


INTRODUCTION
Early identification of delirium in children is an urgent medical matter, as recognition and treatment of its underlying causes may minimize long-term consequences. Although pediatric delirium (PD) research has lagged behind adult studies, it has been established that delirium in children is a significant problem, with acute and potentially long-term effects (Colville et al., Reference Colville, Kerry and Pierce2008; Schieveld et al., Reference Schieveld, van Tuijl and Pikhard2013; Schieveld et al., Reference Schieveld, Leroy and van Os2007; Smith et al., Reference Smith, Fuchs and Pandharipande2009; Reference Smith, Brink and Fuchs2013), and presents similarly as in adults (Leentjens et al., Reference Leentjens, Schieveld and Leonard2008; Turkel et al., Reference Turkel, Trzepacz and Tavaré2006). As delirium is a clinical diagnosis, it is extremely important to standardize assessment and develop clinical screening tools for detection of delirium in critically ill patients of all ages (Girard & Ely, Reference Girard and Ely2008; Schmitt et al., Reference Schmitt, Marcantonio and Alsop2012).
Even with recent progress, there is still a lack of consensus around the diagnosis of delirium in very young or developmentally delayed children, as this requires a developmentally informed assessment. Mastering developmental assessment of the healthy child is a core pediatric skill, yet the pediatric and child psychiatry literature is scant on assessment of development or cognition in ill children. It is generally taught that children temporarily regress behaviorally and emotionally during illness. A child's newly acquired, and therefore precariously anchored, developmental achievements may be temporarily lost. Assessment must take into account such potential fluctuations in milestones and changes in attachment behavior due to the stress of illness and hospitalization (Smith et al., Reference Smith, Boyd and Fuchs2011). Complicating assessment further is the presence of pain, fatigue, anxiety, and sedation in a hospitalized or ill child (see Table 1).
Table 1. Behavioral changes in illness

Adapted from Table 84.1, “Distress Signs,” in Lewis (Reference Lewis and Lewis1991).
Observational and retrospective studies of referred populations have included small numbers of cases of infants and developmentally delayed children (Janssen et al., Reference Janssen, Tan and Staal2011; Schieveld et al., Reference Schieveld, Leroy and van Os2007; Turkel et al., Reference Turkel, Braslow and Tavaré2003), likely because of under-recognition of delirium and under-referral in these populations. In a four-year observational study of patients referred to psychiatry, Schieveld and colleagues reported a 3% rate of delirium in children aged 0–3 years (Leentjens et al., Reference Leentjens, Schieveld and Leonard2008; Schieveld et al., Reference Schieveld, Leroy and van Os2007). The pediatric confusion assessment method for the ICU (pCAM–ICU) has been validated for children aged 5 years and older, but children with developmental or psychiatric comorbidities were excluded (Smith et al., Reference Smith, Boyd and Fuchs2011). Nevertheless, concern about delirium in children aged 0–5 years has led to the development of a preschool version (psCAM–ICU) (validation currently in progress), and the Pediatric Anesthesia Emergence Delirium (PAED) scale has been validated for children aged 12 months and older (Sikich & Lerman, Reference Sikich and Lerman2004; Janssen et al., Reference Janssen, Tan and Staal2011).
The Cornell Assessment for Pediatric Delirium
The Cornell Assessment for Pediatric Delirium (CAPD) was developed to be a rapidly and easily administered screening tool for nurses to identify critically ill children of all ages and developmental stages who are at risk for delirium (see Figure 1). It was piloted and validated against the gold standard: an evaluation based on the Diagnostic and Statistical Manual (DSM) by child psychiatrists in two previously published studies (Silver et al., Reference Silver, Traube and Kearney2012; Traube et al., Reference Traube, Silver and Kearney2013). It was adapted from the PAED scale, which is an observational scale requiring no patient participation. The PAED tends to select for hyperactive delirium, likely due to its intended use in children emerging from anesthesia. Prior efforts to adapt the PAED for the pediatric intensive care unit (PICU) setting showed its suitability and feasibility as an observational scale, but also noted its limitations with respect to detection of hypoactive delirium and a lack of identification of cognitive changes (Blankespoor et al., Reference Blankespoor, Janssen and Wolters2012; Janssen et al., Reference Janssen, Tan and Staal2011). The CAPD scale was designed to address these needs. It consists of eight items that correlate with the diagnostic domains of awareness and cognition from the DSM-5, and also includes psychomotor symptoms. In extensive testing, it has proved to be highly feasible to administer by bedside nurses and takes less than two minutes per patient. Because it is based on behavioral observations of the patient during routine nursing care, it also does not require patient participation at time of administration, making it universally well tolerated.

Fig. 1. Cornell Assessment of Pediatric Delirium (CAPD) revised.
