Introduction
Intranasal steroid sprays are fundamental in the medical management of inflammatory nasal conditions including allergic rhinitis and chronic rhinosinusitis.Reference Mygind 1 – Reference Fokkens, Lund, Mullol, Bachert, Alobid and Baroody 3 Several intranasal steroid sprays are currently available in the UK, including beclomethasone, triamcinolone, budesonide, mometasone and fluticasone.Reference Chong, Head, Hopkins, Philpott, Burton and Schilder 4 These sprays enable the direct application of steroids to the nasal mucosa to decrease inflammation, which reduces systemic effects and allows for continued use. This is particularly important in the treatment of children where systemic steroids can affect growth; intranasal steroid sprays have been approved for use in children as young as two years old.Reference Sheth 5
Recent systematic reviews have demonstrated the effectiveness of intranasal steroid sprays for chronic rhinosinusitis and allergic rhinitis.Reference Al Sayyad, Fedorowicz, Alhashimi and Jamal 6 , Reference Chong, Head, Hopkins, Philpott, Schilder and Burton 7 However, this efficacy can be affected by the method of delivery, and several spray application positions have been described in the literature. Nasal sprays may be applied in a contralateral fashion, for example right hand to left nostril (Figure 1), or an ipsilateral fashion, for example right hand to right nostril (Figure 2). Furthermore, the patient may adopt different head positions: head down (Figure 3), head neutral (Figure 4) and head up (Figure 5).

Fig. 1 Contralateral spray technique.

Fig. 2 Ipsilateral spray technique.

Fig. 3 Head down position.

Fig. 4 Head neutral position.

Fig. 5 Head up position.
A number of studies have investigated the intranasal distribution of steroid using an intranasal steroid spray with these different application techniques.Reference Bateman, Whymark, Clifton and Woolford 8 – Reference Aggarwal, Cardozo and Homer 10 Generally, the intranasal steroid spray is delivered only to the anterior portion of the nasal cavity, despite different application methods. Hence, there is likely to be little measurable difference in symptom control with different methods. Benninger and colleagues, in 2004, reviewed all relevant studies, and found a lack of evidence that intranasal steroid application instructions can maximise efficacy.Reference Benninger, Hadley, Osguthorpe, Marple, Leopold and Derebery 11 However, the authors do recommend a seven-step technique, with an upright head neutral position and use of the contralateral hand to apply the steroid spray, based on the opinion of their expert panel.Reference Benninger, Hadley, Osguthorpe, Marple, Leopold and Derebery 11
It is interesting to note that despite the studies debating the relative merits of these techniques in terms of managing nasal symptoms, few papers have investigated the acknowledged link between spray technique and side effects, including nasal irritation, nasal burning and epistaxis.Reference Al Sayyad, Fedorowicz, Alhashimi and Jamal 6 In one study, patients who developed epistaxis from intranasal steroid spray use were significantly more likely to experience this on the side of their dominant hand (p < 0.001), suggesting an ipsilateral technique on this side.Reference Benninger 12 This adds to the expert opinion favouring a contralateral technique,Reference Benninger, Hadley, Osguthorpe, Marple, Leopold and Derebery 11 though this message may not be communicated effectively to patients.
After a discussion within our department demonstrated that multiple different methods were being recommended to patients by our team, we sought to investigate the incidence of side effects experienced. Furthermore, we wanted to assess the effect that these issues had on patient compliance. We aimed to use this information to provide more accurate advice to our patients.
Materials and methods
A survey was administered to patients using an intranasal steroid spray who were seen at the Aberdeen Royal Infirmary rhinology clinic over a period of three months. Participants were asked about their intranasal steroid spray use, spray technique, associated side effects and compliance (Appendix 1).
Results
A total of 103 fully completed questionnaires were obtained. The mean age of participants was 45 years (range, 18–82 years; median, 45 years). Of the 103 patients, 48 were female (46.6 per cent) and 55 were male (53.4 per cent).
