Introduction
Mortality rates are significantly elevated in individuals with eating disorders, with the highest rate occurring in those with anorexia nervosa (Arcelus et al. Reference Arcelus, Mitchell, Wales and Nielsen2011). The current lifetime prevalence of all eating disorders is about 5% (Treasure et al. Reference Treasure, Claudino and Zucker2010).
In Ireland an estimated 400 new cases of eating disorders emerge each year, representing 80 deaths annually (Department of Health and Children, Ireland 2006). A recent meta-analysis found age at assessment to be a significant predictor of mortality for patients with anorexia nervosa (Arcelus et al. Reference Arcelus, Mitchell, Wales and Nielsen2011). This highlights the need for timely, cost efficient measures to identify at risk individuals in vulnerable populations such as young adult women.
The Eating Disorder Examination (EDE), a semi-structured interview, was developed by Fairburn and Cooper (Reference Fairburn and Cooper1993). Although widely considered the instrument of choice for the assessment and diagnosis of DSM-IV eating disorders (Mond et al. Reference Mond, Hay, Rodgers, Owen and Beumont2004), the EDE requires training, can be time consuming to conduct and is inappropriate for group administration (Luce et al. Reference Luce, Crowther and Pole2008). The self-report version adapted from the EDE, the Eating Disorder Examination Questionnaire (EDE-Q) is a cost-effective alternative that has shown good psychometric properties and can be used to identify probable cases of eating disorders (Mond et al. Reference Mond, Hay, Rodgers and Owen2006). Norms are needed for interpretation of scores. Currently, norms are available in England for young women (1994) (Fairburn and Beglin, Reference Fairburn and Beglin1994; Fairburn et al. Reference Fairburn, Cooper and O’Connor2008) and young adolescent females (2001) (Carter et al. Reference Carter, Stewart and Fairburn2001), in Australia for young adult women (2006) (Mond et al. Reference Mond, Hay, Rodgers and Owen2006), in the United States of America for undergraduate women (2008) (Luce et al. Reference Luce, Crowther and Pole2008) and undergraduate men (2010) (Lavender et al. Reference Lavender, De Young and Anderson2010), in Norway for female university students (2010) (RØ et al. Reference Rø, Reas and Lask2010), in Sweden for young adult women (2011) (Welch et al. Reference Welch, Birgegard, Parling and Ghaderi2011) and in a representative sample of the German population (2012) (Hilbert et al. Reference Hilbert, De Zwaan and Braehler2012).
To our knowledge, no prior studies exist that have published normative scores of the EDE-Q in Ireland. Although current published norms may be applicable to our university population, it is recognised that levels of eating disorder psychopathology may vary across countries (Mond et al. Reference Mond, Hay, Rodgers and Owen2006). Normative data will assist in the interpretation of EDE-Q test scores in both clinical and research settings in those looking to assess eating disorder psychopathology. The purpose of this study is to present prevalence of key eating disorder behaviours and to establish norms for the EDE-Q among female university students in Ireland.
Methods
Participants
The EDE-Q was administered to a consecutive sample of 200 female students attending a university primary health care service over a 1-month period. Nine students did not consent to the study and one student did not complete the questionnaire leaving a total of 190 participants. Written informed consent was obtained from all participants. The study was reviewed and approved by the Ethics Committee of Trinity College, Dublin.
Instrument
The EDE-Q version 6.0 was used in this study. The EDE-Q is a 28-item instrument that focuses on the previous 28 days and measures core eating disorder behaviours. The EDE-Q produces a global score and four subscale scores: restraint, shape concern, weight concern and eating concern.
The global score is the average of the four subscale scores. Responses are rated on a seven-point Likert scale, and higher scores indicate greater disordered eating pathology. A cut-off score of ⩾4 is commonly used to indicate clinical significance (Carter et al. Reference Carter, Stewart and Fairburn2001; Mond et al. Reference Mond, Hay, Rodgers and Owen2006; Luce et al. Reference Luce, Crowther and Pole2008; Lavender et al. Reference Lavender, De Young and Anderson2010).