Improving Reliability
Reliability of a diagnosis of pediatric delirium in young children depends on (1) the ability of the examiner to identify age-appropriate and developmental stage–expected behaviors; (2) the ability of the rater to assess whether deviations from expected behaviors are (a) a consequence of developmental delay (an atypical baseline), (b) a change from baseline as a consequence of regression associated with illness, or (c) a change from baseline due to delirium (Silver et al., Reference Silver, Kearney and Traube2014); (3) the ability of the examiner to explore and understand how a child may experience and express pain, and how this may be expressed at different developmental stages; and (4) the ability of the examiner to elicit concerns and ideas that may be associated with anxiety, and how to understand this in children in a developmental context.
The physician examiners on the research team addressed these issues of accuracy and reliability of assessment through frequent interdisciplinary meetings to discuss difficult cases, where delirium was on the differential diagnosis but not clearly manifest. Anecdotally, the consistency of psychiatrists' diagnostic approaches improved and in an early phase of the study showed good interrater reliability (Silver et al., Reference Silver, Kearney and Traube2014). “Thinking developmentally” about each diagnostic symptom domain allowed the clinician to differentiate the delirious child from a child experiencing pain, anxiety, or regression (Schieveld et al., Reference Schieveld, van der Valk and Smeets2009; Smith et al., Reference Smith, Brink and Fuchs2013).
In the early phases of CAPD development, reliability between nurse screeners varied, and it became clear that ratings differed based on nurses' comfort and understanding of child development and behavior, particularly for preverbal children. With minimal psychoeducation (little more than reminding nurses about their knowledge and clinical experience assessing developmental stages in children), interrater reliability improved. For example, item #1—“Does the child make eye contact with the caregiver?”—evaluates a behavior that indicates awareness, and delirious children are frequently observed to have an unfocused and wandering gaze. Nurses questioned how to evaluate “eye contact” in an infant or young child. It was stressed to “think developmentally,” to compare current assessment with the developmentally expected level. One can expect an 8 week old to look at the examiner, to follow objects past midline, or to regard their own hand (Ball, Reference Ball1977; Shapiro & Hertzig Reference Shapiro, Hertzig, Talbot and Hales2003). If the child's gaze is floating around the room, never focused, this is considered altered eye contact, and the nurse would report how frequently that alteration was noted. These discussions demonstrated that a standardized assessment for delirium in young children needed to be explicitly anchored in a framework of developmental milestones. Similar observations were also recently noted by Turkel and colleagues in regard to psychiatric diagnosis of delirium in infants (Turkel et al., Reference Turkel, Jacobson and Tavaré2013).
METHODS
Creation of CAPD Developmental Anchor Points
The “developmental anchor points” (previously unpublished) were initially taken from developmental texts and established scales for the behavioral domains addressed by CAPD items (Ball, Reference Ball1977; Bayley, Reference Bayley2005; Frankenburg et al., Reference Frankenburg, Dodds and Archer1990). These were then reviewed by a panel of experts that included experienced child psychiatrists (from psychoanalytic, infant, and consult–liaison psychiatry subspecialties), pediatric intensivists, pediatric nurses, developmental psychologists, and a psychometrician in order to evaluate for content validity and include consideration of sick behaviors in a hospital setting. For example, an early version of the developmental anchor points for item #2—“Are the child's actions purposeful?”—included motor milestones for a 2 year old such as “jumps, kicks a ball, builds a tower of seven blocks.” Considering the constraints of the hospital and the fatigue and malaise of a sick 2 year old, this was changed to “Tries to change position; if mobile tries to get up and walk.” Building towers would require blocks and the child's willing participation, so it was eliminated. For item #6—“Does the child communicate needs and wants?”—the 2-year-old guideline originally stated, “50+ words, uses I and you, 3–4 word sentences, uses plurals.” Taking into account that the child may be intubated, or regressed, not feeling well, weak or uncomfortable, it was changed to “uses 3–4 word sentences or signs to communicate needs.” These changes were intended to capture the normal developmental expectations in the context of an ill, hospitalized child.
RESULTS
The resulting developmental anchor points at the key ages of newborn (NB), 4 weeks, 6 weeks, 8 weeks, 28 weeks, 1 year, and 2 years (Figure 2) served as the basis for the training of nurses to score the CAPD in the validation trial (Traube et al., Reference Traube, Silver and Kearney2013). The developmental anchor points also served as a multifaceted bedside reference chart for the two blinded nurses when scoring the initial 70 CAPD screens. As previously reported, reliability was excellent, with kappa ranging from 0.68 to 0.78 for each individual item and a kappa of 0.94 for the overall screen result (positive score >9).