Intranasal steroid spray types
The most common intranasal steroid sprays used were mometasone furoate (Nasonex®) (28 per cent), beclometasone dipropionate (Beconase®) (20 per cent) and fluticasone propionate (Flixonase®) (19 per cent). Twenty-four per cent of patients did not know which intranasal steroid spray they were using (Figure 6).
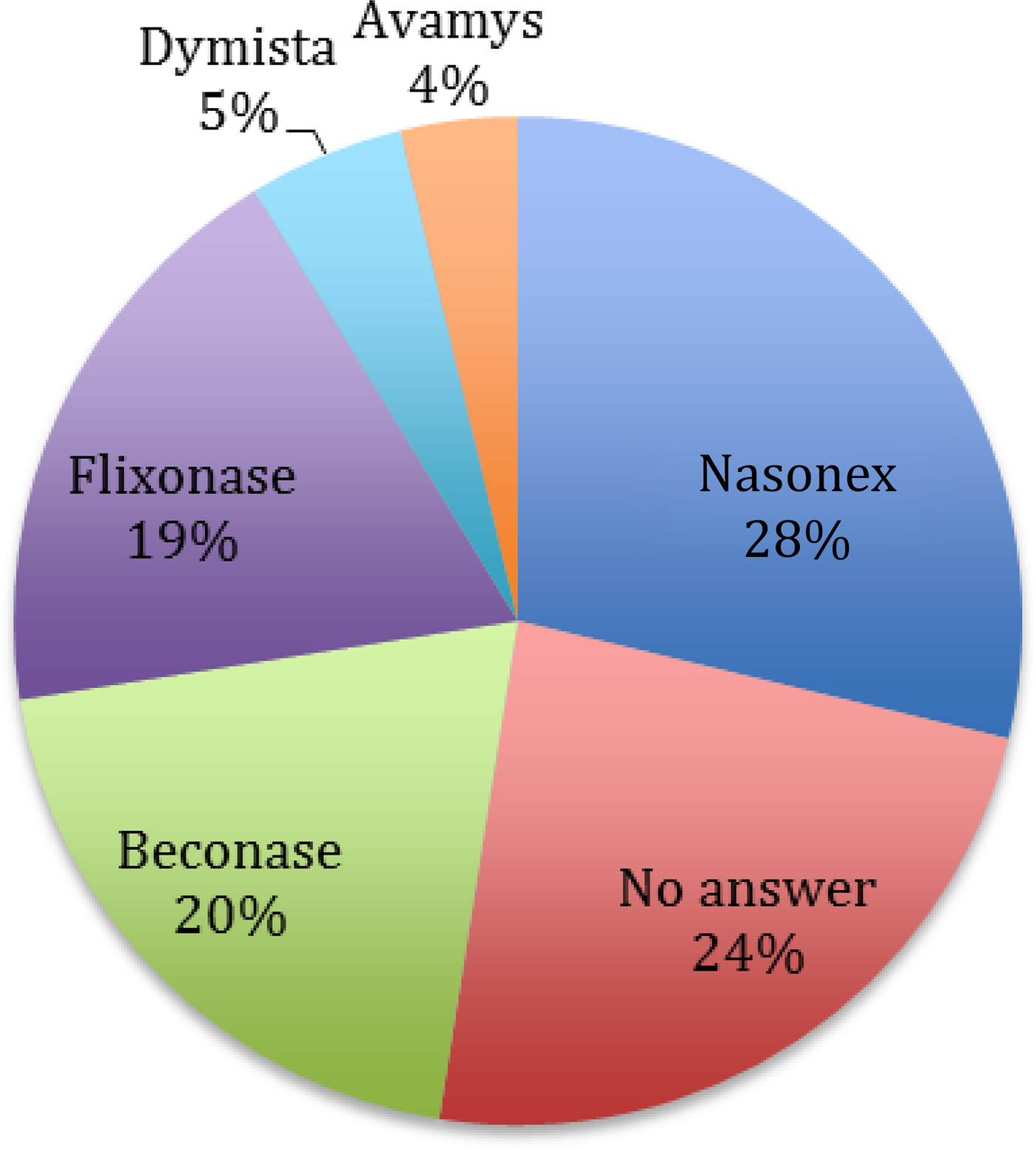
Fig. 6 Intranasal steroid sprays used.
