Unroofed coronary sinus syndrome is a rare congenital cardiac anomaly in which the roof of the coronary sinus is absent, resulting in a partial or complete defect between the coronary sinus and the left atrium.Reference Kong and Ahmad1
In coronary sinus orifice atresia, myocardial ischaemia, infarction, and death have been reported in several patients in whom there was no alternative exit for the coronary sinus blood.Reference Yokota, Kyoku and Kitano2
We report a rare combination of partial unroofed coronary sinus and coronary sinus orifice atresia in an infant.
Case report
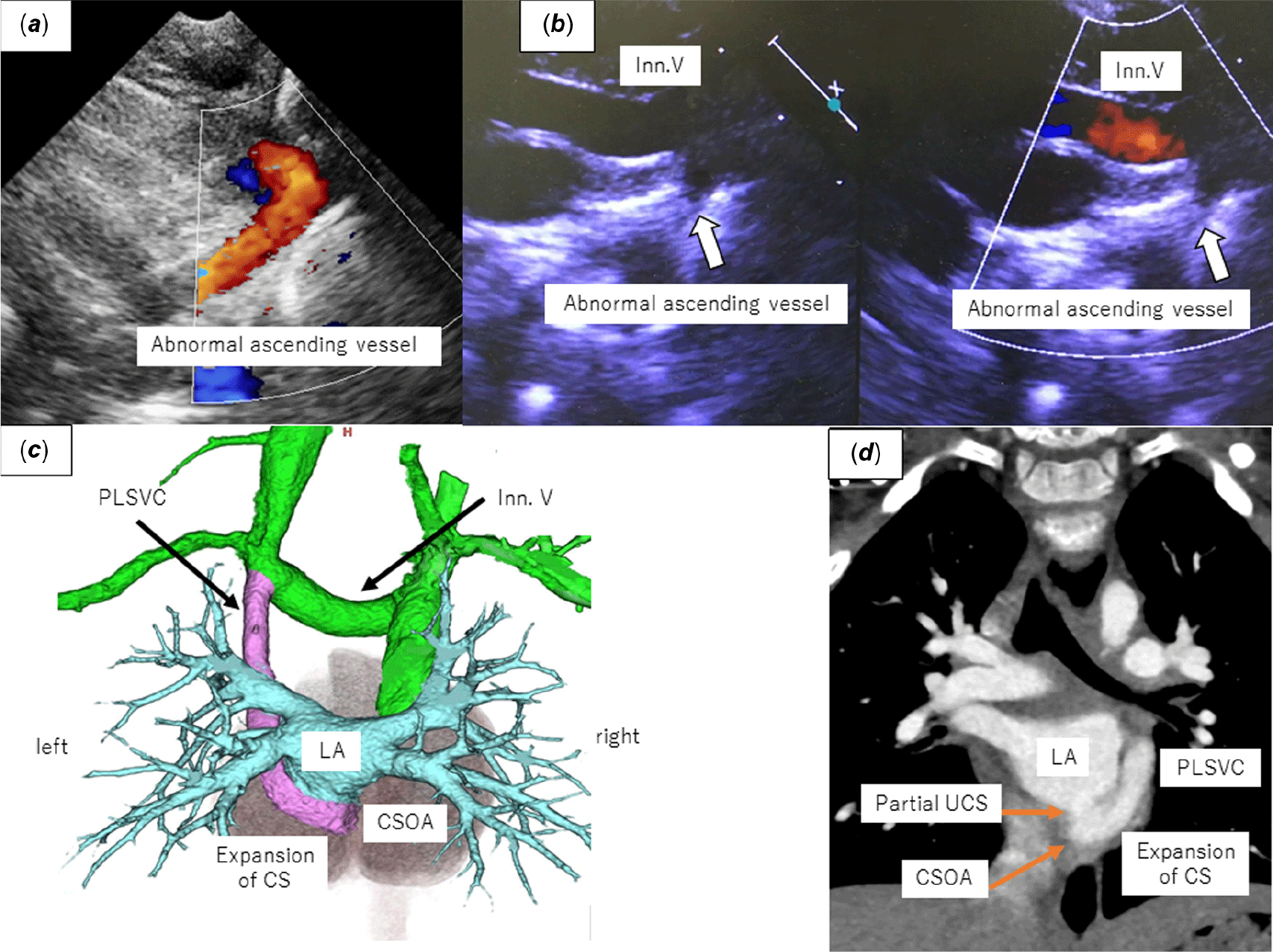
Our patient was a 1-year and 8-month-old boy weighing 9 kg. He was born, weighing 2294 g, by normal spontaneous vaginal delivery at 37 weeks’ gestation. Cardiac murmur was detected at the age of 5 days. Echocardiography revealed a patent ductus arteriosus, a patent foramen ovale, and an anomalous ascending vessel draining into the innominate vein (Fig 1a and b). Initially, this abnormal vessel was considered as the partial anomalous pulmonary vein. He had no clinical symptoms and was followed up without any medication. Patent ductus arteriosus and patent foramen ovale closed spontaneously at the age of 3 months, but this abnormal vessel showed no change. He was referred to our department for haemodynamic evaluation. Enhanced cardiac CT revealed an abnormal vessel as persistent left superior caval vein connecting between the coronary sinus and the innominate vein (Fig 1c). However, the end of coronary sinus draining to the right atrium was not recognised, and the partial unroofed coronary sinus was identified (Fig 1d). No other congenital abnormality was identified. Cardiac catheter examination was performed to elucidate the haemodynamics. A Berman wedge catheter was easily advanced from the persistent left superior caval vein through the unroofed coronary sinus into the left atrium (Fig 2a). The pressure in the left atrium was 8 mmHg, and that in the persistent left superior caval vein and the innominate vein was 8 and 6 mmHg, respectively. The pulmonary/systemic flow ratio was 1:1. Persistent left superior caval vein angiography revealed the contrast ascending into the innominate vein, draining into the superior caval vein (Fig 2b). On the other hand, the contrast flowed in the reverse direction through the unroofed coronary sinus into the left atrium during balloon occlusion with no ischaemic changes on electrocardiography (Fig 2c). The pressure in the persistent left superior caval vein increased from 8 to 9 mmHg during balloon occlusion. The pressure in the innominate vein was unchanged. This patient has been followed up with no intervention and he has been asymptomatic.

