



Introduction
Demographic change is one of the most challenging social phenomena of modern societies, and the need for healthy ageing is of primary economic and social importance in the context of an ageing population. Successful ageing is a challenge that lies ahead of modern societies. In order to tackle this challenge, international and European organisations are working towards a paradigm shift on ageing. This new paradigm explains that success and wellbeing at this stage of life will be determined by physical and mental health as well as social, economic and cultural aspects, which together play a key role in how older people face the process of becoming older (Cosco et al., Reference Cosco, Prina, Perales, Stephan and Brayne2014; World Health Organization, 2015). In this regard, the World Health Organization (2015) has deployed the concept of healthy ageing, which ‘is about creating the environments and opportunities that enable people to be and do what they value throughout their lives’. Healthy ageing is not only determined by biological ageing health status and functionality but also by the capability of older adults to live well in later life (Yeung and Breheny, Reference Yeung and Breheny2016). Thus, this stage that occupies a third of our life is a new opportunity to continue developing ourselves at the physical, psychological and social level, and thus an opportunity for personal growth (Gladman, Reference Gladman2019).
Socio-economic environment, physical environment and the person's individual characteristics and behaviours are major determinants of both health (World Health Organization Commission on Social Determinants of Health, 2008) and successful ageing (Zanjari et al., Reference Zanjari, Sani, Chavoshi, Rafiey and Shahboulaghi2017). Many of these determinants may be grouped under the general heading of social determinants of health, in which living standards are embedded (Solar and Irwin, Reference Solar and Irwin2010).
Standard of living is a concept used to describe how well a person can live his or her life in terms of objective wellbeing. Different approaches to this concept have been developed: from a purely material approach based on income, wealth and other material assets to a more holistic approach which not only considers material wealth but also social and environmental goods, their utility or benefit, and individual's use of these goods (Sen, Reference Sen1987). In Sen's Capability Approach, a shift on how wellbeing and quality of life are measured occurred from a perspective based on ‘resources’ and ‘preferences’ to a perspective based on ‘capabilities’, where the focus is not only on the person, but also his or her context (Sen, Reference Sen2009). ‘Capability’ is described as what individuals are able to do and be, and the level of their freedom to pursue the lives they have reason to value (Sen, Reference Sen1999; Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016). Thus, it is necessary to pay attention to the material and social contexts of older people in order to understand and support their welfare regardless of health status (Gopinath, Reference Gopinath2018). The Capability Approach to healthy ageing should be seen as the outcome of an interaction between personal characteristics (i.e. gender, age, presence of disabilities, etc.), economic resources or assets (i.e. pensions), and the social (social norms, sexism, racism, etc.), economic and environmental (i.e. availability of adequate infrastructures) aspects (Yeung and Breheny, Reference Yeung and Breheny2016). In this sense, Sen's Capability Approach contributed to the design of the United Nations Development Programme Human Development Index which offers the possibility of comparing the wellbeing of countries (Sen, Reference Sen1992).
The importance attributed to the different aspects of living standards is subjective and varies across different age groups. The levels of living standards have been reported to increase with age (Groffen et al., Reference Groffen, Bosma, van der Akker, Kempen and van Eijk2008; Litwin and Sapir, Reference Litwin and Sapir2009; Breheny et al., Reference Breheny, Stephens, Alpass, Stevenson, Carter and Yeung2013). Lifetime accumulation of wealth may explain this tendency, as well as the change in the experiences and expectations of living standards and income as people age (Stoller and Stoller, Reference Stoller and Stoller2003; Berthoud et al., Reference Berthoud, Blekesaune and Hancock2006; Wilkinson, Reference Wilkinson2016). Moreover, living standards have been traditionally associated with quality of life by many authors stating that living standards are an important part of older people's quality of life (e.g. Lawton, Reference Lawton1983; Smith et al., Reference Smith, Langa, Kabeto and Ubel2005; Diener et al., Reference Diener, Harter and Arora2010). Both measures are, in turn, related to health – understood as physical and mental health – which has been shown to be affected by living standards and to have an effect on quality of life for older people (Fergusson et al., Reference Fergusson, Hong, Horwood, Jensen and Travers2001; Low and Mozahn, Reference Low and Molzahn2007).
