


Introduction
During the past two decades cognitive models of obsessive-compulsive disorder have gained in momentum. In these models the notion of inflated responsibility is central, at least in Salkovskis' version of cognitive theory of OCD (Salkovskis et al., Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester, Richards, Reynolds and Thorpe2000). This means a tendency to perceive that one has a pivotal role in causing or hindering whether misfortune happens to self or others. Various correlational and experimental studies have supported the role of responsibility in OCD symptoms (Rachman, Thordarson, Shafran and Woody, Reference Rachman, Thordarson, Shafran and Woody1995; Salkovskis, Shafran, Rachman and Freeston, Reference Salkovskis, Shafran, Rachman and Freeston1999; Smári and Hólmsteinsson, Reference Smári and Holmsteinsson2001; Smári, Bouranel and Eiðsdóttir, Reference Smári, Bouranel and Eiðsdóttir2008; Yorulmaz, Altin and Karanci, Reference Yorulmaz, Altin and Karanci2008). The influence of responsibility on OCD symptoms may be subtle and even reciprocal as, for example, increased checking seems to induce increased responsibility as well as being increased by it in turn (Rachman, Reference Rachman2002). The question is how such generalized feelings of responsibility or responsibility attitudes arise in the first place.
Salkovskis and colleagues (Reference Salkovskis, Shafran, Rachman and Freeston1999) suggested that early experiences may bring about inflated responsibility. More precisely they hypothesized five different pathways to inflated responsibility. 1) Heightened responsibility as a child: This implies an experience of increased levels of responsibility in childhood. Children may be obliged to assume responsibility at an unusually young age, for instance be asked to perform tasks that are typically performed by adults. Thus a child might, because of parental incompetence, be expected to ensure that a slightly younger sibling gets safely in time to school every morning and take responsibility for his well-being in general; 2) Rigid and extreme codes of conduct as a child: This pathway refers to early exposure to rigid rules. Children may be taught to adhere to strict behavioral codes and led to believe that failure to do so may result in blame or punishment. An example might be a child that is supposed to refrain from revealing any signs of anger or disappointment as this might hurt the parents' feelings; 3) Overprotective and critical parenting leading to lack of experience with responsibility as a child: Attempts to protect the child from harm or danger may result in overprotective parenting. This parenting style may also increase the child's sensitivity to responsibility as a result of very limited experience of personal responsibility. As pointed out by Coles and Schofield (Reference Coles and Schofield2008), overprotection is not to be understood as an opposite of heightened responsibility on a continuum between high and low responsibility but rather as an independent dimension. An example might be a child that is constantly told that he/she cannot play with another child without a parent's consent as other children might lead him/her astray; 4) Incidents in which one's actions/inactions caused a serious misfortune: This pathway refers to the development of inflated responsibility after a catastrophic event that affected the welfare of oneself or others. With this type of event the individual believes that he or she played an important role in causing the event or that they failed to prevent it. An example might be a child that contaminated a younger sibling that became very sick with a flu; 5) Incidents where it appears that one's actions/inactions/thoughts influenced a serious misfortune: The final pathway is similar to the fourth pathway in that the individual believes that he/she contributed to serious misfortune to oneself or to someone else. However, in this pathway, the events are coincidental, such as having a thought about something bad happening. An example might be a child that in anger wished his grandfather to die and soon after the grandfather had a heart attack.
Salkovskis and colleagues (Reference Salkovskis, Shafran, Rachman and Freeston1999) suggested that these five pathways may interact with other factors in influencing responsibility. Salkovskis and colleagues (Reference Salkovskis, Shafran, Rachman and Freeston1999) further proposed that these different pathways are related; for example to generality-specificity of responsibility, speed of onset of OCD, whether there is co-occurring depression and that they are also related to dominant symptom patterns of OCD (for instance whether checking is predominant or not). For example, OCD onset was expected to be gradual if the person had experienced broad responsibility since childhood, overprotection or rigid rules, but sudden when following incidents affecting others' health or welfare.
