


Introduction
Zenker's diverticulum is a pharyngoesophageal outpouching of mucosa and submucosa through Killian's dehiscence. The latter is a triangular weak spot between the oblique fibres of the thyropharyngeus muscle and the cricopharyngeus muscle, both of which are components of the inferior pharyngeal constrictor muscle, described by Killian in 1908.Reference Sen, Kumar and Bhattacharyya1,Reference Prisman and Genden2 The outpouching consists of mucosa and submucosa without muscle, and is therefore more accurately classified as a pseudodiverticulum.Reference Prisman and Genden2,Reference Law, Katzka and Baron3
This dehiscence was first discovered in 1769 by Ludlow. He identified it as an abnormal dilatation in the posterior pharyngeal wall during the post-mortem examination of a patient who, during life, complained of dysphagia.Reference Siddiq4 Later, in 1877, von Zenker and von Ziemsen proposed that the intraluminal forces within the pharynx act against an area of restriction.Reference Nguyen and Urquhart5
The cricopharyngeus muscle has been found to be the muscle primarily responsible for the muscular tone of the region.Reference Ferreira, Simmons and Baron6 This muscle attaches to either side of the cricoid cartilage without a median raphe, and therefore lies as a muscular swing around the inlet to the oesophagus.Reference Ferreira, Simmons and Baron6,Reference van Overbeek7 The thyropharyngeus muscle runs between the oblique line of the thyroid cartilage and then inserts in the posterior midline of the pharyngeal raphe. The pharyngeal raphe runs from the base of the skull, as a fibrous band, and is the attachment for all of the constrictors.Reference Ferreira, Simmons and Baron6