Therefore, it is particularly important to measure living standards among older adults. To this aim, it is essential to have a living standards measure able to assess both the variety of living standards of older people and their change over time (Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016). One of the main instruments to assess living standards capabilities among older adults is the Living Standards Capabilities for Elders scale (LSCAPE) (Breheny et al., Reference Breheny, Stephens, Alpass, Stevenson, Carter and Yeung2013). This scale was developed based on Sen's Capability Approach. LSCAPE is a 25-item scale which include questions on a variety of living standards: health, social integration, contribution, enjoyment, security and restriction. The authors also proposed a short version of LSCAPE consisting of six items that are scored as in the original scale (Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016). This six-item version of LSCAPE has been included as part of the Healthy Ageing in Scotland study to assess living standards, which is the first long-term ageing study to improve the lives of elderly people in Scotland (Douglas et al., Reference Douglas, Rutherford and Bell2017).
LSCAPE was validated using the New Zealand Longitudinal Study of Ageing involving a sample of 2,968 older adults (aged 50–87 years) in New Zealand (Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016). The psychometric properties of the scale were evaluated by the authors with reliability and validity. Reliability results indicated excellent internal consistency of LSCAPE (Cronbach's alpha for the six sub-scales ranged from 0.81 to 0.90 and the total LSCAPE score was 0.96). Regarding the dimensional structure of LSCAPE, Confirmatory Factor Analysis (CFA) was performed indicating a six-factor structure.
At the time this study was performed, there was no official Spanish version of the scale. Therefore, the aims of the present study are: (a) to adapt and validate the LSCAPE for use in a Spanish population; (b) to examine the dimensionality, validity and reliability, using CFA, of LSCAPE in a sample of Spanish older people; and (c) to establish the convergent validity of LSCAPE with quality of life and a self-reported monthly income measure.
Method
Sample
The target population of this study was older population from the city of Valencia (Spain). Participants were recruited in two health centres between March 2017 and March 2018. The inclusion criteria were living independently, lacking severe cognitive impairment and having the capacity to provide informed consent. Consecutive patients meeting the inclusion criteria were invited to take part in the study by their general practitioners (GPs), with an acceptance rate of 69.7 per cent.
The final sample was composed of 411 home-dwelling older adults aged between 65 and 92 with an average age of 77 years, from which 38.32 per cent were men (169 persons) and 61.68 per cent were women (272 persons).
The analysis of the income of the participants revealed that 64.85 per cent of them (286 out of 441) had an income of €1,200 per month or less, while 17.69 per cent had an income between €1,200 and 1,700 (78 persons), 8.84 per cent between €1,700 and 2.300 (39 persons), and 7.03 per cent more than €2,300 (31 persons).
With regard to the household composition, 25.85 per cent of participants (114 persons) were living alone, 58.50 per cent were living with one more person (258 persons) and 15.65 per cent were living in households of three or more people (69 persons).
The socio-demographic characteristics of our study sample are similar to those of the target population: older adults living in the city of Valencia. In January 2018, there were 164,341 adults aged 65 and older in Valencia, of whom 40.4 per cent were men and 59.6 per cent were women (Ajuntament de València, 2019). Their average monthly income was €1,050.24 (Generalitat Valenciana, 2019), and 26.31 per cent of them were living alone and 18.76 per cent were living in households of three or more people (Ajuntament de València, 2019).
Procedure
Consecutive patients who visited health-care centres were invited by health professionals. The persons who agreed to participate in the study gave consent to provide the researchers with contact details and to be contacted by phone in the next two weeks. During the phone conversation, an appointment at the participant's home was set in order to administer the LSCAPE by a trained researcher. This study was approved by the Ethics Committee of Consorcio Hospital General Universitario and the Ethics Committee of Hospital Universitari i Politècnic La Fe, both from Valencia (Spain).
Measures
LSCAPE
LSCAPE is a 25-item scale based on Sen's Capability Approach that assesses the living standards of older people in terms of their capability of achieving valued functioning across six domains: health, social integration, contribution, enjoyment, security and restriction (Breheny et al., Reference Breheny, Stephens, Alpass, Stevenson, Carter and Yeung2013). Each item is responded to on a five-point Likert-type scale ranging from 1 (‘not at all true for me’) to 5 (‘definitely true for me’), with a total score that ranges from 25 to 125; the higher the score, the higher the living standards.