Strangely enough, very little research effort has been dedicated to these interesting conjectures. Recently, however, Coles and Schofield (Reference Coles and Schofield2008) have, on the basis of Salkovskis and colleagues' (Reference Salkovskis, Shafran, Rachman and Freeston1999) suggestions, proposed a measure of these experiences: the Pathways to Inflated Responsibility Beliefs Scale (PIRBS). Items reflecting the five pathways defined by Salkovskis were constructed for the initial item pool. In an exploratory factor analysis of the PIRBS items the scree test suggested the extraction of four or five factors. However, the five-factor solution was judged unacceptable as only three items loaded on one of the factors and therefore a four-factor solution was retained. Items reflecting the first three pathways (Heightened Responsibility, Rigid Rules and Overprotection) emerged as clear factors, but items reflecting pathways 4 and 5 (actions caused misfortune and actions influenced misfortune) loaded on the same factor in the four-factor solution. A confirmatory factor analysis in a new sample yielded support for the four-factor solution even though the fit indices were only marginally acceptable (RMSEA = .08, CFI = .86, SRMR = .07). Consequently, four subscales were formed: these are Heightened Responsibility (HR), Rigid Rules (RR), Overprotection (OP) and Actions that caused or influenced misfortune (AIC). The last subscale is a combination of items representing pathways four and five. In Coles and Schofield's (Reference Coles and Schofield2008) study support for the convergent validity of the PIRBS was found through correlations between the Overprotection (OP) subscale and measures of parental protectiveness and parental authoritarianism on the Parental Bonding Instrument (Parker, Reference Parker1989), between the Heightened Responsibility (HR) subscale and a measure of childhood chores and between all subscales and the Overestimation of threat/responsibility subscale of the short version of the Obsessive Beliefs Questionnaire or OBQ-44 (Obsessive-compulsive working group, 2005). These correlations with Overestimation of threat/responsibility were higher than correlations with the other subscales of the OBQ-44. Furthermore, all subscales had significant moderate correlations with a measure of OCD symptoms (Obsessive-Compulsive Inventory or OCI; Foa, Kozak, Salkovskis, Coles and Amir, Reference Foa, Kozak, Salkovskis, Coles and Amir1998).
In the present study we address the psychometric properties of the PIRBS instrument in a different linguistic and cultural context. Further, we address the fundamental question of whether responsibility attitudes mediate between pathways to responsibility and obsessive-compulsive symptoms as implied by Salkovskis and colleagues' (Reference Salkovskis, Shafran, Rachman and Freeston1999) model. The aims of the present research were thus the following: 1) to investigate the psychometric properties of the Icelandic translation of the PIRBS, in particular the factor structure conducting a confirmatory factor analysis; 2) to investigate whether experiences addressed in PIRBS are related to inflated responsibility and to obsessive-compulsive symptoms in line with what has been suggested by Salkovskis and colleagues (Reference Salkovskis, Shafran, Rachman and Freeston1999) and Coles and Schofield (Reference Coles and Schofield2008); 3) test whether inflated responsibility mediates between PIRBS and OCD symptoms as may be expected from Salkovskis and colleagues' (Reference Salkovskis, Shafran, Rachman and Freeston1999) suggestions.
Method
Subjects
Three hundred undergraduate students from the University of Iceland served as subjects. One hundred and eighteen were males and 173 were females. Gender was unknown for 9 subjects. Thirty-five were between the ages of 18 and 20, 125 between the ages of 21 and 23, 50 between 24 and 25, and 81 were 26 years old or older. Nine subjects did not reveal their age.
Measures
Responsibility Attitudes Scale (RAS) (Salkovskis et al., Reference Salkovskis, Wroe, Gledhill, Morrison, Forrester, Richards, Reynolds and Thorpe2000). This is a 26-item scale for measuring responsibility attitudes. Items are rated on a scale between totally agree (1) and totally disagree (7). The psychometric properties of the Icelandic version of RAS have been found to be satisfactory (Smári and Hólmsteinsson, Reference Smári and Holmsteinsson2001).
Obsessive-Compulsive Inventory-Revised (OCI-R) (Foa et al. Reference Foa, Huppert, Leiberg, Langner, Kichic, Hajcak and Salkovskis2002). This is an 18-item inventory. There are six subscales, each with 3 items: (1) Washing; (2) Checking/doubting; (3) Obsessing; (4) Mental neutralizing; (5) Ordering; and (6) Hoarding. The items are rated on a 5-point scale between 0 = not at all and 4 = very much, with regard to how much the symptom has troubled the subject during the past week. The inventory was translated into Icelandic and then back-translated into English by an English speaking professional translator. Its psychometric properties in English college populations have been found satisfactory and the factor structure replicated (Hajcak, Huppert, Simons and Foa, Reference Hajcak, Huppert, Simons and Foa2004). The back-translation was compared to the original English version to ensure accuracy. The six-factor structure of the OCI-R has been confirmed in a confirmatory factor analysis with a large Icelandic sample (Smári, Ólason, Eyþórsdóttir and Frölunde, Reference Smári, Ólason, Eythorsdottir and Frölunde2007).
