



Introduction
Mental health problems have a detrimental effect on various aspects of a person's life, including social relationships, physical health, and career and academic success (Reference Clement, Schauman, Graham, Maggioni, Evans-Lacko and Bezborodovs1). At the moment, stress, anxiety, and depression are the most common psychological problems that cause disability (2;3). Depression has been recognized as one of the most important causes of disability in the world, affecting more than 300 million people (4). The symptoms of depression include loss of enthusiasm, worthlessness, sadness, sleep disorders, anorexia, excessive fatigue, and reduced concentration (Reference Marcus, Yasamy, van Ommeren, Chisholm and Saxena5). Depression affects sleep quality, performance, productivity, and routine activities (Reference Adler, McLaughlin, Rogers, Chang, Lapitsky and Lerner6). Anxiety is also one of the most common mental illnesses in the world, which has approximately affected 29.8 percent of the people (Reference Polanczyk, Salum, Sugaya, Caye and Rohde7). Anxiety has been defined as the body's response to a perceived threat that exacerbates an individual's beliefs, feelings, and thoughts and increases blood pressure, respiration rate, heart rate, sweating, drowsiness, and chest pain (Reference Baxter, Vos, Scott, Norman, Flaxman and Blore8). Stress is an emotion that begins when an individual realizes that demand is more than the available resources (Reference Lazarus9). Over the past decade, stress-related illnesses have been thought to be a reason for increased long-term sick leave in many European countries (Reference Henderson, Glozier and Elliott10). Despite the spread of these diseases, mental health services are limited, and many people do not have access to such services. Approximately 50–78 percent of people with mental health problems are not treated adequately in Europe and the United States (Reference van Orden, Deen, Spinhoven, Haffmans and Hoencamp11;Reference Jörg, Visser, Ormel, Reijneveld, Hartman and Oldehinkel12). The situation is worse in middle- and low-income countries, and more people are deprived of treatment (Reference Demyttenaere, Bruffaerts, Posada-Villa, Gasquet, Kovess and Lepine13;Reference Li, Du, Chen, Song and Zheng14).
The expansion of digital technology has led to an improvement of access to healthcare services (Reference Khademian, Rezaee and Pournik15). Mobile phones with Internet access and the ability to download and launch mobile software applications (apps) offer an affordable and accessible way to provide mental health services, especially in hard-to-reach areas (Reference Aboujaoude, Salame and Naim16). The number of mobile phone users has been expected to reach 1.6 billion worldwide by 2020 (Reference Ericsson17).
The efficacy of medical intervention can be enhanced by increasing user satisfaction and adherence (Reference Lee, Uhm, Cheong, Yoo, Chung and Park18). According to Donkin et al., adherence is defined as “the degree to which the user followed the program as it was designed” (Reference Donkin, Christensen, Naismith, Neal, Hickie and Glozier19). Improving adherence to interventions has always been a challenge for researchers, and they always tried to find factors affecting it. In this regard, a study found that being female, as well as having higher openness to experience, lower resistance to change, or less depressive symptoms were significant indicators for better intervention adherence (Reference Rathbone and Prescott20). Another research has shown that the use of SMS services as a reminder improves adherence to prescription medication (Reference Islam, Lechner, Ferrari, Froeschl, Alam and Holle21). Moreover, a study reported that adherence has improved by human support (support of counselors, peers, and phone and e-mail contact) (Reference Brouwer, Kroeze, Crutzen, de Nooijer, de Vries and Brug22). Besides, research suggests that more personalization of digital interventions can enhance adherence (Reference Ryan, Bergin and Wells23). In addition, some studies showed a high level of satisfaction among mHealth interventions (Reference Lee, Uhm, Cheong, Yoo, Chung and Park18;Reference Knight-Agarwal, Davis, Williams, Davey, Cox and Clarke24;Reference Herring, Cruice, Bennett, Rose, Davey and Foster25). In this regard, the details or specificity of the content, data transmission accuracy, mutual feedback systems, as well as configuration of individualized programs are crucial factors for user satisfaction (Reference Lee, Uhm, Cheong, Yoo, Chung and Park18). Nevertheless, studies reported that perceived quality and usefulness (Reference Kang and Park26), ease of use, ease of navigation, and interactivity (Reference Ohk, Park and Hong27), as well as trust (Reference Zhou28) and human support (Reference Herring, Cruice, Bennett, Rose, Davey and Foster25) had positive effects on user satisfaction.