Figure 1. Echocardiogram and enhanced cardiac CT. (a) Red colour shows an ascending vessel with continuous flow. (b) This abnormal vessel drains into Inn.V. (c) Three-dimensional image from posterior view; all four pulmonary veins drain into LA. PLSCV connects between CS and Inn.V. (d) Coronal view shows CSOA and partial UCS. CSOA = coronary sinus orifice atresia; Inn.V = innominate vein; LA = left atrium; PLSCV = persistent left superior caval vein; UCS = unroofed coronary sinus.

Figure 2. Catheter examination. (a) Berman wedge catheter advances into LA from PLSCV through UCS easily. (b) PLSCV angiogram without balloon occlusion; contrast ascends to Inn.V draining into SCV smoothly. (c) PLSCV angiogram with balloon occlusion; contrast descends into LA through UCS smoothly. (d) Schematic image of this patient. CSOA = coronary sinus orifice atresia; ICV = inferior caval vein; Inn.V = innominate vein; LA = left atrium; PLSCV = persistent left superior caval vein; RA = right atrium; SCV = superior caval vein; UCS = unroofed coronary sinus.
Discussion
We describe a rare case of a combination of partial unroofed coronary sinus and coronary sinus orifice atresia having persistent left superior caval vein with bidirectional coronary venous return.
Unroofed coronary sinus is defined by the presence of communication in the wall between the coronary sinus and the left atrium.Reference Ootaki, Yamaguchi, Yoshimura, Oka, Yoshida and Hasegawa3 Patients with this anomaly exhibit signs and symptoms identical to those with atrial septal defect. However, our patient’s pulmonary/systemic flow ratio was just 1:1. Therefore, we considered he had no heart failure symptoms. Generally, intra-cardiac shunt flow in this anomaly is expected to be in the left-to-right direction; however, right-to-left shunt can happen depending on the communication size and the inter-atrial pressure gradient.Reference Shirakawa, Kawamura and Muraoka4 Consequently, early diagnosis and treatment of this anomaly have diagnostic importance because right-to-left shunt can result in cerebral embolism or brain abscess.Reference Ootaki, Yamaguchi, Yoshimura, Oka, Yoshida and Hasegawa3 In this case, the contrast flowed right-to-left direction during balloon occlusion with the slight pressure increase of the persistent left superior caval vein. This result showed that he had the risk of paradoxical embolisation.
In coronary sinus orifice atresia, myocardial ischaemia is unlikely as long as an alternate exit exists for coronary sinus blood,Reference Santoscoy, Walters, Ross, Lyons and Hakimi5 namely, via two possible circulatory routes as follows: First, the coronary sinus blood flows into the left atrium through an unroofed coronary sinus. Second, the coronary sinus blood flows across the persistent left superior caval vein into the innominate vein, back towards the right atrium. Our patient had both alternate exists, and coronary venous flow was bidirectional depending on the slight pressure balance between the left atrium and the persistent left superior caval vein. The only clue for diagnosis is the reverse direction of flow through persistent left superior caval vein.Reference Song, Ren and Chen6 We believe that the catheter examination is the good modality to elucidate the haemodynamics in this anomaly.
Persistent left superior caval vein ligation was discussed to decrease the pulmonary/systemic flow ratio. When the pressure of the persistent left superior caval vein is <16 mmHg in unroofed coronary sinus, the persistent left superior caval vein can be ligated.Reference Ootaki, Yamaguchi, Yoshimura, Oka, Yoshida and Hasegawa3 The pressure in the persistent left superior caval vein stayed at 9 mmHg during test occlusion. However, the occlusion time was short, and although the haemodynamics was not completely the same, Yokota et al reported the inadvertent ligation of left superior caval vein leading to death in a patient with transposition of great arteries with coronary sinus ostial atresia.Reference Yokota, Kyoku and Kitano2 Furthermore, coronary venous flow returned to the left atrium through the unroofed coronary sinus during balloon occlusion, which is like a single ventricle physiology.Reference Kaneko, Kobayashi, Yamamoto and Tsuchiya7 This circulation has the risk of cyanosis and paradoxical embolism. Although ischaemic change or cyanosis did not occur during test occlusion in our patient, we decided not to perform the persistent left superior caval vein ligation.
In summary, we experienced a rare case of partial unroofed coronary sinus complicated by coronary sinus orifice atresia with persistent left superior caval vein in an infant. This patient had bidirectional coronary venous flow. The flow changed by the slight pressure balance between the left atrium and the persistent left superior caval vein. We need to reconsider the intervention if heart failure symptoms appear due to left-to-right shunt or paradoxical embolism occurs due to right-to-left shunt. We believe that the closure of unroofed coronary sinus and creation of the coronary sinus are the appropriate intervention to correct the haemodynamics.
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.