Pathways to Inflated Responsibility Beliefs Scale (PIRBS) (Coles and Schofield, Reference Coles and Schofield2008). The PIRBS is a 23-item instrument supposed to measure four different pathways to inflated responsibility. The four subscales of the PIRBS are the following: Heightened Responsibility (5 items); Rigid rules (5 items); Overprotection (5 items); and Actions caused/influenced (8 items). The items are rated on a scale between 0 = never and 4 = always. The scale was translated into Icelandic and then backtranslated into English to ensure accuracy.
Results
Confirmatory factor analysis
The most widely used estimates in structural equation modeling are derived from the Maximum Likelihood (ML) method (Anderson and Gerbing, Reference Anderson and Gerbing1988; Hu and Bentler, Reference Hu and Bentler1999) and in this study models were tested with that procedure, using the EQS 6.1 for covariance structure models (Bentler and Wu, Reference Bentler and Wu2002). However, there is less consensus over the different goodness of fit indices and their appropriate cut-off values (Hu and Bentler, Reference Hu, Bentler and Hoyle1995, Reference Hu and Bentler1999; MacCallum and Austin, Reference MacCallum and Austin2000; Marsh, Hau and Wen, Reference Marsh, Hau and Wen2004; Shevlin, Miles and Lewis, Reference Shevlin, Miles and Lewis2000). For example, the chi-square test will often suggest a poor fit, even when there is a very small discrepancy between the sample and fitted covariance matrices and a number of authors have recommended using additional fit indices (Bentler, Reference Bentler1995; Byrne, Reference Byrne1994; Cole, Reference Cole1987; Hu and Bentler, Reference Hu and Bentler1999). Following the recommendation of various authors, different goodness of fit tests were used to evaluate the fit of the models (Bentler and Wu, Reference Bentler and Wu2002; Hu and Bentler, Reference Hu and Bentler1999; MacCallum and Austin, Reference MacCallum and Austin2000). In addition to Chi-square, the comparative fit index (CFI; Bentler, Reference Bentler1990), the standardized root mean square residual (SRMR; Bentler, Reference Bentler1990) and the root mean square error of approximation (RMSEA; Browne and Cudeck, Reference Browne, Cudech, Bollen and Long1993; Steiger and Lind, Reference Steiger and Lind1980) were used. The range for the CFI is between zero and one, and values in the mid-90s or higher with a cut-off value close to 0.08 for the SRMR are taken to indicate an acceptable fit to the data (Hu and Bentler, Reference Hu and Bentler1999). RMSEA values less than .5 indicate a close fit to the model, values between .05 and 0.08 are acceptable fit, and values greater than .10 a poor fit (Browne and Cudeck, Reference Browne, Cudech, Bollen and Long1993).
Prior to the CFA, items were screened for deviation from the normal distribution. Skewness and kurtosis values were adequate for all items, except items 4, 16, 18, 19 and 20 to 23. Logarithmic transformations reduced skewness and kurtosis values for all items satisfactorily.
The factor structures that were assessed were the four-factor model of Coles and Schofield (Reference Cole2008), and the five-factor model corresponding to Salkovskis and colleagues' (Reference Salkovskis, Shafran, Rachman and Freeston1999) suggestions where there is a differentiation between actions influenced and actions causing misfortune. (see items expected to load on the five different factors in Table 1). The factors for both four- and five-factor models were allowed to correlate freely. The summary of results for the CFA for data is presented in Table 2. Inspection of the models presented in Table 1 reveals that neither of the models provide an optimal fit to the data. The CFI values are unacceptable according to the criteria from Hu and Bentler (Reference Hu and Bentler1999), although both SRMR and RMSEA suggest moderate fit to the data. The results also suggest a slightly better fit for the five-factor model.
