Internationally adopted children often experience a range of early adverse experiences prior to adoption, including deficits in their caregiving environment, such as multiple transitions in care and institutionalization. The lack of a stable caregiver puts these children at risk for long-lasting negative social–emotional outcomes, including difficulties with emotion expression (Ghera et al., Reference Ghera, Marshall, Fox, Zeanah, Nelson, Smyke and Guthrie2009) and social relationships (Almas et al., Reference Almas, Degnan, Radulescu, Nelson, Zeanah and Fox2012; Colvert et al., Reference Colvert, Rutter, Beckett, Castle, Groothues, Hawkins and Sonuga-Barke2008; Erol, Simsek, & Münir, Reference Erol, Simsek and Münir2010; Hodges & Tizard, Reference Hodges and Tizard1989). Therefore, effective interventions to address the social–emotional needs of internationally adopted children are critical.
Although several interventions target children's physical and motor development, there are few evidence-based approaches to prevent or treat internationally adopted children's difficulties with social–emotional functioning (Welsh, Viana, Petrill, & Mathias, Reference Welsh, Viana, Petrill and Mathias2007). The present study sought to examine the efficacy of a home visiting intervention, Attachment and Biobehavioral Catch-up (ABC), in supporting the social–emotional development of internationally adopted children by enhancing parenting quality. The ABC intervention has been found efficacious in improving parental sensitivity in foster parents, Child Protective Services (CPS)-involved parents (Bernard, Simons, & Dozier, Reference Bernard, Simons and Dozier2015; Bick & Dozier, Reference Bick and Dozier2013), and in the current sample of internationally adoptive parents (Yarger, Bernard, Caron, Wallin, & Dozier, Reference Yarger, Bernard, Caron, Wallin and Dozier2019). Given that parental sensitivity is critical to the positive development of social–emotional competence, we predicted that ABC would improve the social competence capabilities of internationally adopted children.
Parenting and Social–Emotional Competence
Social–emotional competence is a multifaceted construct that involves the ability to engage in positive, reciprocal interactions with others, display prosocial behavior, understand emotion expressed by others, and remain emotionally and behaviorally organized in interpersonally challenging situations (Rubin & Rose-Krasnor, Reference Rubin, Rose-Krasnor, Van Hasselt and Hersen1992). Early social–emotional competence plays an important role in future functioning, with higher levels of social–emotional competence linked to later academic success and reduced risk of developing externalizing and internalizing problems (Bornstein, Hahn, & Haynes, Reference Bornstein, Hahn and Haynes2010; Jones, Greenberg, & Crowley, Reference Jones, Greenberg and Crowley2015).
The foundations of social–emotional competence develop within the context of a responsive and sensitive parent–child relationship (Lengua, Honorado, & Bush, Reference Lengua, Honorado and Bush2007). Sensitive and responsive parents are aware of their children's needs, respond promptly and appropriately to their children's signals, and direct positive affect and support toward their children (Laible, Thompson, & Froimson, Reference Laible, Thompson, Froimson, Grusec and Hastings2015). Sensitive parents help to promote children's social–emotional abilities by serving as co-regulators of emotions and behaviors (Eisenberg et al., Reference Eisenberg, Valiente, Morris, Fabes, Cumberland, Reiser and Losoya2003), promoting feelings of social reciprocity and responsibility (Davidov & Grusec, Reference Davidov and Grusec2006), and encouraging positive expectations about relationships (Sroufe, Egeland, & Carlson, Reference Sroufe, Egeland, Carlson, Collins and Laursen1999). Thus, children who experience more sensitive, responsive parenting display more socially competent and prosocial behavior compared with children who experience less sensitive, responsive parenting (Kim, Boldt, & Kochanska, Reference Kim, Boldt and Kochanska2015; Lindsey, Mize, & Pettit, Reference Lindsey, Mize and Pettit1997; Zhou et al., Reference Zhou, Eisenberg, Losoya, Fabes, Reiser, Guthrie and Shepard2002).
