


Echocardiography is a useful method for the evaluation of the cardiac anatomy and function. In addition, it is practical for diagnosis, monitoring of congenital and acquired cardiac diseases. M-mode echocardiography is a widely used method to measure cardiac chambers and wall thickness.Reference Sahn, DeMaria and Kisslo1 The past 15 to 20 years have introduced important developments in echocardiographic techniques, so that is now possible to obtain more clearly identified M-mode waves. Previously, there were several studies suggesting normative data related to cardiac chambers and wall thickness in children.Reference Pearlman, Triulzi, King, Newell and Weyman2–Reference Kampmann, Wiethoff and Wenzel19 However, most of these studies consisted of small and heterogeneous samples of healthy infants, children, and young adults.Reference Pearlman, Triulzi, King, Newell and Weyman2–Reference Henry, Ware, Gardin, Hepner, McKay and Weiner16 The body weight, body surface area, and gender were found to be significant determinants for cardiac dimensions. However, various studies conducted in infants and children introduced conflicting results in regard to correlation of these determinants. In general, body weight was used to express normal values in newborns, whereas body surface area was chosen for infants and older children.Reference Pearlman, Triulzi, King, Newell and Weyman2–Reference Kampmann, Wiethoff and Wenzel19
In this study, we aimed to measure the right ventricle, left ventricle, interventricular septum, aorta, and left atrium diameters using M-mode echocardiography to determine the normal values of healthy newborns. According to these suggested normative data, it can be determined whether newborns have normal or abnormal echocardiographic measurements.
Materials and methods
From January, 2008 to June, 2008, a total of 250 – 130 female and 120 male – term healthy babies who were born by normal vaginal delivery or caesarean section, and completed the first 24 hours of life, were included in the study. Newborns requiring resuscitation after birth; having genetic or skeletal abnormalities; birth weight under 2000 grams or above 4500 grams; whose mothers have diseases such as diabetes mellitus, systemic lupus erythematosus, and hyperthyroidism were not included in the study. The cardiac examination was performed at delivery and the next day to exclude congenital malformation. The local ethics committee approved the study protocol, and a written informed consent was obtained from the parents of all newborns.
M-mode echocardiographic measurements were recorded by a paediatric cardiologist in accordance with the American Society of Echocardiography recommendations.Reference Sahn, DeMaria and Kisslo1 The newborns were examined without sedation in the supine position with the right shoulder slightly raised, using the Siemens Acuson Cypress Cardiovascular System (Mountain View, California, United States of America) echocardiography device. An appropriate probe (7V3C) was used to define the cardiac measurements. Electrocardiogram was performed simultaneously. We evaluated echocardiographic dimensions using body weight, because body surface area changed minimally in this age group. If the newborns were too restless, they were excluded from the study.
The following echocardiographic imaging results were measured in millimetres: right ventricular anterior wall end-diastolic thickness, right ventricular end-diastolic diameter, interventricular septum end-diastolic thickness, left ventricular end-diastolic diameter, left ventricular posterior wall end-diastolic thickness, interventricular septum end-systolic thickness, left ventricular end-systolic diameter, left ventricular posterior wall end-systolic thickness, aortic root dimension, and left atrium dimension. The percentages of left ventricular ejection fraction and shortening fraction were calculated automatically by the system.Reference Sahn, DeMaria and Kisslo1 Each measurement was repeated three times and then the mean of the measurements was taken (Fig 1).

Figure 1 The M-mode echocardiographic measurements for right ventricle, left ventricle and interventricular septum. IVSd = Interventricular septum end-diastolic thickness, LVDd = Left ventricular end-diastolic diameter, LVDs = Left ventricular end-systolic diameter, LVPWd = Left ventricular posterior wall end-diastolic thickness, RVAWd = Right ventricular anterior wall end-diastolic thickness, RVDd = Right ventricular end-diastolic diameter.
Statistical analyses
Data were described as frequencies, median, and mean with standard deviation, unless otherwise indicated. The normality Kolmogorov–Smirnov test was performed to determine whether or not the continuous variables were normally distributed. Data were analysed using Student's t test, analysis of variance with the Tukey Honestly Significant Differences test, and the Mann–Whitney U test. Differences between groups were assessed using the chi-square analysis for categorical variables. All analyses were performed using the Statistical Package for the Social Sciences program (version 16.0, Chicago, Illinois, United States of America) using default settings. A p-value less than 0.05 was considered significant.
Results
The newborns were divided into five groups according to their body weight. The distribution of the groups is shown in Table 1. The measurements are given as a mean and standard deviation in Table 2. Each calculated value is shown graphically (Figs 2–11). All of these measurements showed statistically significant linear increase values from groups 1 to 5 (p < 0.05). When the measurements were evaluated according to gender, significant differences were not found (p > 0.05). The mean left ventricular ejection fraction was 69.62%, with a standard deviation of 9.8%, and the mean left ventricular shortening fraction was 33.78%, with a standard deviation of 6.94%. These parameters did not change with gender, and there was no significant difference among groups (p > 0.05).
Table 1 The distribution of patients according to the body weight and age of life.