According to a study, there are more than 15,000 health-related applications, 29 percent of which are related to mental health (Reference Anthes29). Mental health applications increase the incentive to use the services among people who do not like face-to-face visits (Reference Kovandžić, Chew-Graham, Reeve, Edwards, Peters and Edge30). Despite a large number of apps in this domain, it is not easy to find a useful and reliable one, given the fact that the effectiveness of many apps has not been proven scientifically. The research question is: What are the effects of stress, anxiety, and depression-related apps on reduced depression, anxiety, and stress. Therefore, the present study aims to explore the effects of mental health apps on the management of stress, anxiety, and depression symptoms.
Methods
A systematic literature review was conducted in PubMed, Scopus, Web of Science, Cochrane library, and Embase databases for the relevant articles published from 2000 to 2019. The search included a combination of MeSH terms and keywords related to mobile applications, stress, anxiety, depression, and effectiveness. The search was structured according to the PICO framework: P (problem) was depression, anxiety, or stress, I (intervention) was mobile app and web application, C (comparison) was other mHealth initiatives, and O (outcome) was reduced levels of depression, anxiety, or stress. The details of the search strategy have been presented as Supplementary File 1.
The studies were screened in several phases using inclusion and exclusion criteria. At first, all titles and abstracts were screened to remove irrelevant and duplicate studies. Then, full-text copies of all potentially related articles were obtained. The full texts of the papers were also obtained in case their abstracts were insufficient to determine their eligibility. Reference lists of the included articles were also screened, and a search was done in Google Scholar using similar keywords to identify further eligible articles. Next, the full-text articles were screened and were excluded if they did not meet the inclusion criteria. It should be noted that the selection of the eligible articles and completion of the data extraction table were carried out by two authors (FKh and AA) independently, and any disagreement was resolved through discussion.
Eligibility Criteria
All systematic review and meta-analysis studies that assessed the effects of mental health apps on the symptoms of stress, anxiety, and depression were included. The included studies were published in English-language peer-reviewed journals, systematically reviewed mobile apps intervention for their effectiveness in stress, anxiety, and depression, evaluated physical or emotional symptoms of stress, anxiety, and/or depression as one of their primary or secondary outcome measures, and used mobile apps (Android or IOS) or web-based mobile applications as an intervention or as a part of an intervention. There was no limitation regarding the participants’ age or gender.
The studies were excluded if they (i) involved only a computer-based, Internet-based, or text messaging intervention without a mobile app component, (ii) included only a description of the mobile app without the outcome data, (iii) reviewed other mental health symptoms (e.g., schizophrenia, bipolar affective disorder, paranoia, post-traumatic stress disorder, and psychosis), (iv) did not provide outcome measurement scale, and (v) included protocols and conference abstracts.
Methodological Quality of the Reviewed Studies
The methodological quality of the included articles was assessed independently using the Assessment of Multiple Systematic Reviews (AMSTAR) instrument. This validated tool evaluated the degree to which the review methods avoided bias by assessing the methods against eleven distinct criteria (see Table 1). Each item was rated as “yes” (one score) or “no,” “cannot answer,” and “not applicable” (zero scores). The scores could range from 0 to 11. Accordingly, the scores were classified into three categories of low quality (0–3), moderate quality (4–7), and high quality (8–11) (Reference Bashi, Karunanithi, Fatehi, Ding and Walters39). Each included article was independently assessed by two authors (FKh and AA) in terms of methodological quality, and any disagreement was discussed in order to reach consensus. The included studies were of various qualities, but they were mostly of moderate quality according to the AMSTAR tool. In addition, most reviews (n = 8) were of moderate quality, and one was of low quality.
Table 1. Methodological quality of the systematic reviews based on the AMSTAR instrument scores
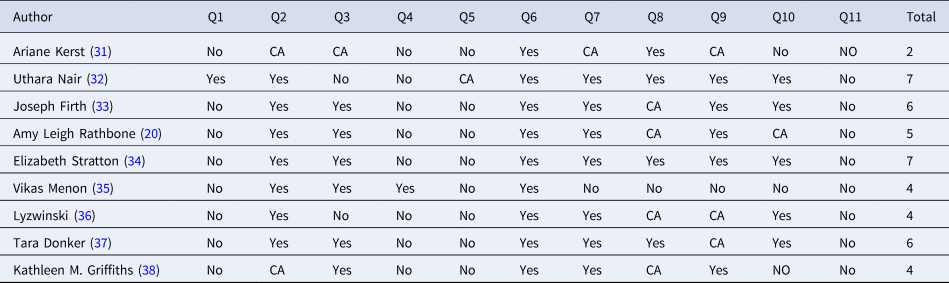
CA, cannot answer; NA, not applicable.