This study aimed to investigate the propensity for Zenker's diverticulum to occur on the left side by examining the muscle thickness in Killian's dehiscence, and to explore possible correlations between muscle thickness and sex, height and age.
Materials and methods
Patients
Once ethical clearance was granted, the data for the study were collected (by authors SM and NAF, and Dr MO Kwete) from human cadavers donated to the School of Anatomical Sciences at the University of the Witwatersrand, Johannesburg. The study initially included 110 Caucasian cadavers; all those included in the study had died aged over 40 years. Only 1 female cadaver was excluded from the study, in 2016, leaving us with 109 cadavers in total, 52 male and 57 female. This cadaver was excluded because the cause of death was disseminated carcinoma of an unknown type.
Killian's dehiscence, a triangular, full-thickness portion of tissue, approximately 1.5 × 2 cm in size, was excised from all cadavers (Figure 1).
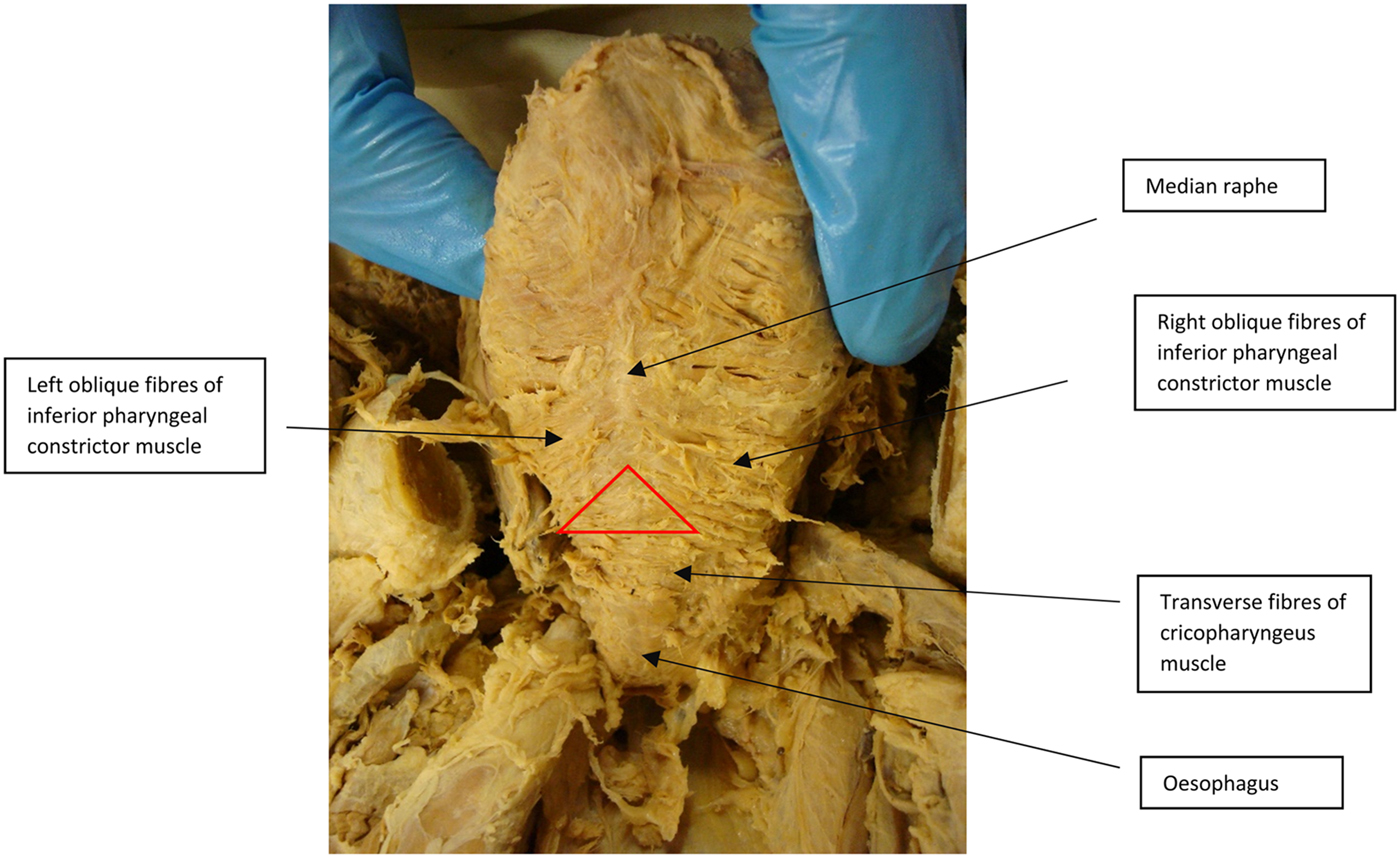
Fig. 1. Indicates Killian's triangle (red triangle), the muscular borders of the triangle and the oesophagus.
This portion of tissue was excised along the borders of Killian's triangle; namely, the inferior border of the oblique inferior constrictor muscle and the superior border of the cricopharyngeus muscle from the posterior wall of the pharynx. The specimen was orientated using ink (the right-hand side was marked in red and the left-hand side in green), immediately after excision, and placed into a specimen bottle (Figure 2).