The frequency of key eating and compensatory behaviours such as objective binge episodes, self-induced vomiting, laxative misuse and excessive exercise are also recorded. Regular occurrence of excessive exercise was defined as exercising ‘in a driven or compulsive way as a means of controlling your weight, shape or amount of fat, or to burn off calories’ (EDE-Q 6.0, item 18) for ⩾20 times over the past 28 days. For regular occurrence, dietary restraint was defined as going ‘for long periods of time (8 waking hours or more) without eating anything at all in order to influence your shape or weight’ (EDE-Q 6.0, item 2) for more than three times per week (⩾13 times) over the past 28 days. For all other behaviours regular occurrence was defined as four or more occurrences over the past 28 days.
Missing data
The scoring methods advised by Fairburn et al. (Reference Fairburn, Cooper and O’Connor2008) were used for the calculation of EDE-Q subscale and global scores. With respect to missing data, 0.3% of the items required to score the EDE-Q subscales were missing. One participant failed to respond to three of the five eating concern questions and so their eating concern subscale was excluded from the analysis. Another participant failed to respond to two items but, otherwise, there were no other participants with more than one missing item. Any missing responses were replaced with the mean item score as done in previous studies using this instrument.
Statistical analysis
All analyses were carried out using Stata, version 12. Our descriptive findings are reported using means, standard deviations and percentile ranks. We used linear regression models to examine the association between EDE-Q items and the body mass index (BMI) of respondents; and EDE-Q items and age of respondents. The association with BMI was examined treating BMI first as a linear variable and subsequently as a categorical variable. For the categorical variable we divided BMI into three categories: (1) <18.5 underweight; (2) 18.5–25 healthy weight and (3) >25 overweight.
Results
The mean age of respondents was 21.9 years (s.d.=4.2 years) with a self-reported BMI of 22.1 kg/m2 (s.d.=3.4 kg/m2). There was no association between EDE-Q global score and age of respondents [b=−0.01, t(177)=−0.75, p=0.45] or between EDE-Q score on any of the subscales and age of respondents [restraint: b=−0.01, t(177)=−0.43, p=0.67; eating concern: b=−0.02, t(177)=−1.12, p=0.26; shape concern: b=−0.01, t(177)=−0.63, p=0.52; weight concern: b=−0.02, t(177)=−0.80, p=0.42].
The mean global EDE-Q score was 1.51 (s.d.=1.28). Means and standard deviations for the EDE-Q, as well as the corresponding percentile ranks for the subscales and global score, are presented in Table 1.
Table 1 EDE-Q descriptive data and percentile ranks for raw EDE-Q global and subscale scores (n=190)

EDE-Q, Eating Disorder Examination Questionnaire.
The frequency of any or regular occurrence of objective binge eating, self-induced vomiting, laxative misuse, excessive exercise and dietary restraint are presented in Table 2.
Table 2 Proportion of women engaging in any or regular occurrence of key eating and compensatory behaviours

OBE=objective binge episodes.
There was an association between BMI and the global EDE-Q score [b=0.1, t(184)=4.45, p<0.0001] as well as between BMI and all the subscales of the EDE-Q [restraint: b=0.05, t(184)=2.08, p<0.05; eating concern: b=0.04, t(184)=1.95, p=0.05; shape concern: b=0.16, t(184)=24.96, p<0.0001; weight concern: b=0.19, t(184)=6.37, p<0.0001]. This evidence indicates that as an individual’s BMI increases, there is a corresponding increase in their EDE-Q score. Results from the regression model with BMI modelled as a categorical model indicates that individuals in the overweight category (BMI>25) have a significantly higher global score on the EDE-Q than individuals who are in the healthy weight category [b=1.1, t(183)=4.24, p<0.0001].
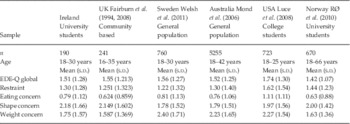
A comparison of our results with other studies that have compiled norms for the EDE-Q are presented in Table 3. Using a cut-off score of ⩾4 to indicate clinical significance, 5.8% of the sample scored in the clinically significant range on the global EDE-Q score.
Table 3 Comparison of female EDE-Q norms

EDE-Q, Eating Disorder Examination Questionnaire.
Discussion
The limitations of self-report measures are well established. A clinical interview is likely to be more accurate than a self-report questionnaire. However, time and resource constraints encourage the use of self-report measures. Studies have shown a high level of agreement between the EDE-Q and the EDE interview in the assessment of attitudinal features of eating disorder psychopathology (Mond et al. Reference Mond, Hay, Rodgers and Owen2006).