Outcome Measures
The primary outcome measures were changes in stress, anxiety, and depression symptoms, and the secondary outcome measures were effects on satisfaction and adherence rate.
Results
Selection and Inclusion of Studies/Search Results
A total of 4,992 peer-reviewed articles were identified in PubMed (n = 1,220), Scopus (n = 3,352), EMBASE (n = 321), Cochrane (n = 92), and Web of Science (n = 7) databases. After searching the reference lists of the included articles and Google Scholar using similar keywords, seven other articles were added, as well. After removing the duplicates, 4,999 articles were reduced to 4,353. Furthermore, 4,314 articles were excluded after reviewing the titles and abstracts, and full texts of 39 articles were reviewed. After reviewing the full texts, 28 articles were removed because they did not follow the systematic review design (n = 8), did not use application interventions (n = 3), reviewed other mental health symptoms (n = 1), were a conference abstract (n = 1), did not measure stress, anxiety, and depression symptoms (n = 2), were duplicate (n = 2), did not evaluate the effectiveness or efficacy of the apps (n = 3), reviewed the same articles (n = 6), did not provide outcome measurement scale (n = 2), and other reasons (n = 2). Finally, nine systematic reviews were included. The results of the included studies were extracted, reviewed, and reported in a systematic format. The screening process was detailed in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram (Figure 1).

Figure 1. PRISMA flow diagram.
The characteristics of the included systematic reviews are presented in Table 2. A total of nine articles were included in this review, consisting of six systematic reviews and three systematic reviews with meta-analysis. The publication dates of the systematic reviews ranged from 2010 to 2018, with a remarkable increase in the number of publications from 2017; seven systematic reviews were published from 2017 to 2018 (Reference Kerst, Zielasek and Gaebel31–Reference Lyzwinski, Caffery, Bambling and Edirippulige36). According to Supplementary File 2, the maximum number of systematic reviews was found for depression disorders (n = 7). In addition, systematic reviews examined depression, anxiety, and stress (n = 2), depression and anxiety (n = 2), as well as depression and stress (n = 1) simultaneously.
Table 2. Characteristics of the included systematic reviews

* According to our objectives; ACT, acceptance and commitment therapy; BA, behavioral activation; BDI, Beck depression inventory; CBT, cognitive behavioral therapy; CBM, cognitive bias modification; CC, cognitive control; DASS, depression anxiety stress scales; EPDS, Edinburgh postnatal depression scale; JBI, Joanna Briggs institute critical appraisal checklist for RCTs; M-SIT, multimedia videos for mobile stress inoculation training; MBSR, mindfulness-based stress reduction; NR, no report; NA, no answer; PHQ, patient health questionnaire; PSS, perceived stress scale; CES-D, Center for Epidemiologic Studies Depression Scale; MSP, Mesure de Stress Psychologique; GHQ, General Health Questionnaire; STAI, State and Trait Anxiety Inventory.
Totally, seventy-six articles in the nine systematic reviews met the inclusion criteria of the study. These studies were conducted on a total of 3,581 participants (ranging from 8 to 855). However, thirty-two out of the seventy-six articles were repeated. On average, each systematic review contained four articles that met the aim of the current study. Most systematic reviews included young adult to adult populations (18–55 years old) (Reference Nair, Armfield, Chatfield and Edirippulige32;Reference Firth, Torous, Nicholas, Carney, Rosenbaum and Sarris33;Reference Lyzwinski, Caffery, Bambling and Edirippulige36;Reference Griffiths, Farrer and Christensen38). In addition, in one systematic review, the participants aged 18–65 years (Reference Stratton, Lampit, Choi, Calvo, Harvey and Glozier34).