Table 1. Items from the PIRBS and their classification according to their expected dominant loadings in a five-factor model. In the four-factor model items of the last two factors are expected load on the same factor
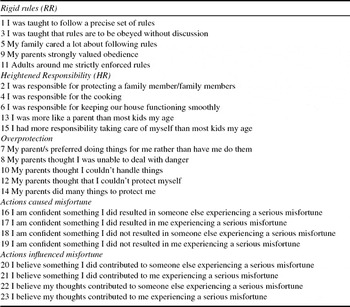
Table 2. Goodness of fit indices for the confirmatory factor structures of PIRBS

**p < .001. X2 = Chi square; CFI = Comparative Fit Index; RMSEA = Root Mean Squared Error of Approximation: a 90% population confidence interval for RMSEA; SRMR = Standardized Root Mean Square Residual.
Further inspection of the model parameters, suggest that item 14 “As a child my parent(s) did many things to protect me” was poorly defined by its appropriate factor (standardized coefficient = 0.19; R2 = 3,6%). Thus, the five-factor model was tested again without item 14, resulting in a slight improvement in model parameters; CFI = 0,85; SRMR = 0,07 and RMSEA = 0,08. (An exploratory factor analysis of the data set of this study yielded a four-factor structure that was very similar to the four-factor structure of Coles and Schofield (Reference Coles and Schofield2008) with the exception that item 14 did not load on the expected factor. We do not emphasize this result, however, as the exploratory and confirmatory factor analyses are conducted on the same data set and are thus not independent). In the following we use scales corresponding to the four-factor model of Coles and Schofield (Reference Coles and Schofield2008) rather than the somewhat better supported five-factor model in order to facilitate comparisons with the results of their study.
Descriptive statistics for the PIRBS, OCI-R and RAS
Means, standard deviations and alpha coefficients were calculated for the four PIRBS subscales and the total scale as well as for the OCI-R and RAS (Table 3).
Table 3. Means, standard deviations and alpha coefficients for the PIRBS total scale and subscales as well as for the RAS and the OCI-R (within brackets results from Coles and colleagues (Reference Coles and Schofield2008) for comparison)

AIC: Actions caused or influenced. RR: Rigid rules. HR: Heightened responsibility. OP: Overprotection.
Correlations between PIRBS, RAS AND OCI-R
Correlations were then calculated between PIRBS and its subscales and RAS and OCI-R (see Table 4).
Table 4. Correlations between PIRBS and its subscales, OCI and RAS

AIC: Actions caused or influenced. RR: Rigid rules. HR: Heightened responsibility. OP: Overprotection
All correlations coefficients p < .01 two-tailed except*.
The sample correlations between RAS and the total PIRBS as well as with the PIRBS subscales are slightly higher than the correlations of these scales with the OCI-R with the exception of the Actions caused or influenced subscale where OCI-R has a slightly higher sample correlation than the RAS (a comparison between the correlations with Steiger's (see Howell, Reference Howell2002) method of comparing dependent correlations revealed, however, that none of the differences was significant).
Does inflated responsibility mediate between pathways to responsibility and obsessive- compulsive symptoms?
In order to demonstrate statistical mediation, four conditions have to be satisfied (Baron and Kenny, Reference Baron and Kenny1986; MacKinnon and Dwyer, Reference McKinnon and Dwyer1993): 1) the predictor has to be associated with the mediator; 2) the predictor has to be associated with the outcome; 3) the mediator has to be associated with the outcome; 4) there has to be less association between the predictor and the outcome when the mediator is controlled for. Table 3 shows that the first three conditions are satisfied for inflated responsibility as a mediator between pathways to responsibility beliefs and OCD symptoms. In order to investigate whether the fourth condition was also satisfied, a regression analysis was conducted with OCD symptoms as the dependent variable and inflated responsibility and pathways as predictors (see Table 5).
Table 5. Hierarchical multiple regression. Dependent variable OCI-R. Dependent variables:RAS scores entered on step 1 and PIRBS scores entered on step 2

R2 step1 = .14 p < .001; R2ch step 2 = .06 p < .001.
The beta coefficient for pathways to responsibility beliefs (the independent variable) when RAS was also in the equation was reduced from .39 to .28. Then a Sobel test was conducted in order to test for the indirect effect. A value of z = 3.90 was found (p<.001). The results did thus support the mediation hypothesis.
Discussion
In cognitive theory inflated responsibility is expected to play a fundamental role in obsessive-compulsive symptoms. It is thus important to know how the so-called responsibility attitudes that according to theory generate inflated responsibility appraisals appear. A priori it may be expected that childhood experiences and parenting play an important role in their formation as proposed by Salkovskis and colleagues (Reference Salkovskis, Shafran, Rachman and Freeston1999).