Table 2 Normative M-mode echocardiographic data for newborns according to body weight.
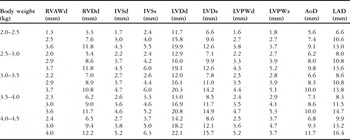
AoD = aortic root dimension; IVSd = interventricular septum end-diastolic thickness; IVSs = Interventricular septum end-systolic thickness; LAD = left atrium dimension; LVDd = left ventricular end-diastolic diameter; LVDs = left ventricular end-systolic diameters; LVPWd = left ventricular posterior wall end-diastolic thickness; LVPWs = left ventricular posterior wall end-systolic thickness; RVAWd = right ventricular anterior wall end-diastolic thickness; RVDd = right ventricular end-diastolic diameter
The mean value is the middle number, the value above −2 SD and the value below +2 SD

Figure 2 Right ventricular anterior wall end-diastolic thickness (RVAWd) according to body weight.

Figure 3 Right ventricular end-diastolic diameter (RVDd) according to body weight.

Figure 4 Interventricular septum end-diastolic thickness (IVSd) according to body weight.

Figure 5 Left ventricular end-diastolic diameter (LVDd) according to body weight.

Figure 6 Left ventricular posterior wall end-diastolic thickness (LVPWd) according to body weight.

Figure 7 Interventricular septum end-systolic thickness (IVSs) according to body weight.

Figure 8 Left ventricular end-systolic diameter (LVDs) according to body weight.

Figure 9 Left ventricular posterior wall end-systolic thickness (LVPWs) according to body weight.

Figure 10 Aortic root dimension (AoD) according to body weight.

Figure 11 Left atrium dimension (LAD) according to body weight.
Discussion
Previously, there were several studies suggesting normative data related to cardiac chambers and wall thickness.Reference Pearlman, Triulzi, King, Newell and Weyman2–Reference Kampmann, Wiethoff and Wenzel19 However, most of these studies consisted of small and heterogeneous samples of healthy infants, children, and young adults.Reference Pearlman, Triulzi, King, Newell and Weyman2–Reference Henry, Ware, Gardin, Hepner, McKay and Weiner16 There are a few number of studies achieving reference values of M-mode echocardiographic measurements for large samples of healthy newborns.Reference Hagan, Deely, Sahn and Frıedman17–Reference Kampmann, Wiethoff and Wenzel19 Of these, two studies were not in accordance with the American Society of Echocardiography recommendations.Reference Hagan, Deely, Sahn and Frıedman17, Reference Solinger, Elbl and Minhas18 In the study conducted by Kampmann et alReference Kampmann, Wiethoff and Wenzel19 and our study, M-mode echocardiographic measurements were recorded in accordance with the American Society of Echocardiography recommendations.Reference Sahn, DeMaria and Kisslo1
This study was conducted in healthy newborns to achieve a normative data for the right ventricle, left ventricle, left atrium, and aortic measurements. A total of 250 newborns had complete cross-sectional M-mode echocardiographic examination. It was shown that all of the measurements were not different with gender; however, the right ventricle, left ventricle, left atrium, and aortic measurements increased linearly in relation to body weight.
Body weight, body surface area, and gender were found to be significant determinants of cardiac dimensions.Reference Kampmann, Wiethoff and Wenzel19 It has been suggested that the variables body weight, body surface area all correlate well with each other.Reference Kampmann, Wiethoff and Wenzel19 However, in newborns, because of the small body surface area, body weight was preferred for measurements.Reference Hagan, Deely, Sahn and Frıedman17–Reference Kampmann, Wiethoff and Wenzel19
M-mode echocardiographic measurements of infants have been proposed to vary according to gender and race.Reference Lester, Sodt, Hutcheon and Arcilla3, Reference Palcoux, Jouan, Palcoux, Lusson, Jallut and Raynaud13, Reference Nagasawa and Arakaki14 Lester et alReference Lester, Sodt, Hutcheon and Arcilla3 performed M-mode echocardiographic measurements in 202 subjects. They have demonstrated the differences in measurements with respect to sex and race. In particular, the differences in measurements have emerged in the adolescent period. In our study, the influence of gender in newborns was not achieved.
In this study, right ventricular anterior wall end-diastolic thickness, right ventricular end-diastolic diameter, interventricular septum end-diastolic thickness, left ventricular end-diastolic diameter, left ventricular posterior wall end-diastolic thickness, interventricular septum end-systolic thickness, left ventricular end-systolic diameter, left ventricular posterior wall end-systolic thickness, aortic root dimension, and left atrium dimension were exponentially correlated to body weight. The right ventricular anterior wall end-diastolic thickness, interventricular septum end-diastolic thickness, interventricular septum end-systolic thickness, left ventricular posterior wall end-diastolic thickness measurements were found to be in agreement with previous studiesReference Hagan, Deely, Sahn and Frıedman17–Reference Kampmann, Wiethoff and Wenzel19 (Table 3). Right ventricular end-diastolic diameter was lower than that in the previous studies,Reference Hagan, Deely, Sahn and Frıedman17, Reference Solinger, Elbl and Minhas18 but similar to the study conducted by Kampmann et al.Reference Kampmann, Wiethoff and Wenzel19 In the study conducted by Kampmann et al,Reference Kampmann, Wiethoff and Wenzel19 right ventricular anterior wall end-diastolic thickness and right ventricular end-diastolic diameter measurements range between 1.3 and 3.7 millimetres, 4 and 13.1 millimetres, respectively. In their study, parallel to ours, the American Society of Echocardiography recommendations were used for the measurements.
Table 3 Normal echocardiographic values in studies that include 200 or more healthy newborns.