In our study BMI was found to be positively associated with EDE-Q scores with overweight individuals (BMI>25) having significantly higher global EDE-Q scores than those in the healthy weight category. This may be reflective of more prevalent bulimic symptoms in the population. Obesity has been associated with both an increased risk of bulimia nervosa (BN) and a worse prognosis (Hay & Claudino, Reference Hay and Claudino2010). A previous primary care study suggested that the health burden of bulimic type eating disorders is substantial but remains largely hidden (Mond et al. Reference Mond, Myers, Crosby, Hay and Mitchell2010).
The mean global EDE-Q score for our sample (1.51) was comparable to mean global scores obtained in previous studies of English (1.55), Australian (1.52) and Swedish (1.56) populations (Mond et al. Reference Mond, Hay, Rodgers and Owen2006; Fairburn et al. Reference Fairburn, Cooper and O’Connor2008; Welch et al. Reference Welch, Birgegard, Parling and Ghaderi2011). We recruited participants attending a university primary health care service. Our study shows substantial levels of disordered eating pathology in undergraduate women with 5.8% of the sample scoring in the clinically significant range on the global EDE-Q score. As individuals with eating disorders have a tendency to conceal their illness and avoid professional help, our sample may represent a false high prevalence compared with those who do not access health care services (Hsu, Reference Hsu1996; Treasure et al. Reference Treasure, Schmidt and Van Furth2003). This point is important as our method of recruitment may influence the generalisability of our findings. In a study of risk factors for eating disorders, only half of their anorexia nervosa sample sought treatment (Hilbert et al. Reference Hilbert, Pike, Goldschmidt, Wilfley, Fairburn, Dohm, Walsh and Striegel Weissman2014). However, it is worth noting that our sample was recruited while attending a primary care service for non-eating disorder related difficulties.
It is concerning that 2.1% of our sample reported regular self-induced vomiting, compared with 2% in the Norwegian university sample (RØ et al. Reference Rø, Reas and Lask2010) and 1.3% and 4.0% in the Swedish and Australian general population samples, respectively (Mond et al. Reference Mond, Hay, Rodgers and Owen2006; Welch et al. Reference Welch, Birgegard, Parling and Ghaderi2011). Regarding dietary restraint, 5.3% of our sample reported regularly going without food for 8 hours or more in order to influence weight or shape, compared with 1.8%, 5.8% and 3.4% in the Norwegian, Swedish and Australian samples, respectively (Mond et al. Reference Mond, Hay, Rodgers and Owen2006; RØ et al. Reference Rø, Reas and Lask2010; Welch et al. Reference Welch, Birgegard, Parling and Ghaderi2011).
The EDE-Q is a useful instrument to aid in the identification of disordered eating pathology. Once identified, the management of eating disorders can prove more problematic for psychiatrists and general practitioners due to limited availability of services. In Ireland, with a population of 4.5 million people, there are only three public specialised eating disorder beds (Central Statistics Office, 2012). The Royal College of Psychiatrists’ (2000) report on eating disorders recommended the provision of six beds per million population for patients over 16 years of age.
Our sample was a consecutive sample of female young adult students aged between 18 and 30 years attending a university primary health care service. Eating pathology tends to emerge in mid to late adolescence with Hudson et al. finding a mean age of onset of 19 years for anorexia nervosa and 20 years for bulimia nervosa (Hudson et al. Reference Hudson, Hiripi, Pope and Kessler2007). Hence, our rationale for selecting a sample aged between 18 and 30 years. Anorexia nervosa has been consistently linked to personality traits such as conformity, perfectionism and obsessive–compulsive features (Westen & Harnden-Fischer, Reference Westen and Harnden-Fischer2001). As this is a third level university sample, it is likely to contain a greater prevalence of high achieving, perfectionistic females and hence is not generalisable to the general young adult female population.
In conclusion, this study presents normative EDE-Q data for an Irish female university sample. Norms are needed for interpretation of EDE-Q scores. In an Irish population with an estimated 200 000 people affected by eating disorders (Department of Health and Children, Ireland 2006), a psychometrically established and cost saving method of quickly assessing core eating disorder psychopathology is valuable. These results may be useful for clinicians and/or researchers in the evaluation of EDE-Q scores in Irish female university students.
Acknowledgement
The authors wish to thank the students who participated in this study.
Conflicts of Interest
None.