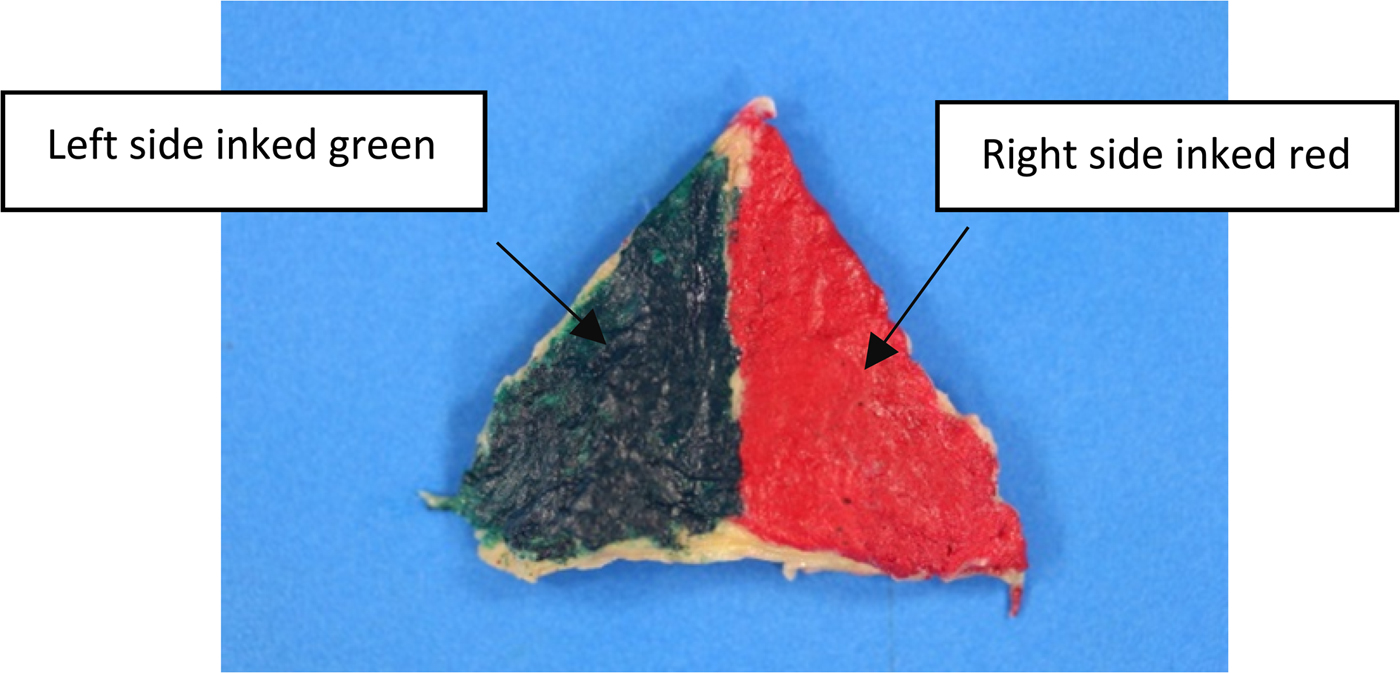
Fig. 2. Excised triangular portion of tissue, showing the orientation.
Each specimen bottle was labelled with the accession number assigned to the cadaver by the School of Anatomical Sciences for anonymous use throughout the study. This enabled subsequent correlation of the specimen with each cadaver's sex, length or stature, and age (these details were provided by the School of Anatomical Sciences).
Histopathological process
The processing of specimens was carried out at Dr Gritzman and Thatcher Laboratories. Each triangular portion of tissue was longitudinally cut into nine 2–3 mm thick sections. Four longitudinal sections were sampled from each cadaver, including the left lateral, left medial, right medial and right lateral aspects of Killian's dehiscence (Figure 3). These samples were then embedded in wax and cut with a microtome at 5 µm thickness. They were then placed on microscope slides, and stained with haematoxylin and eosin (Figure 4).

Fig. 3. Shows the four samples taken from the excised triangular portion of tissue.