Preadoptive Caregiving Experiences
Children adoped internationally experience either institutional or foster care prior to adoption. Children raised in institutional care often do not experience consistent responsive parenting. The quality of institutional care can vary between regions, as institutions in Eastern Europe have typically been associated with particularly high child-to-caregiver ratios and caregiver turnover (Kroupina et al., Reference Kroupina, Toemen, Aidjanov, Georgieff, Hearst, Himes and Sharmanov2014; Robinson, McGuinness, Azuero, & Pallansch, Reference Robinson, McGuinness, Azuero and Pallansch2015). Regardless of region, institutional care is generally associated with high child-to-caregiver ratios, ranging from 8:1 to 31:1 (van IJzendoorn et al., Reference van IJzendoorn, Palacios, Sonuga-Barke, Gunnar, Vorria, McCall and Juffer2011). In addition, specific caregivers are not consistently present for a child due to shift changes, staff turnover, and child movement between wards (van IJzendoorn et al., Reference van IJzendoorn, Palacios, Sonuga-Barke, Gunnar, Vorria, McCall and Juffer2011). Other adults, such as medical workers and volunteers, may also rotate in and out of the children's lives (Johnson, Reference Johnson2000). The high rate of caregiver turnover and high child-to-caregiver ratios make it difficult for children to develop trusting relationships with consistent, responsive caregivers. Furthermore, institutional caregivers tend to focus on the medical and physical well-being of children, and have little training in the importance of social interaction with children (van IJzendoorn et al., Reference van IJzendoorn, Palacios, Sonuga-Barke, Gunnar, Vorria, McCall and Juffer2011). Caregivers in institutions often do not have a psychological investment in the children they care for, viewing the children as a job rather than as their own (Dozier, Kaufman, et al., Reference Dozier, Kaufman, Kobak, O'Connor, Sagi-Schwartz, Scott and Zeneah2014). Therefore, children in institutions often fail to experience interactions with sensitive and responsive caregivers that are important for the development of social–emotional competence.
Internationally adopted children can also be placed into foster care or experience transitions between institutional care and foster care prior to adoption (Grotevant & McDermott, Reference Grotevant and McDermott2014; Rutter, Reference Rutter, Brodzinsky and Palacios2005). Though generally presenting fewer risks than institutional care, children in foster care often experience multiple moves across placements, which can limit exposure to responsive interactions with a primary caregiver (Fisher, Stoolmiller, Mannering, Takahashi, & Chamberlain, Reference Fisher, Stoolmiller, Mannering, Takahashi and Chamberlain2011; Holtan, Handegård, Thørnblad, & Vis, Reference Holtan, Handegård, Thørnblad and Vis2013). As with institutional workers, foster caregivers may lack psychological investment in the children in their care, which is associated with poorer quality of foster parent–child interactions (Bernard & Dozier, Reference Bernard and Dozier2011; Dozier & Lindhiem, Reference Dozier and Lindhiem2006).
Social–Emotional Competence of Children Adopted Internationally
Given these adverse early caregiving experiences, it is not surprising that problems in social–emotional competence are observed in children adopted internationally. For example, one longitudinal study found that internationally adopted children exhibited more social difficulties and fewer close relationships during adolescence than children living with their biological parents (Hodges & Tizard, Reference Hodges and Tizard1989; Tizard & Hodges, Reference Tizard and Hodges1978). Similarly, the Bucharest Early Intervention Project found that 8-year-olds who had experienced institutional care or who were placed into foster care after 20 months old displayed lower levels of teacher-reported social skill competencies than children who had never been institutionalized (Almas et al., Reference Almas, Degnan, Radulescu, Nelson, Zeanah and Fox2012). Other studies have found similar problems with social–emotional competence among internationally adopted children, and have linked these deficits to future impairments in areas such as emotion regulation (Colvert et al., Reference Colvert, Rutter, Beckett, Castle, Groothues, Hawkins and Sonuga-Barke2008; Erol et al., Reference Erol, Simsek and Münir2010). Further, the difficulties with social–emotional competence observed in internationally adopted children tend to be more long-lasting and more impactful compared with deficits in other domains (Almas et al., Reference Almas, Degnan, Radulescu, Nelson, Zeanah and Fox2012; Gunnar & Van Dulmen, Reference Gunnar and Van Dulmen2007; Tieman, van der Ende, & Verhulst, Reference Tieman, van der Ende and Verhulst2006).