In the framework of this study, a Spanish version of LSCAPE (see Table 1) was developed using the back-translation method (Brislin, Reference Brislin1970). Two bilingual translators translated and adapted the items from English to Spanish and two different translators translated it back to English. The authors of this study verified the semantic equivalence of the translated version towards the original scale.
Table 1. Spanish version of the Living Standards Capabilities for Elders scale (LSCAPE)

Short-Form Health Survey version 2
The Spanish version of the Short-Form Health Survey version 2 (SF-12v2) (Vilagut et al., Reference Vilagut, Valderas, Ferrer, Garin, López-García and Alonso2008) was used to measure the quality of life of older people in order to assess convergent and discriminant validity of LSCALE. SF-12v2 is a reliable and valid instrument for measuring health status, and physical and mental wellbeing. It consists of 12 items which are rated on a three- or five-point Likert scale. The items are condensed into two summary components – Physical Health and Mental Health – which demonstrated high internal consistency in our sample (0.90 and 0.81, respectively).
Monthly income
Monthly personal income in euros was assessed with a five-point self-reported response: <700; 700–1,200; 1,200–1,900; 1,900–2,700; >2,700. This measure was also used to assess the convergent and discriminant validity of LSCALE.
Data analysis
Firstly, CFA was carried out using the MPlus program (version 8) to test the fit of the 25-item LSCAPE Six-factor Model (Breheny et al., Reference Breheny, Stephens, Alpass, Stevenson, Carter and Yeung2013, 2016) for the whole sample (N = 441). The Weighted Least Square Mean and Variance Corrected method was employed to estimate the model and to overcome the non-normality and ordinal nature of the items (Finney and DiStefano, Reference Finney, DiStefano, Hancock and Mueller2006).
The goodness of fit was determined through the estimated factor loadings which are significant when associated p-values of the t-test are lower than 0.001, and using the following statistics: χ2, Standardised Root Mean Square Residual (SRMR), Comparative Fit Index (CFI) and Tucker–Lewis Index (TLI). The overall model fit is considered acceptable if: the probability of SRMR is close to 0, CFI ⩾ 0.9 and TLI ⩾ 0.9 (Hu and Bentler, Reference Hu and Bentler1999).
Discriminant and convergent validity of the model were assessed using Average Variance Extracted (AVE). According to the Fornell–Larcker testing system (Fornell and Larcker, Reference Fornell and Larcker1981), discriminant validity can be assessed by comparing the amount of the variance capture by the factor and the shared variance with other factors. Thus, the levels of the square root of the AVE for each factor should be greater than the correlation involving the factors. On the other hand, AVE values higher than 0.5 indicate good convergent validity (Hair et al., Reference Hair, Black, Babin and Anderson2010).
The reliability (internal consistency) of the scale was demonstrated as good by Composite Reliability (CR) indices with values > 0.7 (Hair et al., Reference Hair, Black, Babin and Anderson2010) and Cronbach's alpha with values > 0.7.
Finally, convergent validity was analysed using Spearman rank correlation co-efficient (rho) – as the data followed a non-normal distribution – to determine the strength of the relationship between LSCAPE sub-scales and the SF-12 sub-scales and monthly personal income. The strength of correlation was interpreted as high (rho > 0.7), moderate (0.4–0.7) and low (<0.4) (Akoglu, Reference Akoglu2018).
Results
Dimensionality
CFA has been used to test the fit of the 25-item LSCAPE Six-factor Model. Six dimensions were obtained: health care, social integration, contribution, enjoyment, security and restriction. As shown in Table 2, fit measures for all these dimensions present appropriate values: SRMR is lower than 0.09; CFI and TLI are higher than 0.9.
Table 2. Goodness-of-fit indexes of the model

Notes: N = 441. LSCAPE 6F: 25-item Living Standards Capabilities for Elders scale Six-factor Model. p: probability of χ2. SRMR: Standardised Root Mean Square Residual. CFI: Comparative Fit Index. TLI: Tucker–Lewis Index.