In three systematic reviews, other disorders were studied in addition to depression, anxiety, and stress. Other disorders included psychotic disorders, sleep disorder, substance abuse (Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37), suicidal behavior (Reference Menon, Rajan and Sarkar35;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37), schizophrenia (Reference Rathbone and Prescott20;Reference Menon, Rajan and Sarkar35), bipolar disorders, eating disorders, gambling (Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37), smoking cessation, medication adherence, and mood depressive disorders (Reference Rathbone and Prescott20). Furthermore, other interventions were used in addition to mobile applications in six systematic reviews. These interventions included electronic-based (Reference Lyzwinski, Caffery, Bambling and Edirippulige36) and Internet-based interventions (Reference Griffiths, Farrer and Christensen38), SMS (Reference Rathbone and Prescott20), eHealth interventions (Reference Stratton, Lampit, Choi, Calvo, Harvey and Glozier34), mobile phone-based technologies (Reference Menon, Rajan and Sarkar35), and telemedicine (Reference Nair, Armfield, Chatfield and Edirippulige32). The duration of interventions varied from 1 week (Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37) to 1 year (Reference Griffiths, Farrer and Christensen38). Besides, the duration of interventions was more than 6 weeks in eight studies (Reference Rathbone and Prescott20;Reference Kerst, Zielasek and Gaebel31;Reference Nair, Armfield, Chatfield and Edirippulige32;Reference Stratton, Lampit, Choi, Calvo, Harvey and Glozier34–Reference Griffiths, Farrer and Christensen38).
We assessed systematic reviews in line with outcome variables. Our findings related to the comparison between outcome variables among included systematic reviews are summarized in Table 3. We tried to find a common measurement scale among included studies. The effect sizes were comparable finding between systematic reviews, although it was not reported in one study. In this regard, the largest effect size was found in Menon et al. (Reference Menon, Rajan and Sarkar35) and Kerst et al. (Reference Kerst, Zielasek and Gaebel31) studies. In both systematic reviews, all reviewed mobile apps interventions were effective in reducing intended symptoms. Moreover, the acceptability of these studies was good, which is an important factor for the successful implementation of an intervention in practice (Reference Ediriweera, Kasturiratne, Pathmeswaran, Gunawardena, Wijayawickrama and Jayamanne40). Hence, the smallest effect size was from Nair et al. study (Reference Nair, Armfield, Chatfield and Edirippulige32). This can be related to high attrition rates as well as a lack of participant blinding that were reported as common limitations.
Table 3. The comparison between outcome variables among included systematic reviews

d, effect size; P, p-value; NR, not reported.
Effects on Depression, Stress, and Anxiety
Five systematic reviews that measured depression outcomes using the Patient Health Questionnaire (PHQ-9) showed a reduction in the depression score (Reference Rathbone and Prescott20;Reference Kerst, Zielasek and Gaebel31;Reference Nair, Armfield, Chatfield and Edirippulige32;Reference Stratton, Lampit, Choi, Calvo, Harvey and Glozier34;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). Three systematic reviews that used Beck Depression Inventory (BDI) also revealed a reduction in the depression score (Reference Rathbone and Prescott20;Reference Kerst, Zielasek and Gaebel31;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). However, one study that used the “Center for Epidemiologic Studies Depression Scale” (CES-D) did not show any significant reduction in the depression score (Reference Griffiths, Farrer and Christensen38). Furthermore, three systematic reviews measured stress outcomes using the Perceived Stress Scale (PSS) and showed a significant reduction in the stress scores (Reference Rathbone and Prescott20;Reference Stratton, Lampit, Choi, Calvo, Harvey and Glozier34;Reference Lyzwinski, Caffery, Bambling and Edirippulige36). However, stress was measured by the Mesure de Stress Psychologique (MSP) scale in one study, which revealed no significant reduction (Reference Lyzwinski, Caffery, Bambling and Edirippulige36). In addition, three systematic reviews measured anxiety outcomes using Generalized Anxiety Disorder 7-item (GAD-7) (Reference Rathbone and Prescott20;Reference Firth, Torous, Nicholas, Carney, Rosenbaum and Sarris33;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). In one study, no significant reduction was found in the anxiety scores (Reference Rathbone and Prescott20). Furthermore, State and Trait Anxiety Inventory (STAI) was used in one systematic review, which indicated a significant reduction in the anxiety scores (Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). Besides, two systematic reviews used the Depression Anxiety Stress Scale (DASS) to measure depression, anxiety, and stress (Reference Rathbone and Prescott20;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). One study showed no significant reduction in the scores of depression, anxiety, and stress (Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). However, two systematic reviews used the General Health Questionnaire (GHQ) and obtained significant results (Reference Rathbone and Prescott20;Reference Lyzwinski, Caffery, Bambling and Edirippulige36).