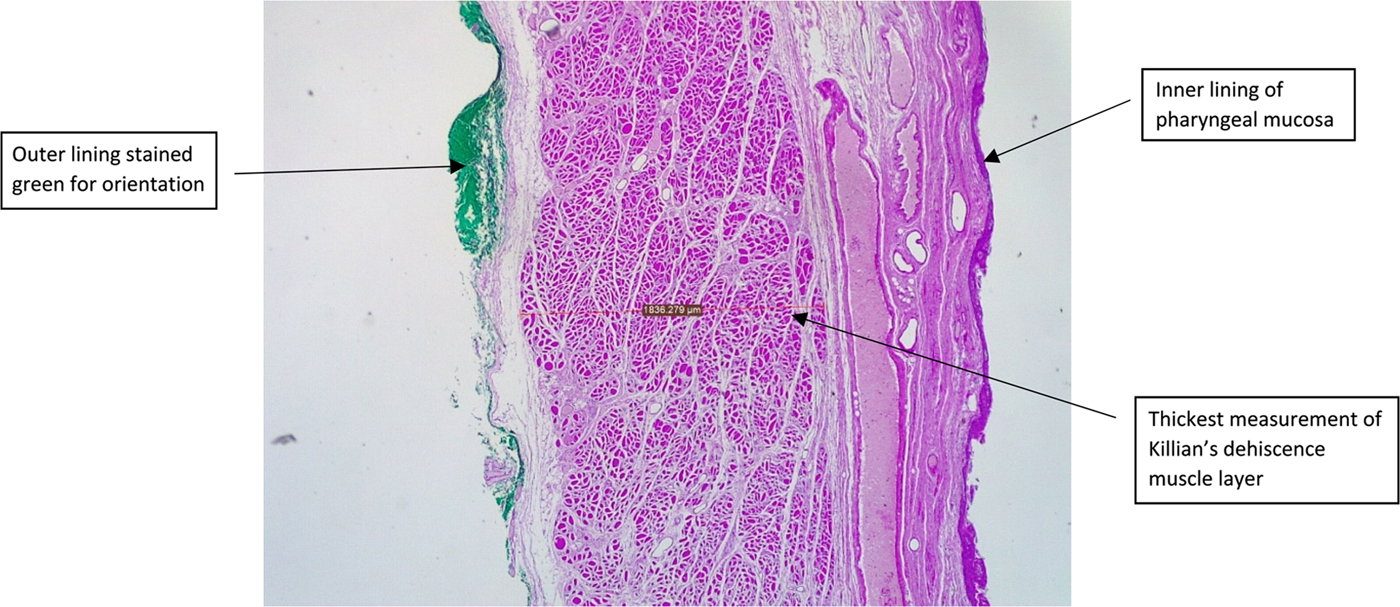
Fig. 4. Microscopic image showing a longitudinal section through Killian's dehiscence. It demonstrates the thickest measurement of the muscle layer. (H&E; ×25)
Data analysis
Muscle layer identification
The layer of muscle was identified using a Leica ICC50 W microscope at 25× magnification. A digital image was transmitted from the microscope camera to Leica Application Suite software platform on a computer, where images were captured and analysed further.
Muscle layer size
Both the thickest and the thinnest portions of muscle in the four sampled sections (left lateral, left medial, right medial and right lateral) were measured, with a total of eight measurements for each cadaver. The measurements, calculated to the nearest one-thousandth of a micrometer, were all taken by the same operator to ensure consistency. Each measurement was taken perpendicular to the mucosal layer.
Statistical analysis
Mean values for the thickest and thinnest measurements of muscle for each of the four samples (left medial, left lateral, right medial and right lateral) were used. When necessary, the mean of the individual thickest and thinnest muscle layer was used for each of the four samples.
For the main hypothesis, parametric testing was conducted with the paired student's t-test using RStudio statistical software.8,9 For the sub-hypotheses, different combinations of tests were used. In order to explore a correlation between muscle thickness and age, a manual non-parametric test was performed using Microsoft Excel spreadsheet software. To test for a correlation between muscle thickness and length or stature, a Pearson correlation test in RStudio was used for parametric testing.8,9 The impact of sex on muscle thickness was determined using chi-square tests of independence.10
During sample collection and data recording, a difference was observed between the medial and lateral samples. This difference was further investigated statistically using a paired student's t-test for parametric testing in RStudio.8,9
Results
The 52 male cadavers in the study had a mean age of 78.7 years and a mean height of 172.9 cm. The 57 female cadavers had a mean age of 77.4 years and a mean height of 159.9 cm. All cadavers were of Caucasian ethnicity.
