The Ebola epidemic has prompted health care professionals to question the scope of their obligations to care for patients with this contagious and deadly disease in both epidemic and nonepidemic settings. Treating patients with Ebola virus disease (EVD) in Africa has already resulted in the infection of 830 health care workers and the deaths of 488. 1 The infection has also spread to at least 3 health care workers caring for patients with EVD in the United States and Europe, all of whom have recovered. 2 Even in nonepidemic settings, such risks create a moral predicament for clinicians whose training and conscience urges them to treat all patients, but who understandably fear for their lives as well as the lives of their families, close personal contacts, and their other patients. Similar concerns have accompanied other recent epidemics including HIV,Reference Freedman 3 , Reference Arras 4 multidrug-resistant tuberculosis, and severe acute respiratory syndrome.Reference Brody and Avery 5 In these other epidemics, careful reasoning and argumentation concluded that there is a general professional obligation to treat. However, the facts and fears associated with Ebola have reopened such questions. Addressing these issues is especially important as anecdotal reports suggest that at least some health care professionals have refused or may refuse to care for patients in nonepidemic settings.Reference Govan 6 , Reference Feintzeig 7
Professional codes of ethics and societal expectations indicate that physicians have an obligation to treat all patients, including those who pose a risk to them. In assuming their roles as professionals, physicians implicitly promise to adhere to these values.Reference Wynia, Papadakis and Sullivan 8 , Reference Cruess, Cruess and Johnston 9 Stated differently, physicians have a fiduciary obligation to treat patients.Reference Emanuel 10 - Reference Huber and Wynia 12 That is, physicians are expected to act in ways that privilege the interests and welfare of patients over their own. Nurses similarly have professional obligations to care for patients in a nondiscriminatory fashion. 13 Nevertheless, such obligations are not unconditional. That is, “in certain situations the risks of harm may outweigh a nurse’s moral obligation or duty to care for a given patient.” 14 To help delineate the scope of the obligation to treat patients with EVD in light of the associated risks in nonepidemic settings, in this article we focus on 3 practical areas: (1) minimizing risks, (2) the context of care, and (3) fairness.
MINIMIZING RISKS
The profound consequences of EVD for clinicians and their contacts underscore the duty to reduce the nosocomial risk of transmission. As a starting point, health care systems must ensure that evidence-based measures are in place to protect clinicians.Reference Kortepeter, Smith and Hewlett 15 This includes providing personal protective equipment, rigorous education and training, policies to reduce exposures, and procedures to ensure that safety measures are being properly implemented. To date, the only infections of health care workers in the United States have occurred in 2 nurses who were working outside of a specialized infection control unit. In contrast, none of those staffing these special units have become infected with Ebola. Therefore, to minimize risk, all clinicians arguably should be prepared to recognize and triage patients suspected of having EVD and then safely transfer appropriate patients to those with specialized training. In addition, swiftly providing clinical care to patients with EVD may not only reduce mortality but also decrease the need for invasive interventions that pose additional risk of infection.Reference Ansumana, Jacobsen and Foday 16
Although the risk to clinicians of using invasive interventions (eg, dialysis or extracorporeal membrane oxygenation) can be justified when they are expected to be beneficial, this may not be the case when there is good reason to believe that they pose minimal chance of benefit. For example, resuscitation from an unwitnessed cardiac arrest generally has a very low probability of success and for a patient with EVD could put clinicians at increased risk of infection.Reference Altman 17 , Reference Fins 18 Moreover, because risk minimization demands using personal protective equipment, there can be additional delays in initiating resuscitation, further reducing the likelihood of success. In contrast, using a defibrillator to treat a witnessed, in-hospital arrest in a previously healthy patient will likely have a far higher chance of success as well as be less risky for clinicians, thereby altering the calculus regarding its use.Reference Halpern and Emanuel 19
Accordingly, efforts should be taken to craft protocols regarding the appropriate use of invasive procedures for patients with EVD.Reference Decker, Sevransky and Barrett 20 However, the current paucity of systematic data regarding the benefits and risks involved with particular invasive procedures in this setting suggests that these protocols be revisited as new data become available. These protocols should be vetted widely during development and be made transparent once they have been completed so that they are fairly implemented.