Postadoption Recovery in Children Adopted Internationally
Adoption is a powerful intervention for children adopted internationally, with children showing dramatic improvements across a range of domains of functioning postadoption (van IJzendoorn & Juffer, Reference van IJzendoorn and Juffer2006). However, the social–emotional difficulties in children adopted internationally can present unique challenges for adoptive parents (Cyr, Euser, Bakermans-Kranenburg, & van IJzendoorn, Reference Cyr, Euser, Bakermans-Kranenburg and van IJzendoorn2010). Children exposed to early adversity often behave in ways that can make it difficult for parents to provide sensitive and nurturing care (Stovall & Dozier, Reference Stovall and Dozier2000; Stovall-McClough & Dozier, Reference Stovall-McClough and Dozier2004). Specifically, children exposed to early adversity can avoid parents or become angry with parents when they are distressed, which can be interpreted by parents as meaning that their support is not needed or they are not able to effectively care for their children's needs. Children adopted internationally can also display indiscriminately friendly behavior, or overfriendly attention, comfort seeking and affectionate behavior directed toward unfamiliar people (Smyke, Dumitrescu, & Zeanah, Reference Smyke, Dumitrescu and Zeanah2002), which can communicate to parents that they are not uniquely important to the child. Parents tend to respond “in kind” to children's signals, behaving as if their children do not need them (in the case of avoidant behavior or indiscriminately friendly behavior) or responding angrily (in the case of resistant behavior; Stovall & Dozier, Reference Stovall and Dozier2000). Given these unique parenting challenges, parents of children adopted internationally may benefit from interventions designed to help them understand their children's behaviors, enhance specific parenting skills, and override these automatic responses.
Supporting this idea, the parenting quality provided by adoptive parents has been shown to affect children's functioning (Jaffari-Bimmel, Juffer, van IJzendoorn, Bakermans-Kranenburg, & Mooijaart, Reference Jaffari-Bimmel, Juffer, van IJzendoorn, Bakermans-Kranenburg and Mooijaart2006; van den Dries, Juffer, van IJzendoorn, Bakermans-Kranenburg, & Alink, Reference van den Dries, Juffer, van IJzendoorn, Bakermans-Kranenburg and Alink2012). In internationally adopted children followed longitudinally from infancy to age 14, previous and concurrent parental sensitivity predicted child social–emotional development (Jaffari-Bimmel et al., Reference Jaffari-Bimmel, Juffer, van IJzendoorn, Bakermans-Kranenburg and Mooijaart2006). High levels of parental sensitivity are associated with greater child social responsiveness and less indiscriminate friendliness in internationally adopted children (van den Dries et al., Reference van den Dries, Juffer, van IJzendoorn, Bakermans-Kranenburg and Alink2012). Thus, interventions to promote parental sensitivity among adoptive parents may enhance internationally adopted children's social–emotional competence.
Interventions for Internationally Adopted Children
There are few evidence-based interventions available for young internationally adopted children (Ní Chobhthaigh & Duffy, Reference Ní Chobhthaigh and Duffy2018; Welsh et al., Reference Welsh, Viana, Petrill and Mathias2007). The only empirically supported intervention of which we are aware is an attachment-oriented therapy that was studied with Dutch adoptive parents and children placed before 6 months of age (Stams, Juffer, van IJzendoorn, & Hoksbergen, Reference Stams, Juffer, van IJzendoorn and Hoksbergen2001). The intervention involved readings that emphasized the importance of parents being responsive and sensitive to their children's signals and three sessions using video feedback to highlight these parenting behaviors. Increased parental sensitivity was found when children were 18 and 30 months, but only for adoptive families without prior biological children. No intervention effects on social–emotional competence were detected when the children were 7 years old (Stams et al., Reference Stams, Juffer, van IJzendoorn and Hoksbergen2001). Other interventions designed for domestically and internationally adopted children have shown improvements in child attachment and parent–child emotional attachment, and reductions in parent-reported child behavioral problems (Baker, Biringen, Meyer-Parsons, & Schneider, Reference Baker, Biringen, Meyer-Parsons and Schneider2015; Colonnesi et al., Reference Colonnesi, Wissink, Noom, Asscher, Hoeve, Stams and Kellaert-Knol2013). Therefore, interventions that improve social competence, a particular area of concern for children adopted internationally, are still needed.