Spray technique
It was revealed that 56 patients (54.4 per cent) used the ipsilateral hand technique, whereas 47 (45.6 per cent) used the contralateral hand technique.
Of the 103 completed questionnaires, 95 patients (92.2 per cent) commented on the head position used for nasal spray application, though 5 of these patients reported using more than 1 head position. This showed that 51 patients (53.7 per cent) used a head up position, 25 (26.3 per cent) used a neutral head position and 23 (24.2 per cent) used a head down position.
Fifty-four patients (53.5 per cent) stated that they had been shown how to use their nasal spray by their general practitioner.
Side effects
Twenty-two patients (21.4 per cent) reported side effects with intranasal steroid spray use. Of these, 10 patients (45.5 per cent) reported nasal irritation, 8 (36.4 per cent) reported epistaxis, and 12 (54.5 per cent) reported both nasal irritation and epistaxis. Fourteen patients (63.3 per cent) graded their epistaxis as minor, with 5 (22.7 per cent) describing it as moderate. No patients described their epistaxis as severe.
Side effects and technique
Of the 20 patients who reported epistaxis (the epistaxis-alone group plus the nasal irritation and epistaxis group), 16 (80 per cent) used the ipsilateral technique and 4 (20 per cent) used the contralateral technique.
Fourteen of the 22 patients (63.6 per cent) who reported nasal irritation used their ipsilateral hand whereas 8 (36.4 per cent) used their contralateral hand (Table I).
Table I Nasal spray technique and side effects

Compliance
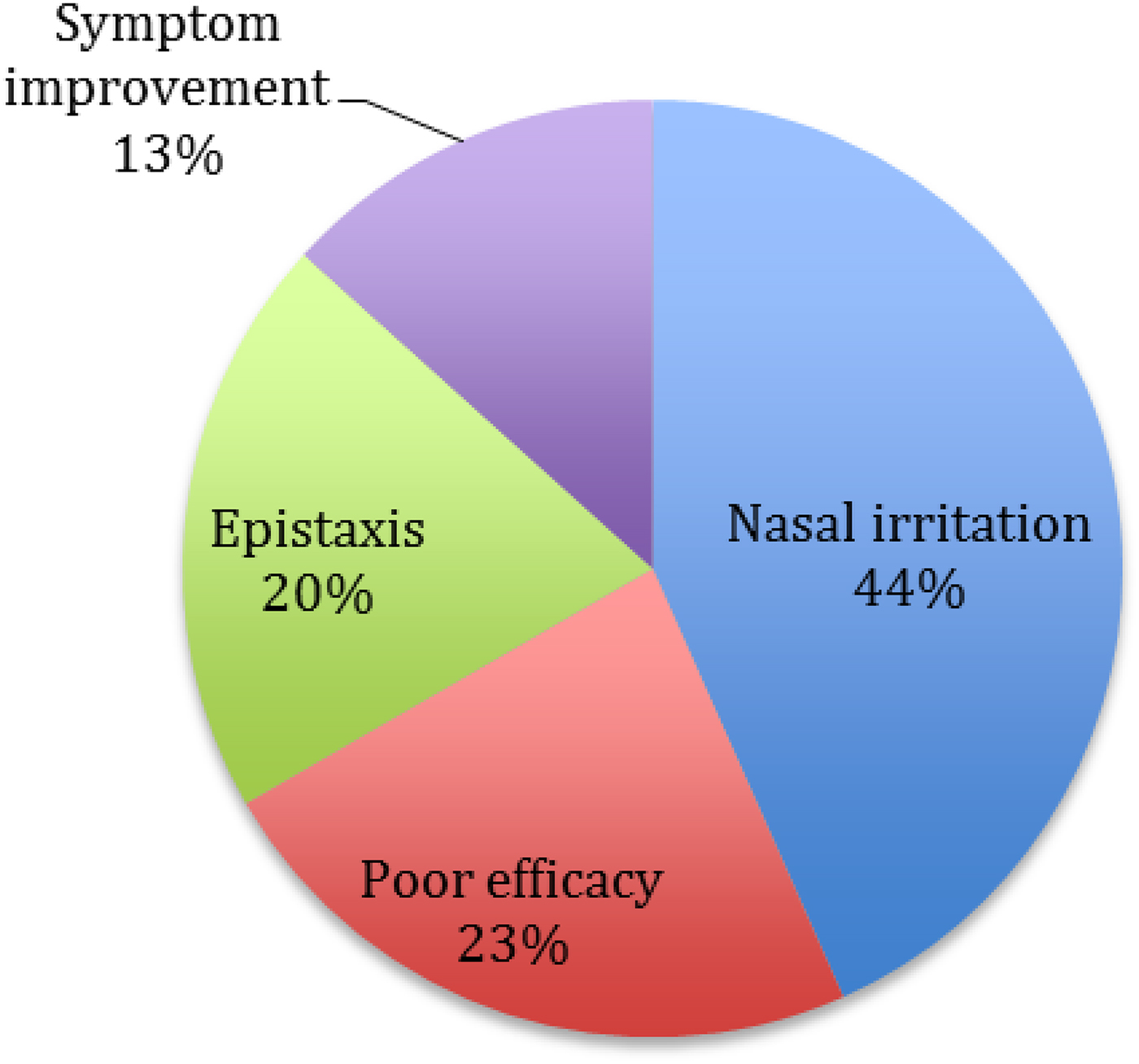
Thirty patients (29.1 per cent) stopped using their intranasal steroid spray. The reasons given for this non-compliance were: problems with nasal irritation (n = 13), lack of symptom improvement (n = 7), epistaxis (n = 6) and symptom resolution (n = 4) (Figure 7).
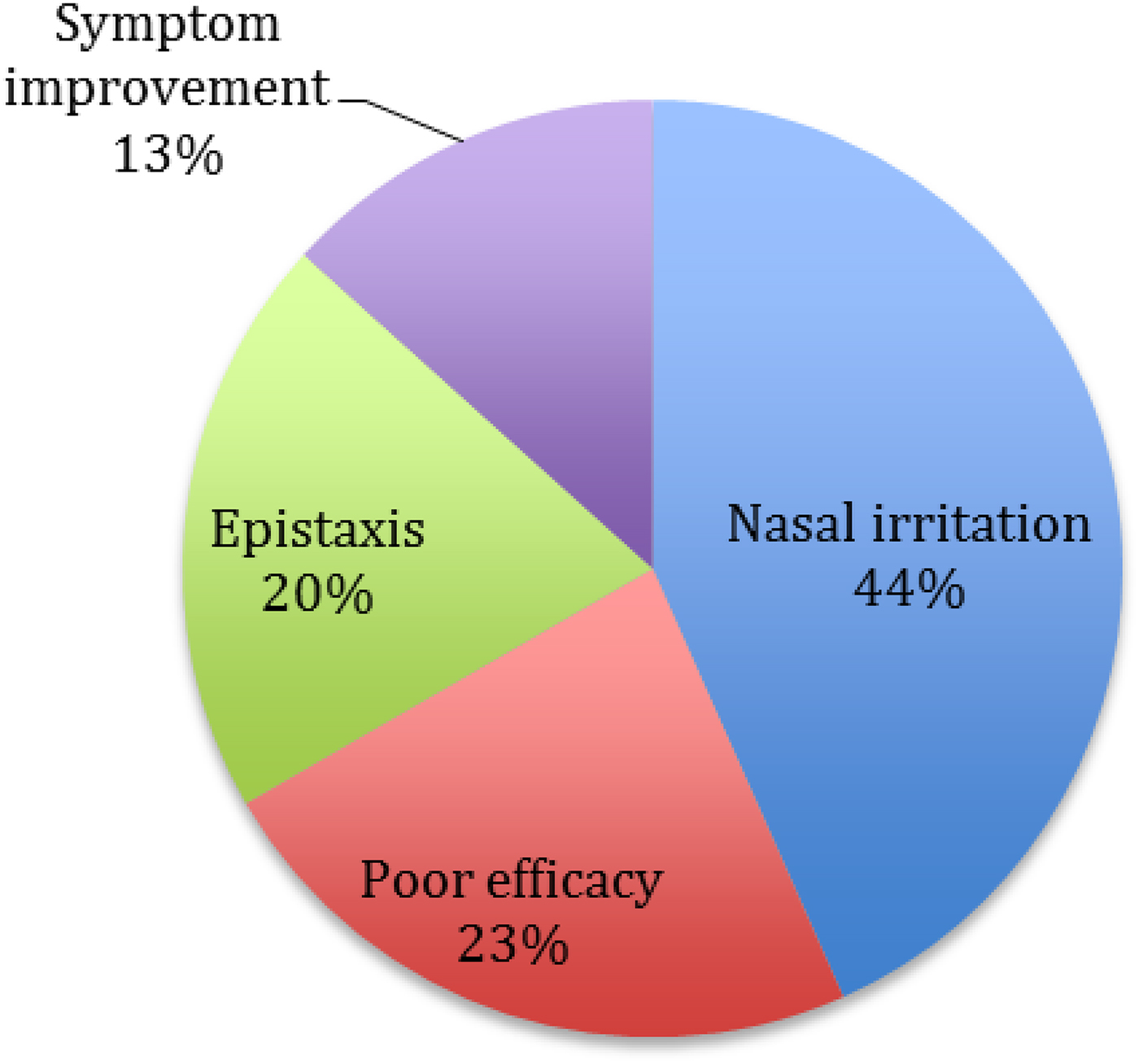
Fig. 7 Reasons for intranasal steroid spray non-compliance.
Therefore, the majority of patients (26 out of 30) who showed poor compliance cited either a lack of symptom improvement or side effects. Of these 26 patients, 20 (77 per cent) used the ipsilateral technique, whereas 6 (23 per cent) used the contralateral technique (p = 0.01, Fisher's exact test two-sided).
Discussion
Our findings show that roughly half of our patients (55.4 per cent) used their ipsilateral hand to apply the nasal spray. The patients who used an ipsilateral spray technique were four times more likely to experience epistaxis and three times more likely to stop using their intranasal steroid spray than patients using a contralateral technique. The ipsilateral spray technique group also experienced a greater proportion of nasal irritation, but this effect did not reach statistical significance (p = 0.35). However, there was statistically significant poorer compliance (p = 0.01) in the ipsilateral group than in the contralateral group, likely due to the excess adverse effects experienced.
The exact cause of nasal irritation and epistaxis with intranasal steroid spray use is unclear. One theory suggests that there is mechanical trauma from use of the spray on the nasal lining. Another theory relates to the chemical trauma caused by corticosteroid use, which is supported by the reduced incidence of epistaxis in patients using the newer aqueous intranasal steroid spray preparations.Reference Benninger 12 An ipsilateral hand technique directs the intranasal steroid spray towards the sensitive and vascular septal mucosa, which is more prone to irritation than the lateral nasal wall, which could explain the amplification of this effect in our patient group.
The majority (53.7 per cent) of the patients surveyed in this study also showed a preference for the head up position when using the intranasal steroid spray. This is one application technique reported in basic science studies to limit the distribution of nasal sprays, with steroids reaching only the inferior portion of the nose before heading into the nasopharynx. If drug delivery to the nasal mucosa is limited in this way, patients will likely experience poorer symptom control.