Characteristics of Depression, Stress, and Anxiety Apps
In total, twenty-two apps with specific names were reported in the nine systematic reviews. The most commonly reviewed apps were Flowy, Get happy, myCompass, and Mood Gym. The applications that used behavior change strategies, such as Cognitive Behavioral Therapy (CBT), Acceptance and Commitment Therapy (ACT), Behavioral Activation (BA), mindfulness-based therapy, and stress inoculation therapy, reported significant effects on depression, anxiety, and stress (Reference Firth, Torous, Nicholas, Carney, Rosenbaum and Sarris33–Reference Griffiths, Farrer and Christensen38). However, no significant reduction was found in one study using CBT (Reference Griffiths, Farrer and Christensen38). myCompass was a self-monitoring app that used CBT, positive psychology, and problem-solving training strategies. Furthermore, it provided feedback and tips via SMS (Reference Firth, Torous, Nicholas, Carney, Rosenbaum and Sarris33). Another effective app was Get happy, which was based on the principles of ACT and provided personalized strategies relating to relationships, personal growth, leisure, and work education (Reference Rathbone and Prescott20). Mood Gym was yet another app that was proved to be effective in preventing and reducing depression and anxiety. It was a web-based app based on cognitive, behavioral, and interpersonal therapy, problem-solving, and coping strategies. Mood Gym provided weekly phone calls to users. It also provided quizzes, exercises with visual aids, and detailed feedback. The content of the Mood Gym included thoughts, moods, and ways to change them (Reference Griffiths, Farrer and Christensen38).
Satisfaction, Adherence, and Acceptability
Two systematic reviews revealed the users’ high satisfaction with smartphone apps (Reference Kerst, Zielasek and Gaebel31;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). Additionally, three systematic reviews showed high adherence to the intervention (Smartphone application intervention) (Reference Rathbone and Prescott20;Reference Kerst, Zielasek and Gaebel31;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). However, one study showed low adherence to the intervention (mobile and web-based apps interventions) (Reference Lyzwinski, Caffery, Bambling and Edirippulige36). Furthermore, five systematic reviews reported the high acceptability of smartphone applications among users (Reference Kerst, Zielasek and Gaebel31;Reference Firth, Torous, Nicholas, Carney, Rosenbaum and Sarris33;Reference Menon, Rajan and Sarkar35;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). The users were more satisfied with the apps that used behavior change strategies (Reference Kerst, Zielasek and Gaebel31;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37).
The Methodological Shortcomings of the Included Studies
We categorized the main methodological shortcomings of the included studies in Supplementary File 3. Accordingly, the main limitation was heterogeneity in the aims, methodology, or outcome measures of the studies that made it hard to draw a clear conclusion (Reference Rathbone and Prescott20;Reference Kerst, Zielasek and Gaebel31–Reference Firth, Torous, Nicholas, Carney, Rosenbaum and Sarris33;Reference Menon, Rajan and Sarkar35;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). Also, another limitation was missing studies because of including just English-language, peer-reviewed articles, or searching in specific (narrow) databases (Reference Rathbone and Prescott20;Reference Kerst, Zielasek and Gaebel31;Reference Menon, Rajan and Sarkar35–Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). Moreover, subjective assessment, which means self-reported measurement instead of a clinical diagnosis, was also reported (Reference Nair, Armfield, Chatfield and Edirippulige32;Reference Stratton, Lampit, Choi, Calvo, Harvey and Glozier34).
Discussion
App-based interventions caused a reduction in depression, anxiety, and stress symptoms in almost all reviewed studies. These results were promising and in line with those of the previous studies (Reference Harrer, Adam, Fleischmann, Baumeister, Auerbach and Bruffaerts41–Reference Børøsund, Varsi, Clark, Ehlers, Andrykowski and Sleveland43). The results suggested that mobile apps had the potential to be effective in improving the symptoms of depression, anxiety, and stress. Given the increasing popularity of smartphones, mHealth has the potential to be effective in mental healthcare delivery, especially in low- and middle-income countries and hard-to-reach populations (Reference Wang, Varma and Prosperi44).