The ABC Intervention
The purpose of this study was to examine the effects of ABC, an intervention originally developed for young children in foster care, on the social–emotional competence of children adopted internationally. The ABC intervention focuses on enhancing children's social–emotional competence by increasing parents’ sensitive and nurturing behaviors and decreasing parents’ intrusive and frightening behaviors (Dozier, Meade, & Bernard, Reference Dozier, Meade, Bernard, Timmer and Urquiza2014). ABC is a manualized, 10-session intervention implemented in the family's home. The therapist (referred to as a “parent coach”) emphasizes the importance of the intervention targets through discussion of child development research, showing video clips, and making “in-the-moment” comments. These comments help communicate the intervention targets to the parents and encourage parents to implement the behaviors in the intervention sessions.
The efficacy of the ABC intervention has been assessed in randomized clinical trials with both foster and CPS-involved birth parents. These studies found that parents who received the ABC intervention interacted with their children in more sensitive ways than parents in a control intervention (Bernard, Simons, et al., Reference Bernard, Simons and Dozier2015; Bick & Dozier, Reference Bick and Dozier2013). In addition, children randomly assigned to ABC showed lower rates of disorganized attachment (Bernard et al., Reference Bernard, Dozier, Bick, Lewis-Morrarty, Lindhiem and Carlson2012), more normative patterns of cortisol production (Bernard, Dozier, Bick, & Gordon, Reference Bernard, Dozier, Bick and Gordon2015), lower levels of negative affect expression (Lind, Bernard, Ross, & Dozier, Reference Lind, Bernard, Ross and Dozier2014), more advanced receptive vocabularies (Bernard, Lee, & Dozier, Reference Bernard, Lee and Dozier2017; Raby, Freedman, Yarger, Lind, & Dozier, Reference Raby, Freedman, Yarger, Lind and Dozier2019), and more effective executive functioning capabilities (Lind, Raby, Caron, Roben, & Dozier, Reference Lind, Raby, Caron, Roben and Dozier2017) than children in a control intervention.
In the only paper reporting effects of the ABC intervention with internationally adoptive families, parents who received ABC showed improvements in parenting quality, including higher sensitivity, at postintervention compared to parents who received a control intervention (Yarger et al., Reference Yarger, Bernard, Caron, Wallin and Dozier2019). These effects persisted over 2 years of follow-up (Yarger et al., Reference Yarger, Bernard, Caron, Wallin and Dozier2019). These findings indicate that the ABC intervention successfully manipulated parenting quality, which is the hypothesized mechanism by which ABC promotes healthy child development outcomes. A critical next step is to examine ABC's effects on children's outcomes. The present study used data from the same sample as Yarger et al. (Reference Yarger, Bernard, Caron, Wallin and Dozier2019) to assess the efficacy of ABC in improving social–emotional competence among children adopted internationally. We hypothesized that children who received the ABC intervention would display higher social–emotional competence than children who received the control intervention. We also theorized that ABC's effects on social–emotional competence would be mediated by improvements in parental sensitivity.
Method
Participants
Internationally adopted sample
The sample consisted of 131 children adopted internationally. Seven families had 2 children in the study, resulting in a total of 124 parents. Families were recruited through adoption agencies and programs for internationally adopted children at children's hospitals in the Mid-Atlantic region. Fifty-one (38.9%) of the children were adopted from China, 24 (18.3%) from Russia, 23 (17.6%) from South Korea, 15 (11.5%) from Ethiopia, and 18 (13.7%) from other countries. Ninety-eight children (74.8%) were in institutional care for some period prior to adoption and 49 children (37.4%) were in foster care for some period prior to adoption, with 19 children (14.5%) experiencing a combination of institutional and foster care. On average, children spent 13.6 months in institutional care (SD = 7.1) and 12.6 months in foster care (SD = 5.9). At the time of adoption, children were, on average, 16.5 months old (SD = 6.9). On average, children were 20.2 months old when they started the ABC intervention (SD = 6.8). Most children (85%) began the intervention within 6 months of being adopted. Additional demographic information about children and parents can be found in Tables 1 and 2.