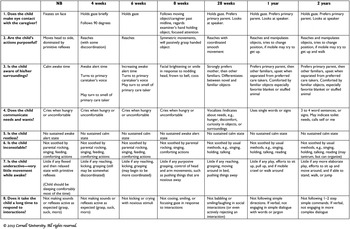
Fig. 2. CAPD developmental anchor points for youngest patients.
DISCUSSION
Considering Each Child's Developmental Trajectory
Developmental milestone charts are useful for education and screening. However, each child is a “moving target” on his or her own trajectory, which can occur at various normal paces, with normal temporary plateaus. Furthermore, differential development of particular domains (e.g., gross motor, social, language) is normal and expected. While the presence of delays should be noted in a child's medical record, it is common for these comorbidities to be minimized or glossed over in the discussion of complex critical illness. In the PICU setting, if parents are absent, the child's pre-hospitalization baseline eye-contact or language abilities are often unknown. In psychiatric assessment, determination of baseline is usually a first step, along with questioning of the parent or caregiver (e.g., “Is this his/her normal self?” or, per Schieveld, “Is this still your child?”) (Creten et al., Reference Creten, van der Zwaan and Blankespoor2011).
Input from staff and bedside caregivers (aides and companions) can help in reaching a consensus as to whether there is a change from baseline. It is helpful to ask about temperament, regulation (baseline sleep and feeding behaviors), recent developmental milestones, previous hospitalizations, favorite comforts and interests, and baseline relationships with caregivers, in order to inform assessment of the other diagnostic domains.
In the hands of the primary bedside nurse, the CAPD can reliably account for individual variations in development. The experience of pediatric nurses with ill children of all ages is invaluable. Their bond with and knowledge of a particular child's family members and caregiving style, particularly in units that employ a primary nursing model, helps establish the child's baseline both pre- and in-hospital.
The CAPD is designed to be utilized by a nurse who has been caring for a patient, completing the scale mid to late shift, reflecting the nurse's experience of the child for that day. It was designed as such to account for (1) a lack of baseline information if the parent was not available at the time of screening, often a limitation and obstacle for accurate assessment of mental status and behaviors in children, and (2) fluctuating mental status over the shift, a hallmark of delirium. Designed as an observational tool, the CAPD benefits from the patient–caregiver interaction (Smith et al., Reference Smith, Brink and Fuchs2013), as the bedside nurse is usually the person with the most cumulative knowledge and experience of the patient on that day. This can be contrasted to the PAED, which was developed for use by an anesthesia nurse accompanying a waking patient postanesthesia. As such, the CAPD, when implemented as recommended, is not a cognitive “test” the patient must pass, like the pCAM–ICU, nor is it a “snapshot” of behavior at a single point in time, like the PAED. Rather, it is an assessment by a trained observer with cumulative experience of the patient over time and across many interactions.
The CAPD, along with the developmental anchor points, was validated in both typically developing children and developmentally delayed children. Sensitivity in developmentally delayed children remained high (96.2%). Specificity was decreased (51.2%) from the overall cohort (79.2%), which was still acceptable for a screening tool (Mehler et al., Reference Mehler, Bertoncini and Barrière1978). Further research is needed to determine how to improve the specificity of this tool in this group. For immediate clinical implementation in the PICU setting, however, this should not be a barrier to utilization of the CAPD. A positive screen should result in referral to psychiatry, as is appropriate in this at-risk population. The psychiatrist can then further investigate the child's developmental baseline, assess the current mental status, and support the PICU team in the holistic care of a developmentally delayed, critically ill child.
Infant Consciousness and Cognition
The CAPD, with the associated developmental anchor points, was designed to assess an infant's mental status using observable behaviors in a PICU setting. The most challenging aspects of assessment of infants and young children are the domains of consciousness (also awareness, in the DSM-5) and cognition.
Normal consciousness may be described as having appropriate alertness, eye contact, awareness of surroundings, communication, and orientation (Ball, Reference Ball1977; Shapiro & Hertzig, Reference Shapiro, Hertzig, Talbot and Hales2003):
-
• Normal alertness in a newborn includes a significant part of the day spent sleeping, with some periods of crying, and periods of calm wakefulness (Holditch-Davis, Reference Holditch-Davis2005; Mirmiran et al., Reference Mirmiran, Maas and Ariagno2003). A hypoalert infant would not wake to feed, or when disturbed, or in pain. Such infants may lack a crying response when bedside procedures like venipuncture or arterial puncture are done. A hyperalert infant may be too distracted to feed and unable to settle into sleep even when fatigued.
-
• Appropriate eye contact develops from a newborn's soft focus on a caregiver's face, to holding a gaze at 6 weeks, to following an object across midline at 8 weeks, to holding a gaze and preferring to watch a parent at 28 weeks.