In addition, risk is minimized by employing a small number of specialized centers to provide high-quality care in a very controlled environment where training, oversight, and quality control mechanisms can be constantly reinforced.Reference Kortepeter, Smith and Hewlett 15 At present, these centers also rely upon clinicians volunteering to serve in this capacity, thereby decreasing the number of clinicians working under duress. The risk of psychological harm or anxiety among health care professionals is also significant, and utilizing those willing to serve may help to minimize such risks.
THE CONTEXT OF CARE
The local prevalence of the disease, the nature of the setting, and the availability of effective treatment are also relevant to delineating professional obligations to treat. For instance, if transmission of Ebola were ever to become widespread in the United States, a relatively small number of regional centers that rely solely on clinicians who volunteer to treat patients with EVD would be insufficient. Therefore, clinicians would generally be expected to deliver care.
Further, the risks and burdens for clinicians depend in part upon the context. For example, although protective equipment is required regardless of the setting, donning it in a climate-controlled hospital in the United States is surely different from using it in the treatment centers in hot and humid West Africa. Risks also are generally lowered in the United States by virtue of close proximity to high-quality supportive care, rather than being potentially hundreds of miles and an airlift away.
Further, if and when effective vaccines or treatments become available, the risk context will shift considerably, and the ethical tensions health care professionals would face in caring for patients with EVD should be further reduced.
FAIRNESS
Fairness is also critical in translating health care professionals’ obligations to treat patients with EVD. For instance, optimal care should be provided for clinicians who become infected. In Liberia, a special treatment center, the Monrovia Medical Unit, was built specifically to treat and give the best possible care to Ebola-infected health care workers.Reference Vandiver 21 Further, as with other work-related injuries, clinicians who become infected while delivering care deserve fair compensation when they are off work or if they are quarantined.Reference Wynia and Gostin 22 Likewise, they are entitled to disability and life insurance.
Fairness also demands that the rights and interests of relevant stakeholders be addressed. Accordingly, health systems should have in place a robust process for respectfully and transparently addressing the concerns of health care professionals. Further, institutions have an obligation to disclose their expectations of clinicians, make explicit the processes and protocols that govern practice, outline their scope of commitment to clinicians who become infected, and articulate the consequences to clinicians for failure to fulfill their expected duties. Further, a process for ongoing monitoring of the intended and unintended consequences of such policies should be in place so that, if necessary, revisions to them can be made.
Finally, there must be consideration of the multiplicative effects that disability or death among clinicians can have on health care systems and the services available to the general population. Routine health care in parts of West Africa essentially ceased as the Ebola epidemic spread, leading to the deaths of a large number of people who had no access to routine or emergency care.Reference Dawson 23 Even in nonepidemic settings, treatment of EVD can have ripple effects on other care. For example, if a patient with EVD is treated in an intensive care unit, other beds may have to be closed and surgical cases may need to be postponed. Similarly, if many clinicians are needed to care for a patient with EVD, this may limit the workforce available to care for others. Consequently, careful planning is needed to address these concerns.
MOVING FORWARD
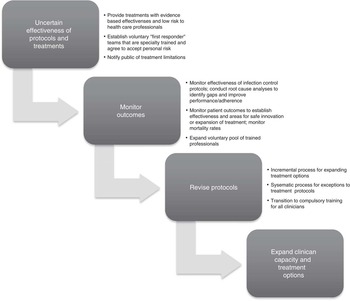
To best translate health care professionals’ obligation to treat patients with EVD into practice, it will be critical to learn from the approaches currently being employed and to modify them based on data. Standard tools derived from quality improvement should be employed to drive policy development involving key stakeholders (see Figure 1). For instance, it will be important to learn if health care professionals in health systems utilizing stringent protective measures become infected. Similarly, it will be necessary to assess the benefits and risks of different treatment modalities and invasive procedures. Such data will be essential in separating facts from fears and thereby help ensure that patients with EVD receive needed medical care.

FIGURE 1 Graded Responsiveness Based on Experience