Table 1. Child demographic characteristics

Note: ABC, Attachment and Biobehavioral Catch-up. DEF, Developmental Education for Families. DB-DOS, Disruptive Behavior Diagnostic Observation Schedule.
Table 2. Parent demographic characteristics

Note: ABC, Attachment and Biobehavioral Catch-up. DEF, Developmental Education for Families. DB-DOS, Disruptive Behavior Diagnostic Observation Schedule.
Low-risk biological sample
A low-risk sample of 48 nonadopted children being raised by their biological parents was included as a normative comparison group to provide benchmark levels of social–emotional competence. These children were screened for significant risks at the time of enrollment, and had no history of CPS involvement or significant disruptions in caregiving environments. They were recruited from a university-based childcare center and local preschools. Demographic information for these parent–child dyads can be found in Tables 1 and 2. Parents and children in the low-risk biological sample did not receive intervention services.
Procedure
Recruitment for this study began in February 2009, and data were collected through May 2017. Internationally adoptive families were recruited from local children's hospitals and international adoption parent groups in the Mid-Atlantic region of the United States. Children were eligible if they had been adopted from outside of the United States and were 36 months old or younger. After obtaining written consent from parents, a project coordinator randomly assigned participants to the experimental intervention (ABC) or the control intervention (Developmental Education for Families; DEF) using a randomly generated number sequence (with group assignment based on even versus odd digits) and simple randomization. See Figure 1 for the CONSORT diagram. A total of 131 internationally adopted children were enrolled and randomized to receive either the ABC or a control intervention, and participants were unaware of their intervention condition and study hypotheses. The low-risk biological sample was recruited from a university-based childcare center and local preschools and did not receive intervention services. Approval for the conduct of this research was obtained from the University of Delaware Institutional Review Board.

Figure 1. Consolidated Standards of Reporting Trials (CONSORT) flow diagram. ABC, Attachment and Biobehavioral Catch-up. DEF, Developmental Education for Families. BITSEA, Brief Infant–Toddler Social and Emotional Assessment. DB-DOS, Disruptive Behavior Diagnostic Observation Schedule.
Research assessments
After enrollment in the study, families completed a home research visit. For internationally adoptive families, these visits were conducted prior to the first intervention session. On average, children were age 20.0 months old (SD = 6.3) at the time of these visits. Internationally adoptive families completed a postintervention follow-up assessment approximately 1 month after completion of the intervention. On average, internationally adoptive children were 30.1 months old (SD = 5.9) at the time of the postintervention visits. Both internationally adoptive families and low-risk biologically related families completed yearly postintervention research visits around the time of the child's birthday at age 12 months (M = 18.5, SD = 2.8), 24 months (M = 25.5, SD = 2.4), 36 months (M = 37.2, SD = 2.0), 48 months (M = 49.9, SD = 1.9), and 60 months (M = 64.9, SD = 5.8). For internationally adoptive families, these yearly visits were conducted after the completion of the intervention.
Interventions
Internationally adoptive families were randomly assigned to one of two interventions. The control intervention was designed to match ABC in format, frequency, and duration. Both interventions consisted of 10 sessions conducted in families’ homes and were based on structured manuals. Interventionists for each condition were distinct, and both ABC and DEF interventionists received weekly supervision.
Experimental intervention: ABC intervention (Dozier & Bernard, Reference Dozier and Bernard2019)
The ABC intervention helped parents with three primary targets: (a) following the lead of their children, (b) providing nurturing care in response to children's distress, and (c) avoiding intrusive behavior. In the adapted version of ABC for internationally adoptive parents, attention to reducing child indiscriminately sociable behaviors was also added to the basic intervention because of its importance for this population. A key component of the ABC intervention was the parent coaches’ provision of “in-the-moment” feedback about the parents’ interactions with children during sessions (Caron, Bernard, & Dozier, Reference Caron, Bernard and Dozier2018). In addition to these “in-the-moment” comments, parent coaches presented information relevant to intervention targets and provided video feedback to illustrate the target behaviors.