-
• Awareness of surroundings begins in newborns as having calm, awake time; by 4 weeks turning to the primary caregiver's voice or smell; and by 8 weeks frowning or turning to a bell, and demonstrating a social smile.
-
• Normal infant communication of needs and wants includes crying when hungry or uncomfortable. At 28 weeks, infants begin to vocalize and point. At 1 year of age, a child may use single words that indicate his awareness of himself and his needs.
-
• Normal orientation in an infant develops with increasing daytime wakefulness and nighttime sleep. Even a newborn will respond preferentially to mother or father's face and voices, and will be soothed by their voices and touch. This will generalize to the increasing soothability of a familiar song, rocking, or holding, and then a preference for primary caretakers over others. In the later months of the first year of life, an infant will clearly indicate an awareness of their own name/nickname (Newman et al., Reference Newman, Morini and Chatterjee2013).
Normal cognition involves the developmentally appropriate ability to learn, remember, and apply knowledge. Elements of cognition include: attention, memory, the production and understanding of language, reasoning, problem solving, and decision making. A cognitively intact infant is one whose actions are purposeful, whose distress is consolable when needs are met, and who utilizes verbal and nonverbal communication to express and manipulate her environment:
-
• Attention can be assessed by evaluating an infant's ability to hold a gaze with a caretaker or focus on a novel object. An 8-week-old infant who cannot hold the gaze of its caretaker or focus on a novel object will not be able to respond appropriately to that person or object (Bushneil et al., Reference Bushneil, Sai and Mullin1989; Field et al., Reference Field, Cohen and Garcia1984; Mehler et al., Reference Mehler, Bertoncini and Barrière1978; Newman et al., Chatterjee, Reference Newman, Morini and Chatterjee2013; Pascalis et al., Reference Pascalis, de Schonen and Morton1995).
-
• Memory can be assessed by recognition of caregivers and responses to familiar objects, routines, or comforts. At birth, infants recognize a caregiver's voice; with early development the infant will remember routines. They will repeat such learned efforts as kicking a mobile or ringing a bell (Gulya et al., Reference Gulya, Rovee-Collier and Galluccio1998).
-
• Psychomotor activity can affect or disrupt multiple areas of cognition. An infant or child with hyperactive delirium may be moving in a badly coordinated fashion, or so constantly that no purpose can be gleaned from her actions. A hypoactive infant may be so delayed and slow in hypoactivity that minimal or no benefit can be gained from his actions.
-
• Even a newborn infant can effectively communicate needs, and her awareness of them, by crying when hungry, or in pain, and stopping crying when fed or soothed. An older child of 1 or 2 years may symbolize nonverbally, or verbally, that she is hungry or uncomfortable, and then be able to symbolize relief or satisfaction. Even an intubated 2-year-old child will be able to point to his stomach in order to communicate pain.
-
• Perceptual disturbances are usually noted by caregiver observations of a child commenting on, or interacting with, something that is not real, for instance, a 5 year old who is swatting nonexistent flies.
Further Questions
Further research is needed to improve our understanding of delirium presentation in the developmentally delayed child. One possible solution to further “anchor” the CAPD for each child's developmental trajectory is a basic developmental screen, done on admission, designed to assess the baseline developmental domains most meaningful in delirium. As thoughtfully suggested by Schieveld and colleagues (Reference Schieveld, Janssen and Cauteren2014), it is possible that an initial CAPD, where parents/caregivers answer questions according to the child's behaviors prior to the current illness, can establish the baseline, but this needs to be validated in delayed children. Additionally, closer examination of subpopulations of developmentally atypical hospitalized children, such as formerly premature infants, may help identify particular risk factors for delirium. Future studies may be useful in determining whether increased frequency (more than twice per day) of screening will improve detection in cases of fluctuating mental status and possibly assist in tracking of delirium response to treatment or changing illness factors.
SUMMARY
Diagnosing delirium in children, particularly infants and children with developmental delay, can be challenging. However, “thinking developmentally” makes it possible to reliably and accurately interpret alterations in behavior, communication, and emotion in the critically ill child of any age. The developmental anchor points, added during piloting of the CAPD, embeds this developmental framework into the tool. As the core diagnostic features of delirium are thought to be the same at all ages, it is reasonable and practical to use an observational scale like the CAPD for all ages and developmental stages. The differential presentation of these symptoms in children of different ages and developmental stages is accounted for with the developmental anchor points reference tables, making the CAPD a valid and versatile tool for delirium screening for all children hospitalized in the PICU. Furthermore, implementation of the CAPD can be an opportunity for training pediatric providers of all disciplines, deepening our assessment skills and diagnostic acumen when evaluating children for delirium.
CONFLICTS OF INTEREST
The authors state that they have no competing interests to declare.