In order to compare the muscle thickness of the four samples taken (left lateral, left medial, right medial and right lateral), parametric testing, by means of a paired student's t-test, was conducted.8 The left side was found to be significantly thinner than the right side, in both its medial and lateral aspects (Table 1, Figure 5).
Table 1. P-values of muscle thickness of left and right sides, in their medial and lateral aspects


Fig. 5. Graphs of left versus right (a) medial and (b) lateral average muscle thicknesses of the 109 specimens.
A negative correlation between the muscle thickness of Killian's dehiscence and age was tested using non-parametric testing. In both the medial and lateral aspects of the left and right sides, the p-value was found to be more than 0.05. Therefore, it cannot be said that there was a significant correlation between age and the muscle thickness of Killian's triangle (Table 2).
Table 2. P-values for mean thickness of right and left sides, in their medial and lateral aspects, versus age

A negative correlation between the muscle thickness of Killian's triangle and the height or stature of the cadavers was explored using parametric testing. A Pearson correlation test revealed no statistically significant correlation between muscle thickness and height or stature for either the medial or lateral aspects in the left and right sides (Table 3).9
Table 3. P-values for mean thickness of right and left sides, in their medial and lateral aspects, versus height or stature

Chi-square tests of independence were used to determine whether sex had any impact on the muscle thickness of Killian's dehiscence.10 No significant correlation was found between muscle thickness and sex (Table 4).
Table 4. P-values of muscle thickness of left and right medial and lateral aspects, in their thinnest areas, versus sex

The muscle thicknesses from the lateral samples of Killian's triangle were compared to those of the medial samples, for both the right and left sides. Parametric testing using a paired student's t-test revealed that muscle thickness was significantly thinner in the medial aspect than in its lateral counterpart, in both the right and left sides (Table 5, Figure 6).
Table 5. P-values for muscle thickness of medial versus lateral aspects of both left and right sides


Fig. 6. Graph of left medial versus left lateral average muscle thickness of the 109 specimens.
Discussion
As the cricopharyngeus is not anchored to the raphe, it has the ability to move independently away from the thyropharyngeus constrictors that lie above it as the oesophagus shortens along its long axis. Over time, a gradually increasing gap may develop between the abovementioned structures. This gap could allow possible herniation due to an increase in the intraluminal pressure caudal to thyropharyngeus, but cephalad to the cricopharyngeus muscle.Reference Sasaki, Ross and Hundal11
Killian's dehiscence has been widely researched in order to determine why it is an area of weakness. van Overbeek postulated that individuals with longer necks may have a longer Killian's triangle. This could predispose such individuals, more so than people with shorter necks, to potential herniation of the mucosa and submucosa. In longer necks, Killian's triangle would have to descend further away from the base of the skull and subsequently from the median pharyngeal raphe. This could explain the geographical differences in the incidence of this condition.Reference van Overbeek7
It is now widely accepted that there is an altered compliance of the cricopharyngeus muscle which causes impaired relaxation of the upper oesophageal sphincter, resulting in impairment of sphincter opening. This impaired opening will cause a raised intrabolus pressure, leading to herniation through the weakened area.Reference Law, Katzka and Baron3,Reference Siddiq4,Reference Ferreira, Simmons and Baron6
Histologically, it has been found that the cricopharyngeus muscle, in patients with Zenker's diverticulum, has extensive fibroadipose tissue replacement (more than 50 per cent) and muscle fibre degeneration, resulting in the replacement of normal muscle and normal connective tissue.Reference Law, Katzka and Baron3,Reference Siddiq4,Reference van Overbeek7,Reference Cook, Bumbergs, Cash, Jamieson and Shearman12 This leads to compromised elasticity and opening of the sphincter, and, in turn, to increased intraluminal pressure. Other findings include increased fibrosis of the cricopharyngeus muscle.Reference Sen, Kumar and Bhattacharyya1,Reference Ferreira, Simmons and Baron6 This further contributes to the increased intraluminal pressure due to stiffness and decreased compliance of the muscle.
