to the vocal process. There is subtle ulceration of the right vocal process (white arrow), upgrading this lesion to a ‘B’ classification. (c) Grade 3A left vocal process granuloma. The granuloma is pedunculated and non-ulcerated, extends past the vocal process and obscures <50 per cent of the endoscopic airway. (d) Grade 4A right vocal process granuloma. The granuloma is pedunculated and non-ulcerated, extends past the vocal process and obscures >50 per cent of the endoscopic airway.
Table I grading system for vocal process granuloma
All identifying information was removed from the images. Two faculty laryngologists and two otolaryngology residents (in their third and fifth postgraduate years) analysed each image independently on two different occasions separated by at least 72 hours. The examiners graded the granulomas based on the proposed grading system. The inter- and intra-rater reliability of the grading system was determined using the kappa (κ) test.
Results
The digital vocal process granuloma database consisted of 35 images. The percentage intra-observer agreement for the two laryngologists was 97 and 100 per cent (κ = 0.94 and 1.00, respectively). The percentage inter-observer agreement between the two laryngologists was 91 per cent (κ = 0.83). The percentage intra-observer agreement for the two residents was 89 and 91 per cent (κ = 0.83 and 0.77, respectively). The percentage inter-observer agreement between the two residents was 83 per cent (κ = 0.67). The percentage inter-observer agreement between laryngologist and resident was 89 per cent (κ = 0.77). There was no difference in agreement, comparing the laryngologists and the residents (p > 0.05).
Discussion
Since the first description by Chevalier Jackson in 1928, much has been written and hypothesised about the origin and treatment of vocal process granuloma.Reference Jackson21 To our knowledge, there has not been a previously described endoscopic grading system for this disorder. Various authors have sub-classified these lesions by presumed aetiology from reflux, intubation or contact ulceration. Treatment strategies for vocal process granuloma include voice rest, voice therapy, anti-reflux medication, antibiotics, steroids, botulinum toxin injection, vocal fold augmentation, surgical resection and even irradiation.Reference Hoffman, Overholt, Karnell and McCulloch5,Reference Koufman8,Reference Devaney, Rinaldo and Ferlito12–Reference Bloch, Gould and Hirano20, Reference Harari, Blatchford, Coulthard and Cassady22 These treatment modalities have given highly variable responses. Such variability is likely to be secondary to the numerous aetiologies involved in granuloma formation. Some of this variability, however, may be secondary to the grouping of vocal process granulomas of different sizes and characteristics into a single analysis.
• Vocal process granuloma has many aetiologies, including laryngopharyngeal reflux, vocal abuse, chronic throat-clearing and cough, infection, and intubation trauma
• Multiple treatment modalities are available, with variable success
• There is no standardised grading system for vocal process granuloma
• The vocal process granuloma grading system presented offers a standardised method for describing the endoscopic appearance of these lesions, and has excellent intra- and inter-rater reliability
• Further study is needed to determine if this grading system is useful for assessing treatment outcomes and assigning prognosis for vocal process granuloma
With the continued evolution and sophistication of digital optics and fibre-optic telescopes, the ability to visualise and characterise lesions of the glottis continues to improve. Our current office laryngoscopes allow accurate determination of lesion size, location, colour, ulceration and attachment (sessile or pedunculated). We have proposed a new, simple staging system for classifying vocal process granulomas, based on those characteristics. In our study, this endoscopic grading system demonstrated excellent inter- and intra-rater reliability at both a consultant and a resident level. This standardised classification system allows a more uniform description of vocal process granuloma.
Our proposed vocal process granuloma classification system may be useful in evaluating treatment outcomes; however, this requires further study. It is not yet clear if the grading system will allow the clinician to choose optimal treatment strategies or to predict prognosis. Other limitations of the current study include the retrospective nature of the data and the fact that it was conducted within a single institution.
Conclusions
We have introduced and evaluated a new endoscopic grading system for vocal process granuloma. This grading system displayed excellent intra- and inter-observer reliability among otolaryngology residents and experienced laryngologists. Further study is needed to determine if this grading system can be used for determining prognosis or treatment outcomes.


