


INTRODUCTION
Pituitary metastases are uncommon at presentation in an undiagnosed primary malignancy.Reference Guillén Ponce, Garrido López, Molina Garrido, Muñoz Molina and Carrato1 Patients usually present with headache, visual loss, and changes in the pituitary hormone production. The most common primary malignancies known to metastasise to pituitary gland are breast and small-cell lung cancer.Reference Agha, Brennan, Moore, Grogan and Thompson2–Reference Granata, Figura, Gulisano, Romeo, Sicurezza and Failla4 These lesions mimic pituitary adenoma and present with a similar clinical picture. However, sudden onset of symptoms and rapid progression in patients over 50 years of age with a history of malignancy is more suggestive of metastases. Routine evaluation includes magnetic resonance imaging (MRI) of brainReference Schubiger and Haller5 and biopsy and managed usually with local therapy like surgery or radiotherapy. Addisonian crisis due to pituitary metastases is a rare occurrence based on available literature. We report a case of pituitary metastases presenting with Addisonian crisis in a patient with an undiagnosed lung mass.
CASE PRESENTATION
A 68-year-old white male with a 66 pack year smoking history, prior stroke and swallowing disorder presented to the emergency department with sudden onset of weakness and mild confusion. He was febrile at presentation with a rectal temperature of 39.2 °C. He also complained of a 2-month history of deterioration of vision, unable to see sides while watching the television as well as blurring. Review of other systems was negative. Auscultation of chest revealed rhonchi over right posterior inferior lung fields. Neurological examination revealed intact mental status with right sided hemiparesis and peripheral visual blurring. The chest X-ray showed an infiltrate at the right base. Despite antibiotic treatment, his confusion persisted and computed tomography (CT) of the head demonstrated an old infarct. CT of chest demonstrated a mass measuring 5 cm in the right lower lobe and enlarged right hilar and precarinal nodes. CT of the abdomen did not reveal adrenal lesions. MRI of the brain showed a heterogeneous enhancing pituitary mass extending into the supra-sellar cistern and optic chiasm (shown in Figure 1a,b). Visual filed testing (Goldman perimetry) was consistent with bitemporal superior hemianopia (shown in Figure 2a,b).
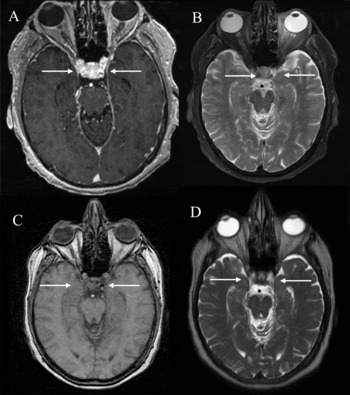
Figure 1. Pre- (a) and post-radiotherapy (c) T1-weighted axial MRI with contrast images showing intra-sellar mass with enlarged pituitary gland, extending to supra-sellar region and resolution of the mass after treatment. Pre- (b) and post-radiotherapy (d) post contrast T2-weighted MRI.

Figure 2. Pre-radiotherapy visual fields: Right eye (a) showing superior temporal defect. Left eye (b) showing midline respecting temporal defect (bitemporal superior hemianopia consistent with compression by the pituitary lesion on optic chiasm). Post-radiotherapy visual fields showing near resolution of field defect superiorly in the right eye (c) and temporally in the left (d) eye.
Adrenocorticotropic hormone (ACTH) stimulation test was suggestive of hypoadrenalism secondary to pituitary abnormality. Laboratory studies showed panhypopituitarism with serum follicle-stimulating hormone: 0.3 mIU/ml (normal: in males, 1.3–19.3), luteinising hormone: 0.3 mIU/ml (1.2–8.6), prolactin: 0.3 ng/ml (2.6–13.1), growth hormone: 0.1 ng/ml (≤10), thyroid-stimulating hormone: <0.10 mIU/l (0.46–4.70), and serum ACTH level of <10 pg/ml (10–60). He was subsequently started on adrenal hormone replacement with hydrocortisone and improved dramatically. On further workup, he was also found to have diabetes insipidus which also responded to adrenal hormone replacement.