Parent coaches consisted of 10 postbaccalaureate, graduate, and postdoctoral coaches. Coaches received weekly 1.5-hr group supervision from the intervention developer. Training included reviewing the ABC manual and participating in group supervision prior to beginning to implement the intervention.
Control intervention: DEF
The DEF intervention was adapted from a home-visiting program developed by Ramey, Yeates, and Short (Reference Ramey, Yeates and Short1984) that was found to be effective in enhancing children's intellectual functioning when provided intensively and for a long duration. DEF focused on three developmental areas: (a) gross and fine motor skills, (b) language acquisition, and (c) cognitive development.
For the DEF intervention, there were 5 postbaccalaureate, graduate, and postdoctoral parent coaches. Coaches received weekly 1.5-hr group supervision from a postdoctoral researcher. Training included reviewing the DEF manual and participating in group supervision prior to beginning to implement the intervention.
Measures
Outcome: Parent-reported child social–emotional competence
Parents completed the Brief Infant–Toddler Social and Emotional Assessment (BITSEA; Briggs-Gowan & Carter, Reference Briggs-Gowan and Carter2002), a parent-report questionnaire designed to identify children at risk for or currently experiencing behavioral problems and/or delays in social–emotional competence. The BITSEA yields two composite scores: social–emotional competence and behavior problems. The current study utilized only the social–emotional competence scale, as this addressed the domain of interest. The social–emotional competence scale consisted of 11 items that parents rated on a 3-point Likert scale ranging from 0 (not true/rarely) to 2 (very true/often). Items assessed a range of social–emotional competencies, including prosocial interaction (e.g., “Plays well with other children, not including brother/sister”), self-esteem (e.g., “Shows pleasure when s/he succeeds. For example, claps for self”), and imitation/play (“Points to show you something far away”). The social–emotional competence scale was computed by adding item scores, with higher scores indicating higher levels of social–emotional competence. The social–emotional competence scale has good test–retest reliability and acceptable interrater reliability (Briggs-Gowan, Carter, Irwin, Wachtel, & Cicchetti, Reference Briggs-Gowan, Carter, Irwin, Wachtel and Cicchetti2004). In the current sample, this scale had adequate internal consistency (Cronbach's α = .74), which is consistent with studies with other populations (Briggs-Gowan & Carter, Reference Briggs-Gowan and Carter2008; Briggs-Gowan et al., Reference Briggs-Gowan, Carter, Irwin, Wachtel and Cicchetti2004).
The BITSEA was collected at two time points: at the initial, preintervention visits and at the subsequent research visit (the first postintervention for internationally adoptive families). Preintervention scores were available for 153 children (DEF = 53, ABC = 53, biological low-risk comparison = 47). Postintervention scores were available for 137 children (DEF = 43, ABC = 50, biological low-risk comparison = 44).
Outcome: Child observed social–emotional competence
The Disruptive Behavior Diagnostic Observation Schedule (DB-DOS) assessed children's demonstration of social–emotional competence in a laboratory-based protocol (Wakschlag, Briggs-Gowan, et al., Reference Wakschlag, Briggs-Gowan, Hill, Danis, Leventhal, Keenan and Carter2008; Wakschlag, Hill, et al., Reference Wakschlag, Hill, Carter, Danis, Egger, Keenan and Briggs-Gowan2008). The DB-DOS consisted of three different contexts in which children were given varying levels of support: parent, examiner present, and examiner busy. In the parent context, the child interacted with his or her parent in a series of activities, including coloring and cleanup, teaching the child to solve a puzzle, and asking the child to wait independently. In the examiner present context, a trained examiner engaged the child in a standardized protocol, including having the child complete a series of boring tasks (e.g., sorting utensils), play with a toy that was not working, and engage with the examiner in joint play followed by cleanup. In this context, the examiner responded to all of the child's cues and participated in the activities with the child. During the examiner busy context, the examiner provided the child with minimal interaction and support, either pretending to be busy doing work or out of the room. In this context, the child was shown a set of attractive toys and told not to touch them, and asked to put together a difficult puzzle (with a missing piece) to win a prize.