The present study findings showed that the duration of interventions was more than 6 weeks in eight systematic reviews. So, it can be noted that for behavior change to happen, the duration of mobile app interventions should be more than a month. This result was in agreement with those of other studies, indicating that longer durations of interventions or follow-ups were necessary to evaluate the effectiveness of mobile apps (Reference Man-Son-Hing, Laupacis, O'Rourke, Molnar, Mahon and Chan45–Reference Zhao, Freeman and Li47). Additionally, our overview showed that the use of reminders was an important factor to increase the acceptability of a mobile app intervention. Several studies have proved the effectiveness of electronic reminders in improving adherence to treatment and medication (Reference Vervloet, Linn, van Weert, De Bakker, Bouvy and Van Dijk48–Reference Berrouiguet, Baca-García, Brandt, Walter and Courtet50).
The results of this systematic review recommended the interventions, such as CBT, ACT, BA, mindfulness-based therapy, and stress inoculation therapy, which were based on behavior change strategies for the reduction of depression, anxiety, and stress. Some studies also reported the effectiveness of behavior change strategies in the field of mental health (Reference Brenninkmeijer, Lagerveld, Blonk, Schaufeli and Wijngaards-de Meij51–Reference Soleimani, Mohammadkhani, Dolatshahi, Alizadeh, Overmann and Coolidge54).
The findings of the present systematic review indicated that the target groups of most apps were young adults and adults, which might be due to the prevalence of psychiatric disorders among these age groups (Reference Mirzaei, Ardekani, Mirzaei and Dehghani55). Teenagers had received the least attention and were studied in just one systematic review. Because teenage is a transitional period, more attention should be given to this age group. During this period, teenagers experience a variety of biological, cognitive, and social changes and encounter a great amount of emotional distress, which can lead to complications (Reference Hashmi56). Another age group that has been ignored is the senior citizen group. According to the World Health Organization (WHO), the world population is aging quickly. Between 2015 and 2050, the percentage of the world's population aged over 60 years has been estimated to almost double from 12 to 22 percent. Approximately 15% of adults aged 60 years and over suffer from a mental disorder. Mental health and well-being are as important in older age as at any other time during life (57). Hence, future research is recommended to focus more on these two age groups.
Several studies have demonstrated that physician support through phone calls, SMS, or e-mails could improve the outcomes (Reference Kerst, Zielasek and Gaebel31;Reference Nair, Armfield, Chatfield and Edirippulige32). This result was consistent with those obtained by Mohr et al. (Reference Mohr, Tomasino, Lattie, Palac, Kwasny and Weingardt58) and Cuijpers et al. (Reference Cuijpers, Kleiboer, Karyotaki and Riper59), which indicated that clinician support was an influential factor in improving the patients’ adherence to interventions. Therefore, physician support has been recommended to be included as a part of the interventions to achieve higher efficiency.
The findings of the current overview confirmed those of the previous studies, which showed that the effect of interventions might be lower in active controls (receiving an intervention) compared with those in the waiting list (receiving no interventions) (Reference Firth, Torous, Nicholas, Carney, Pratap and Rosenbaum60). The use of an active control group could improve the outcome for controlling the condition. This finding could be explained by the Hawthorne effect; the subjects of a study changed their behavior due to their awareness of being observed (Reference McCambridge, Witton and Elbourne61). Accordingly, using the app itself improved the outcome for users. Hence, using an active control group is recommended in order to determine whether the improvement is due to the use of the app alone or due to the app content.
The included systematic reviews were conducted on different populations. In addition, some reviews had focused on specific populations, such as pregnant women and mothers up to 12 months postpartum (Reference Nair, Armfield, Chatfield and Edirippulige32), current paid employment and working-age adults (Reference Stratton, Lampit, Choi, Calvo, Harvey and Glozier34), healthy adults (Reference Lyzwinski, Caffery, Bambling and Edirippulige36), and people with mental health symptoms or disorders (Reference Kerst, Zielasek and Gaebel31;Reference Menon, Rajan and Sarkar35;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37;Reference Griffiths, Farrer and Christensen38). On the other hand, some other studies were not focused on a specific population and reviewed general and clinical populations (Reference Rathbone and Prescott20;Reference Firth, Torous, Nicholas, Carney, Rosenbaum and Sarris33). In this regard, the results of a study showed that designing interventions for healthcare students or providers reduced stress and depression (Reference Pospos, Young, Downs, Iglewicz, Depp and Chen62). Besides, mobile phone-based apps designed for psychotic populations were effective in reducing the symptoms of stress, anxiety, or depression (Reference Menon, Rajan and Sarkar35). Nonetheless, other studies with wider populations showed different results. Some of them showed effective results (Reference Rathbone and Prescott20;Reference Kerst, Zielasek and Gaebel31;Reference Griffiths, Farrer and Christensen38), whereas some others revealed both effective and ineffective findings (Reference Lyzwinski, Caffery, Bambling and Edirippulige36;Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). Thus, it could be concluded that the interventions that were designed for specific populations were more effective. However, in the case of large populations, it might be difficult to meet the needs of different users, and it might impact on effectiveness. The results also indicated that the two systematic reviews that showed more positive results had longer follow-up periods (Reference Rathbone and Prescott20;Reference Griffiths, Farrer and Christensen38). Therefore, longer interventions are likely to have more effective results. It can also be concluded that applications are more effective in long-term use.