It is clear from these survey results that poor symptom control and adverse effects are closely associated with patient compliance. Almost a third of the patients we surveyed had stopped using their prescribed intranasal steroid spray by the time they were reviewed in the rhinology clinic, and most listed limited efficacy or side effects as the reason. From the previous description of both the ipsilateral application technique and employment of the head up position, we can see why patients may have experienced these issues and become non-compliant with their intranasal steroid spray.
Compliance has been shown to be poor generally for intranasal steroid spray use, even in very symptomatic patients. In a study by Nabi et al., 57.4 per cent of chronic rhinosinusitis patients were non-compliant with intranasal steroid spray use, despite recent sinus surgery.Reference Nabi, Rotenberg, Vukin, Payton and Bureau 13 This suggests that patients generally would prefer not to use an intranasal steroid spray, and that issues such as lack of efficacy and adverse effects are likely to lead to non-compliance. Symptoms are likely to worsen in non-compliant patients, which may lead to consideration of surgical management options, which could potentially be avoided with improved intranasal steroid spray use.
This evidence, albeit from a small patient group, confirms that the intranasal steroid spray technique does influence side effects and patient compliance. Advising patients to avoid the ipsilateral technique could limit these side effects and subsequently improve compliance. Furthermore, advocating the use of a head neutral or head down position to maximise drug delivery could improve symptom control.
Similar studies regarding inhaler technique in the asthma population have shown significant improvement in symptom control and compliance following patient education.Reference Capanoglu, Dibek Misirlioglu, Toyran, Civelek and Kocabas 14 Interestingly, studies have shown that educating asthma patients on inhaler technique on a face-to-face basis is the most effective option.Reference Bosnic-Anticevich, Sinha, So and Reddel 15 Our study shows that only 53.5 per cent of patients were shown how to use their sprays by the general practitioner, albeit potentially with poor advice given the debate regarding the best application technique to use. Our findings should be used to promote a doctor–patient discussion on intranasal steroid spray technique as part of the medical management of inflammatory nasal conditions, specifically to recommend a contralateral application technique that avoids the head up position.
Limitations
This is a relatively small patient survey; it cannot definitively show the link between intranasal steroid spray application technique and side effects or compliance, especially as we had limited baseline information on these patients. Furthermore, it is difficult to know if patients fully understood what was meant by each application technique, though photographs were provided as an example. Moreover, several patients reported using different head positions when using the intranasal steroid spray, and this evidence carries less weight if patients are using different techniques on different occasions. However, the results appear to support previous literature suggesting that an ipsilateral technique aimed towards the nasal septum will likely produce more adverse effects, and a head up technique may limit intranasal steroid spray delivery and therefore have poor efficacy. This paper provides further evidence for the recommendation of a contralateral technique, with a head neutral position.
Conclusion
The technique used to apply a steroid nasal spray does affect side effects and patient compliance. We suggest that patients who experience problematic side effects and/or poor symptom control avoid an ipsilateral technique. We recommend that further investigation is conducted to identify the optimal position for nasal spray application.
-
• Intranasal steroid sprays are frequently used to manage inflammatory nasal conditions
-
• Spray technique has not been shown to affect drug distribution, but is associated with side effects (e.g. nasal irritation, epistaxis)
-
• Such side effects commonly lead to poor compliance
-
• In this study, an ipsilateral technique was associated with more side effects and worse compliance than other methods
Acknowledgements
The authors would like to thank the Otolaryngology Outpatients nursing staff of the Aberdeen Royal Infirmary who distributed surveys to patients using an intranasal steroid spray. The clinical photographs of nasal technique are demonstrated by author Miss Vaishnevy Ganesh, who kindly agreed to be photographed for this purpose.
Appendix 1. Questionnaire on intranasal steroid spray use
Dear Sir/Madam, September 2015
We would like to know about your experience using your nasal spray with this short questionnaire
Many thanks,
Mr Banigo, Mr Shakeel and Mr Ram
ENT Registrar and Consultant
ENT Department
Aberdeen Royal Infirmary
AB25 2ZN