The purpose of the present research was to investigate the properties of a new measure of developmental pathways to responsibility beliefs (Coles and Schofield, Reference Coles and Schofield2008) reflecting Salkovskis and colleagues' (Reference Salkovskis, Shafran, Rachman and Freeston1999) theory. We evaluated in a series of confirmatory factor analyses a four-factor model corresponding to Coles and Schofield (Reference Coles and Schofield2008), and a five-factor model distinguishing between actions causing and actions influencing misfortune happening to self or others in line with Salkovskis and colleagues' (Reference Salkovskis, Shafran, Rachman and Freeston1999) original suggestions. While neither the four- nor the five-factor solution was wholly satisfactory with respect to generally accepted criteria, the five-factor solution was somewhat better. It should be mentioned that Coles and Schofield's (Reference Coles and Schofield2008) four-factor solution for the PIRBS was similarly only marginally acceptable and these authors did not test the adequacy of a five-factor solution with CFA. We can however concur with Coles and Schofield (Reference Coles and Schofield2008), citing for example Marsh et al. (Reference Marsh, Hau and Wen2004) that people should beware of reifying “golden rules” for fit indices and that some published cut-off values may be overly conservative. We might thus interpret the results as at least suggestive of a four- or a five-factor solution. In order to facilitate a comparison with Coles and Schofield we decided to use their four PIRBS subscales instead of forming subscales based on the five-factor solution.
The internal consistency of most of the subscales as well as the PIRBS total scale was good. The exception was the overprotection scale (OP) that had a low internal consistency. The reasons for this are not clear. Two items of that scale had the lowest item-total correlations and problematic factor loadings (item 7, “my parents frequently preferred to do things for me rather than have me do them myself” and item 14, “my parents did many things to protect me” seem a bit out of tune with the others as they refer to parental protection in a neutral or a positive way whereas the other items refer more to overprotection in the context of low regard of the child's capacity). It should be noted that these two items had equally the lowest loadings of all items in Coles and Schofield's (Reference Coles and Schofield2008) CFA and an omission of item 14 improved the overall fit of the five-factor model in the present study. All four of the PIRBS scales showed significant correlations with inflated responsibility as well as with the OCI-R. These correlations are similar to those obtained by Coles and Schofield (Reference Coles and Schofield2008) and are consistent with a role played by the four pathways in generating responsibility and OCD symptoms. The scores of the PIRBS subscales are quite similar to those obtained by Coles and her colleagues with the exception of those of the AIC scale that were substantially lower than those obtained by Coles and her colleagues. The reasons for this are again unclear.
If inflated responsibility leads to obsessive-compulsive symptoms and the pathways to responsibility beliefs help to generate responsibility attitudes, the latter should mediate between the former and OCD symptoms. In line with this reasoning there was a strong support for the mediating role of inflated responsibility between pathways to responsibility beliefs and OCD symptoms as proposed by Salkovskis and colleagues (Reference Salkovskis, Shafran, Rachman and Freeston1999). While the mediation was significant there was, however, not at all full mediation between pathways to responsibility beliefs and OCD symptoms through inflated responsibility. The reasons for this may be that the pathways to responsibility beliefs influence other cognitive variables than responsibility such as perfectionism, that in turn may affect obsessive-compulsive symptoms. These possibilities should be elucidated in future research.
As the present study is cross-sectional, no definite conclusions can be drawn from the statistical mediation concerning causal influences. Future research should thus address more directly the role of different pathways to inflated responsibility beliefs with regard to how responsibility and OCD symptoms unfold and develop over time.
If the role of early experiences as those described by the PIRBS in the development of responsibility and in obsessive-compulsive symptoms is confirmed, this has obvious implications for treatment and prevention of obsessive-compulsive problems. Special attention should be given to children encountering many risk factors and attempts should be made to counteract and mitigate their influence through therapy or counseling, targeting in particular parental practices or any thoughts a child might have with regard to his/her influence in bringing about misfortune happening to self or others.
A further limitation of the present study, in addition to its cross-sectional design, is that it addresses responsibility and obsessive-compulsive symptoms only in a non-clinical population. It is obviously of interest to investigate whether the pathways to responsibility beliefs lead to responsibility and ultimately obsessive-compulsive symptoms in a clinical range.
In conclusion, the PIRBS measure seems to be a promising approach to study the important field of developmental precursors of inflated responsibility and OCD symptoms even though the factor structure may need a revision.






Comments
No Comments have been published for this article.