Mental health apps can provide remote therapy sessions for those people who do not obtain treatment due to geographic, social, or health (physical disability and stigmatization concerns) barriers. This gives them a chance to being treated in geographically desired places, as well as saving their time and monetary cost of traveling (Reference Price, Yuen, Goetter, Herbert, Forman and Acierno63). In addition, the mental health app can provide portable and flexible professional help for people in need of treatment in a timely and anonymous manner. Moreover, it can be effective for people who are not seeking treatment (Reference Ebert, Van Daele, Nordgreen, Karekla, Compare and Zarbo64), whereas nonvalidated apps can have negative impacts on patients (Reference Weisel, Fuhrmann, Berking, Baumeister, Cuijpers and Ebert65). Unfortunately, only a few research studies have systematically evaluated the efficacy of mental health app. A systematic review study in 2016 found only five mental health-related apps, out of which only three were examined in an RCT (Reference Donker, Petrie, Proudfoot, Clarke, Birch and Christensen37). In addition, a study that searched app markets for mental health-related application found 208 apps, but the effectiveness of the majority of them was not validated by scientific research (Reference Radovic, Vona, Santostefano, Ciaravino, Miller and Stein66). Moreover, another study conducted in 2019 revealed that although there are hundreds of mental health apps in the app markets, just nineteen eligible studies were found that evaluated the efficacy of apps in an RCT research (Reference Weisel, Fuhrmann, Berking, Baumeister, Cuijpers and Ebert65).
Although app markets have surged enormously, selecting a reliable and effective app is another issue (Reference Kerst, Zielasek and Gaebel31). A study showed that only 14 out of 100 mental health applications benefitted from clinically validated evidence (Reference Wang, Varma and Prosperi44). Nonvalidated mental health mobile apps could be harmful to users (Reference Salehi, Kermani, Khademian and Aslani67). Keeping this in mind, a validated mobile phone-based application should become available to assist the community. Moreover, according to a study, the eHealth literacy of most young people in Iran was reported to be at a low level. Therefore, necessary measures should be taken to improve people's eHealth literacy when using health app (Reference Dashti, Peyman, Tajfard and Esmaeeli68). In conclusion, the present study findings revealed that mobile apps had the potential to be effective in improving the symptoms of depression, anxiety, and stress. Therefore, the results supported the development of mental health apps as a valuable intervention.
Limitation
The current study had several limitations. First, the included studies were of varied qualities. Second, in spite of a systematic search of five databases, the possibility of missing some articles cannot be ignored. Third, despite the promising findings, it should be noted that the evidence is still limited, and the results should be interpreted with due caution. Overall, this is an emerging area of research, and further exploration should be done in future in order to reach conclusive evidence.
Conclusion
The current systematic review aimed to summarize the evidence on the effectiveness of mobile-based applications in monitoring stress, anxiety, and depression symptoms. To the best of our knowledge, this is the first overview of the systematic reviews examining the effects of mobile app interventions on stress, anxiety, and depression symptoms. The study findings might be of use for mental health app users, researchers, and healthcare providers. They can also be helpful for the future development of new mobile apps targeting mental health. It seems that mental health apps can be promising media to reduce depressive symptoms.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0266462320002093.
Acknowledgment
The authors wish to thank Mr. F. Fatehi for his invaluable assistance for improving the use of English in the manuscript.
Funding
This article was extracted from a project approved by Shiraz University of Medical Sciences, Shiraz, Iran (No. 98-01-68-19603).
Declaration of Competing Interest
The authors have no competing interests.