The convergent validity of the six-factor model was demonstrated since the AVE for each of the six factors is higher than 0.5, as well as the factor loadings which present significant values over 0.5 (Hair et al., Reference Hair, Black, Babin and Anderson2010), as shown in Table 3. Moreover, discriminant validity has been confirmed because the square root of the AVE between each pair of factors is higher than the estimated correlation between those factors, as shown in Table 4.
Table 3. Analysis of dimensionality, convergent validity and reliability of the Living Standards Capabilities for Elders scale (LSCAPE)

Notes: AVE: Average Variance Extracted. CR: Composite Reliability.
Table 4. Discriminant validity of the Living Standards Capabilities for Elders scale (LSCAPE)
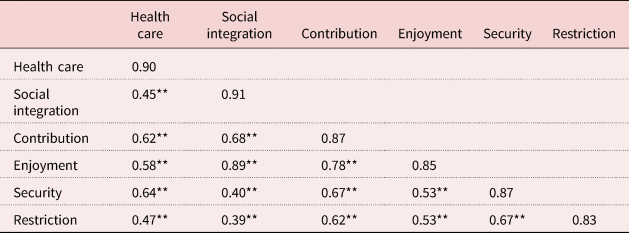
Notes: Diagonal: square root of Average Variance Extracted (AVE); below the diagonal: correlation estimated between the factors. Discriminant validity = square root of AVE greater than inter-construct correlations.
Significance level: ** p < 0.01.
Reliability of LSCAPE
The reliability of LSCAPE was proved since the CR index of each factor was higher than 0.7 (Hair et al., Reference Hair, Black, Babin and Anderson2010), as shown in Table 3.
Convergent validity of LSCAPE
Correlations between LSCAPE (total score and its six sub-scales) and SF-12 sub-scales and monthly personal income are reported in Table 5. Spearman's correlations found that LSCAPE is significantly related to both self-reported measures, especially in the case of SF-12 sub-scales (>0.60). LSCAPE total score, as well as the social integration and contribution sub-scales of LSCAPE, showed moderate to strong relationships with the SF-12 Physical Health and Mental Health sub-scales (>0.60 in all cases). However, a low correlation between LSCAPE and monthly personal income was found for the total score and the sub-scales.
Table 5. Correlations between the Living Standards Capabilities for Elders scale (LSCAPE), Short-Form Health Survey (SF-12) and monthly personal income

Significance level: ** p < 0.01.
Discussion
The present study was intended to analyse, for the first time, the psychometric properties of LSCAPE in a sample of Spanish older adults (>65 years), a population for whom living standards capabilities are particularly relevant due to its influence on healthy ageing.
The CFA of the 25-item LSCAPE revealed that the six-factor model fitted well to the data and the scale items loaded on the same factors as in the solution found by the authors of the scale (Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016). Therefore, our findings support the original six-factor structure of LSCAPE.
Reliability results indicated excellent internal consistency of LSCAPE as found in the original study (Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016). This means that our Spanish-validated version of the LSCAPE offers an accurate, reproducible and consistent measure of living standards.
Moreover, LSCAPE has been shown to be a reliable and valid instrument to assess living standards. Regarding convergent validity, positive correlations have been shown between the LSCALE total score and SF-12 sub-scales (Physical Health and Mental Health). According to McGregor and Goldsmith (Reference McGregor and Goldsmith1998), both concepts, living standards and quality of life, are inherently related to the other; thus, quality of life would be one's perception of and satisfaction with one's reality and living standards would reflect one's actual reality. Following this trend, similar results have been shown by other authors. Increased capabilities (measured by LSCAPE) were associated with greater subjective wellbeing among a sample of older people (Yeung and Breheny, Reference Yeung and Breheny2016). Also, capabilities – together with purpose in life – were highlighted as the most important predictors of quality of life among older people diagnosed with a disability (Yeung and Breheny, Reference Yeung and Breheny2019).