Each context (parent, examiner present, and examiner busy) of the DB-DOS was coded separately, so children received scores for each context. Children's behaviors were evaluated on 4-point scales, ranging from 0 to 3, with higher scores indicating healthier functioning (Wakschlag, Briggs-Gowan, et al., Reference Wakschlag, Briggs-Gowan, Hill, Danis, Leventhal, Keenan and Carter2008; Wakschlag, Hill, et al., Reference Wakschlag, Hill, Carter, Danis, Egger, Keenan and Briggs-Gowan2008). The social–emotional competence scale is a composite of 6 items that assess children's displays of positive affect, social reciprocity, and positive assertions. Independent teams of undergraduate and graduate research assistants were trained to code each of the three DB-DOS contexts. Coding was completed through review of video recordings. Coders were masked to study condition, date of collection, and study hypotheses. Initial reliability was established via 80% exact item-level agreement with master coding sets obtained from the measure developer (Wakschlag, Briggs-Gowan, et al., Reference Wakschlag, Briggs-Gowan, Hill, Danis, Leventhal, Keenan and Carter2008; Wakschlag, Hill, et al., Reference Wakschlag, Hill, Carter, Danis, Egger, Keenan and Briggs-Gowan2008). Twenty percent of the videos were double coded to assess interrater reliability. Interrater reliability was assessed with a one-way random effects intraclass correlation coefficient (ICC; examiner present context: ICC = .88, examiner busy context: ICC = .84, parent context: ICC = .75).
In the current study, DB-DOS data were available for 125 children (DEF = 39, ABC = 53, biological low-risk comparison = 33). One hundred and three children completed the DB-DOS at 48 months, 114 children completed the DB-DOS at 60 months, and 92 children completed the DB-DOS at both ages. Children's social–emotional competence showed significant stability across the two ages (Parent context: r = .22, p < .05; examiner present context: r = .34, p < .01; examiner busy context: r = .37, p < .01). To maximize the sample size and reduce the number of outcome variables, the social–emotional competence ratings for each context were averaged across the two ages.
Mediator: Parent sensitivity postintervention
Parenting behavior was assessed through a semistructured play activity conducted at preintervention and during postintervention follow-up visits when children were approximately 12, 24, and 36 months old. Parents were provided with toys that varied based on the child's age and instructed to play with their child as they normally would for 7 min. Children younger than 18 months at the time of the visits were placed in a high chair and given a set of three toys (i.e., squeaky toy, rattle, and stacking cups). For children between 18 and 35 months, dyads were provided with a set of blocks. For children 36 months and older, dyads were given Play-Doh and related toys (e.g., rollers and cookie cutters).
Video-recorded play interactions were coded using a global 5-point scale of parental sensitivity, which was adapted from the Observational Record of the Caregiving Environment (NICHD Early Child Care Research Network, 1999). The sensitivity scale assessed the extent to which the parent followed the child's lead by responding appropriately to the child's signals. Parents who displayed high levels of sensitivity responded contingently to their child's cues and adjusted their behavior to the interests and pace of the child. Parents who exhibited low levels of sensitivity failed to respond appropriately to the child's bids, frequently directed the interaction, or appeared detached from the child. Coders were masked to study condition, date of collection, and study hypotheses, and were trained to reliability by achieving at least a .75 correlation with a master coder on a reliability set of 10 videos. All videos were double-coded, and the average of both coders’ scores were used for analyses. Interrater reliability was assessed with a one-way random effects intraclass correlation coefficient (ICC = .71).
In the current study, 24 parent–child dyads completed the postintervention play assessment at 12 months old, 91 completed the play assessment at 24 months old, and 97 completed the play assessment at 36 months old. Parent sensitivity showed significant stability across the assessment periods (rs ranging from .26 to .49). To maximize the sample size and reduce the number of variables, the parent sensitivity scores from postintervention assessments at 12, 24, and 36 months old were averaged into a single score.
