


A female infant with complex cyanotic cardiac disease presented at the age of 45 days with absence of the right atrioventricular connection, the left atrium connecting to a dominant left ventricle, discordant ventriculo-arterial connections, and moderate pulmonary stenosis. As the saturations of oxygen were acceptable, the interatrial communication was sizable, and there was balanced flow of blood to the lungs, surgical intervention at this time was deferred. The family failed to attend follow-up appointments, and the child returned in an extreme state, with chronic liver failure at the age of one year. At presentation, the child was in sinus rhythm, with haemoglobin measured at 11 grams per decilitre. The echocardiogram now showed significant restriction of the atrial shunt from the hugely dilated right atrium (RA) into the left atrium (LA) through a patent oval fossa (Fig. 1 – arrow). The right ventricle (RV) was hypoplastic, with the aorta (Ao) arising anteriorly, and the pulmonary trunk (PT), posteriorly, from the left ventricle (LV). A large, well-organized thrombus (Fig. 2 – arrows) was seen within the right atrial appendage (RAA), which was juxtaposed to the left of the arterial pedicle. Left juxtaposition of the right atrial appendage has been well described in the setting of tricuspid atresia,Reference Thoele, Ursell and Ho1 and may constitute a risk factor for intracardiac thrombosis in this sub-set of patients.
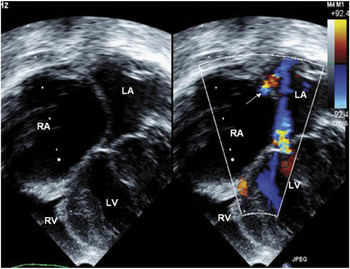
Figure 1 Apical view of echocardiogram.

Figure 2 Parasternal view of echocardiogram.