AoD = aortic root dimension; IVSd = interventricular septum end-diastolic thickness; IVSs = interventricular septum end-systolic thickness; LAD = left atrium dimension; LVDd = left ventricular end-diastolic diameter; LVDs = left ventricular end-systolic diameters; LVPWd = left ventricular posterior wall end-diastolic thickness; LVPWs = left ventricular posterior wall end-systolic thickness; RVAWd = right ventricular anterior wall end-diastolic thickness; RVDd = right ventricular end-diastolic diameter
The left ventricular end-diastolic diameter, left ventricular end-systolic diameter, and left ventricular posterior wall end-systolic thickness measurements were lower than those of other studies.Reference Hagan, Deely, Sahn and Frıedman17–Reference Kampmann, Wiethoff and Wenzel19 This can be explained with higher temporal and spatial resolutions for echocardiographic scanners, which yield a more exact measurement of cardiac structure. In addition, echocardiographic measurements were recorded by several paediatric cardiologists in other studies.Reference Hagan, Deely, Sahn and Frıedman17–Reference Kampmann, Wiethoff and Wenzel19 In our study, all measurements were recorded by one paediatric cardiologist.
In our study, aortic and left atrial dimensions were found to be ranging from 5.6 to 11.7 and 6.6 to 16.4 millimetres, respectively. These measurements were similar to the study conducted by Kampmann et al,Reference Kampmann, Wiethoff and Wenzel19 but lower than those of previous studies.Reference Hagan, Deely, Sahn and Frıedman17, Reference Solinger, Elbl and Minhas18 In previous studies,Reference Hagan, Deely, Sahn and Frıedman17, Reference Solinger, Elbl and Minhas18 the American Society of Echocardiography recommendations were not used for the measurements.Reference Sahn, DeMaria and Kisslo1 Exterior dimension of the aorta was measured.Reference Solinger, Elbl and Minhas18
In our study, in agreement with previous studies, the ejection and shortening fractions did not change with body weight and gender.Reference Mercier, DiSessa and Jarmakani20–Reference Acar, Maunoury, Antonietti, Bonnet, Sidi and Kachaner24
In conclusion, in this study, normative values related to body weight for right ventricular anterior wall end-diastolic thickness, right ventricular end-diastolic diameter, interventricular septum end-diastolic thickness, left ventricular end-diastolic diameter, left ventricular posterior wall end-diastolic thickness, interventricular septum end-systolic thickness, left ventricular end-systolic diameter, left ventricular posterior wall end-systolic thickness, aorta, and left atrium dimension were determined in term healthy newborns. These reference values can be used to evaluate whether newborns have normal or abnormal echocardiographic measurements.
Acknowledgement
We thank all those pediatric cardiologists working at the Cerrahpaşa Medical Faculty.