Furthermore, moderate relationships between the LSCAPE and monthly income values have been reported, which is line with results obtained by the authors of the scale (Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016), especially in the case of restriction and security sub-scales, which contain items about economic issues in comparison to the other four sub-scales. This outcome is in line with other authors in the literature. For instance, Jensen et al. (Reference Jensen, Krishnan, Hodgson, Sathiyandra and Templeton2006) found that living standards of older people from New Zealand were not significantly associated with their income. In the same line, living standards and quality of life values did not consider monetary indicators in a huge comparative study across 170 African countries using Sen's Capability Approach (Bérenger and Verdier-Chouchane, Reference Bérenger and Verdier-Chouchane2007). Additionally, economic living standards did not contribute significantly to wellbeing values among the oldest older participants of a study performed using the Capability Approach (Yeung and Breheny, Reference Yeung and Breheny2016). The lack of strong association between living standards and income found in our study can be explained by the ‘adaption hypotheses’ as older people, on average, need less income to achieve a given living standard in comparison to younger people. Thus, older people adapt their preferences and needs to their economic situation with a decreased perception of financial hardship (Berthoud et al., Reference Berthoud, Blekesaune and Hancock2006, Reference Berthoud, Blekesaune and Hancock2009). In line with this, Hansen et al. (Reference Hansen, Slagsvold and Moum2008) showed that older people tend to report higher financial satisfaction (even in cases of very low incomes) in comparison to younger people, whose financial satisfaction used to depend more on their income levels. Older people tend to adapt to their financial situation through establishing new goals (active coping) and adjusting aspirations to the given situation (passive coping).
Some limitations should be stated. To date, only the original study on the development and validation of LSCAPE (Breheny et al., Reference Breheny, Stephens, Henricksen, Stevenson, Carter and Alpass2016) has analysed this scale which makes it difficult to compare our results with previous findings. On the other hand, although the sample size was adequate for carrying out psychometric analysis of LSCAPE, the sample population was collected from a specific Spanish region which does not permit the results to be generalised for the whole Spanish population and it may be biased in terms of participants’ health status because of recruitment through health-care centres. In this regard and as future recommendations, the authors of this study suggest conducting replication and extension studies on the validity of the Spanish version of LSCAPE in other Spanish regions.
Conclusion
To our knowledge, this is the first study that uses LSCAPE among a Spanish population. These results led to the conclusion that LSCAPE had an acceptable fit in the 25-item six-factor model in the Spanish population, demonstrating that LSCAPE is a reliable and valid instrument to assess living standards capabilities among the Spanish older population.
In sum, outcomes of this paper, besides the validation of LSCAPE among the Spanish older population, provide evidence on how living standards are related to both physical and mental wellbeing. Using measurement tools based on Sen's concept of capabilities that include a quality-of-life approach not only centred on the person but also on the interaction with his or her context (social, material and environmental factors), offers relevant information about the opportunities of older people to access resources, services or assets that impact on their wellbeing. Thus, LSCAPE provides a comprehensive output that could be interesting to Spanish decision and/or policy makers to take into consideration what is important for older people when designing social policies (i.e. revision of pensions, more services and infrastructures adapted to older people's needs, more in-kind services, etc.).
Acknowledgements
We would like to thank all participating older persons as well as health organisations and professionals involved in the study.
Author contributions
The authors have contributed to the manuscript as follows: TA-B in the conception and design of the study, in the analysis and interpretation of data, and drafting the manuscript; AD-M in the analysis and interpretation of data, and drafting the manuscript; and JG-F in the conception of the study and critically reviewing the content of the manuscript. Finally, all authors explicitly approved the final version of the manuscript.
Financial support
This study was supported by funding under the II and III Programme of the European Commission through the R&D projects UHCE [‘Urban Health Centre 2.0: Integrated Health and Social Care Pathways, Early Detection of Frailty, Management of Polypharmacy and Prevention of Falls for Active and Healthy Ageing in European Cities’] (reference number 533157) and APPCARE [‘Appropriate Care Paths for Frail Elderly Patients: A Comprehensive Model’] (reference number 664689). The financial sponsors had no role in the design, execution, analysis and interpretation of data, or writing up of the study.
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
The study cited in this article has been performed according to ethical guidelines and legal requirements at the Spanish level assuring confidentiality, privacy and security of data processed. Moreover, the study was approved by the Ethics Committee of Consorcio Hospital General Universitario, Valencia on 30 April 2015 and the Ethics Committee of Hospital Universitari i Politècnic La Fe, Valencia on 7 November 2016.