Bronchoscopy with needle biopsy demonstrated non-small cell lung cancer. Mediastinoscopy detected evidence of nodal disease (4R lymph node biopsy: two of two positive for metastatic adenocarcinoma). Fluorodeoxyglucose positron emission tomography scan (PET) revealed intense hypermetabolism in the posterior superior segment of right lung, with standard uptake value (SUV) of 8.0 in the precarinal region and 3.8 in the subcarinal region. No other abnormal hypermetabolic foci were seen in abdomen or pelvis. His final diagnosis was metastatic lung cancer (solitary pituitary metastasis) with Addisonian crisis (T2N2M1).
In view of the panhypopituitarism due to pituitary metastases, he was treated with fractionated stereotactic radiotherapy to the sellar lesion. Treatment was planned with a single isocentric technique, using 6 arcs encompassing 480 arc degrees and 20 mm collimator. The ratio of the volume encompassed by the prescription isodose line to the volume of the target volume, prescription isodose to target volume ratio (PITV), was 1.4. A dose of 2375 cGy was delivered in five fractions (475 cGy per fraction) on alternate days (Monday, Wednesday, Friday) over 10 days. The dose was prescribed to the 83% isodose line, with 98.6% of the volume receiving the prescription dose. Mean dose received by the optic chiasm, right optic nerve and left optic nerve was 1192.6 cGy, 206.8 cGy and 346.3 cGy, respectively. Subsequently, he was treated with four cycles of chemotherapy, paclitaxel and carboplatin and concurrent chemoradiation to the right lung mass, 6660 cGy in 37 fractions (180 cGy per fraction, 5 per week over 55 days). Follow-up imaging studies showed resolution of the pituitary mass (shown in Figure 1c,d) and decrease in the lung mass. The endocrine profile was within normal limits. Visual filed testing was normalised (shown in Figure 2c,d) and the patient regained ability to read comfortably. Later, he died of aspiration pneumonia after 11 months.
Discussion
Metastasis to the pituitary gland is rare at initial presentation in patients with malignant disease.1,6 Bitemporal hemianopia is the most common type of visual field defect and the most common endocrine symptom is diabetes insipidus.Reference Granata, Figura, Gulisano, Romeo, Sicurezza and Failla4,Reference Poullin, di Costanzo, Le Pommelet and Gabriel7 Hypothyroidism and hypoadrenalism are also seen in symptomatic hypopituitarism.
A review of the available literature revealed a relative paucity of data with single case studies predominating. Lau et al.Reference Lau, Tan, Chiang and Poh8 reported an unusual case of metastatic carcinoma of the lung in a young Chinese female who presented with pituitary metastasis. She was treated with trans-sphenoidal resection of the lesion. Komninos et al.Reference Komninos, Vlassopoulou, Protopapa, Korfias, Kontogeorgos and Sakas9 reported a rare case of pituitary metastasis in a 68-year-old man with no prior history of malignancy. He was treated with trans-sphenoidal surgical decompression of the sellar mass and pathology was suggestive of a metastatic hepatocellular carcinoma. Later, he was found to have primary liver tumour. Although adjuvant radiotherapy to the sellar mass was recommended, he died due to deterioration of liver disease.
Metastasis to the pituitary in advanced cases of malignancy or on follow-up have been reported. The prognosis is poor due to the poor performance status and presence of other metastases.3,4 Adrenal gland metastases present with symptoms of malaise, weakness and weight loss. Adrenal insufficiency due to adrenal metastasis is a treatable condition and provides a symptom relief after proper management. They are usually diagnosed by CT or PET scans. Hypoptuitarism with adrenal crises due to pituitary metastasis is a rare presentation and management of these patients is primarily treating the pituitary.Reference Piorunek, Nowicka, Mlynarczyk, Nowak, Majewski and Sosnowski10
CONCLUSIONS
In conclusion, we report the case of a patient with panhypopituitarism with Addisonian crisis due to pituitary metastasis at presentation in an undiagnosed lung mass. Immediate radiation therapy to the sellar region with stereotactic radiotherapy along with symptomatic management of the adrenal crisis provided improvement in the symptoms and reversal of the hormonal status. Supplemental hormone therapy is the key to the management of the Addisonian crisis.