Presentation
Zenker's diverticulae usually occur in patients in their seventh or eighth decade of life, and occur rarely in patients aged under 40 years.Reference Law, Katzka and Baron3 Patients present complaining most often of dysphagia and regurgitation, and occasionally of a soft lump in the left side of the neck (Boyce sign) and halitosis.Reference Prisman and Genden2,Reference Law, Katzka and Baron3,Reference Ferreira, Simmons and Baron6 The presence of cervical borborygmi is pathognomonic of Zenker's diverticulae. The pseudodiverticulum is found to occur predominantly in men, with an overall prevalence of 0.01–0.11 per cent in the general population in the USA and of 2 per 100 000 people per year in the UK.Reference Law, Katzka and Baron3,Reference Ferreira, Simmons and Baron6
The incidence has been found to be higher in Northern Europe than in Southern Europe.Reference Ferreira, Simmons and Baron6 It has been found to occur less frequently in Indonesia and Japan than it does in Canada, USA and Australia. These variations in geographical incidence may be a result of varying average heights in different geographical regions of the world. The average height for men in Norway and Sweden (Northern European countries) is 179.1 cm and 178.1 cm respectively, and the average female height for women in these countries is 165.9 cm and 164.7 cm respectively. In comparison, the average height for men in France and Spain (Southern European countries) is 173.4 cm and 170.3 cm respectively, and the average height for women in these countries is 161.9 and 160.4 cm respectively.Reference Cavelaars, Kunst, Geurts, Crialesi, Grötvedt and Helmert13 The higher incidence for the typically taller populations in Northern European countries supports the theory postulated by van Overbeek mentioned earlier.Reference van Overbeek7
The pseudodiverticulum is most often found on the left side of the neck, with only 10 per cent of Zenker's diverticulae found on the right side.Reference Sen, Kumar and Bhattacharyya1,Reference Siddiq4 Westrin et al. postulated that this could be explained anatomically by the potential space between the left carotid artery and the concavity of the cervical oesophagus.Reference Westrin, Ergün and Carlsöö14 Stafford et al. have suggested that the difference in the side where the outpouching occurs may be related to a patient's handedness (wherein the pseudodiverticulum occurs on the side opposite to the patient's handedness).Reference Stafford, Moore-Gillon and McKelvie15
• This study aimed to investigate the propensity for Zenker's diverticulum to occur on the left side
• It examined muscle thickness in Killian's dehiscence in 109 Caucasian cadavers, and correlations between muscle thickness, sex, height and age
• The results showed a significant difference in muscle thickness between the left and right sides of Killian's dehiscence
• The findings suggest there is a reason why Zenker's diverticulum occurs predominantly on the left side
• The study also revealed a significant difference in muscle thickness between the medial and lateral aspects of Killian's triangle
Given the propensity for Zenker's diverticulum to occur on the left side of the neck, it has become standard procedure, when performing a diverticulectomy, to carry out the cervicotomy over the anterior border of the left sternocleidomastoid muscle.Reference Law, Katzka and Baron3,Reference Nguyen and Urquhart5,Reference Ruiz-Tovar, Pérez de Oteyza, Collado, Rojo and García-Villanueva16
Conclusion
The study demonstrates a significant difference in muscle thickness between the left and right sides of Killian's dehiscence. The findings suggest there is a reason why Zenker's diverticulum occurs predominantly on the left side. The study also revealed a significant difference in muscle thickness between the medial and lateral aspects of Killian's triangle.
Acknowledgements
The authors would like to acknowledge: the School of Anatomical Sciences (University of the Witwatersrand), Dr Brunton Wium (anatomical pathologist) of Dr Gritzman and Thatcher Laboratories, Ms Kate Dudley (statistician).
Competing interests
None declared