Statistical analyses
T tests, chi-square tests, and correlations were conducted to check the randomization of groups, examine the effects of possible covariates (e.g., child age and gender) on the target variables, and evaluate possible effects of attrition. Primary analyses used repeated measures analyses of covariance (ANCOVAs) to test for intervention effects on (a) parent-reported child social–emotional competence at 24 to 36 months old, and (b) observed child social–emotional competence at age 48 to 60 months. Differences between parents and children in the ABC and DEF intervention groups were examined using an intent-to-treat approach. ANCOVAs were also used to examine differences on the outcomes between the internationally adopted intervention groups and the low-risk biological comparison group. Cohen's d scores are provided as standardized between-group effect sizes; these scores were calculated using the estimated marginal means (provided in text) from ANCOVA models (i.e., controlling for significant covariates). A mediation model was then tested to assess whether the intervention effects on observed child social–emotional competence were mediated by earlier changes in parent sensitivity. All analyses were conducted in SPSS v. 25, and mediation analyses utilized PROCESS v.3.3 (Hayes, Reference Hayes2016).
Results
Preliminary analyses
Randomization check
Families randomly assigned to the ABC intervention and the DEF intervention were compared across a range of factors to ensure comparability of randomized groups. Children randomly assigned to the ABC intervention did not differ significantly from children assigned to the DEF intervention in child age at intervention, age at the time of the postintervention assessments, gender, race, or ethnicity. Similarly, there were no group differences in parent age, gender, race, ethnicity, education, marital status, or income (all p values > .05). In addition, no significant differences in parenting quality were observed preintervention between parents randomized to receive ABC versus DEF (Yarger et al., Reference Yarger, Bernard, Caron, Wallin and Dozier2019).
There were no significant differences between children adopted internationally and the low-risk biological children with regard to child gender or age at the time of the social–emotional competence assessments, or with regard to parent gender, marital status, or education (all p values > .05). Internationally adoptive parents were older (M = 42.8, SD = 6.1) than low-risk biological parents (M = 36.4, SD = 4.5), t (123) = 5.16, p < .01. In addition, there was a larger proportion of African American parents among the low-risk biological parents than among internationally adoptive parents, χ2 (2) = 8.02, p < .05.
Possible covariates
Associations between children's demographic characteristics, preadoptive experiences, and parent-reported and observed social–emotional competence scores were examined with Pearson correlations. Children's social–emotional competence was not significantly associated with children's age at adoption, gender, or minority status. However, children's age at the time of the DB-DOS assessment was significantly associated with observed social–emotional competence during the examiner present context (r = –.19, p < .05), and was therefore included as a covariate in subsequent analyses involving DB-DOS outcomes. In addition, child gender was significantly associated with parent-reported social–emotional competence on the BITSEA (r = –.21, p < .05), with boys showing significantly lower competence than girls. Child gender was therefore included as a covariate in subsequent analyses that involved BITSEA. A full correlation table of all variables is available in the online-only Supplementary material.
Attrition
To assess whether differential attrition threatened the validity of the social–emotional competence assessments, the characteristics of children who completed the assessments and those who did not were compared. For parent-reported child social–emotional competence on the BITSEA when children were 24 to 36 months old, there were no significant differences between the groups with regard to child or parent age at the preintervention visits, child or parent gender, child or parent race or ethnicity, or parent income, education, or marital status (all p values > .05).
For the assessment of observed child social–emotional competence on the DB-DOS when children were 48 to 60 months old, no significant differences were found between families who participated in the follow-up assessments and those who did not with regard to child or parent gender, age, or ethnicity, and parent income, education, or marital status (all p values > .05). Of note, more families who received ABC participated in the 48 month and 60 month visits than families who received DEF (87% vs. 64%). To explore possible systematic differences between groups beyond demographic characteristics, preintervention parent report of child social–emotional competence on the BITSEA was examined. Results from the preintervention BITSEA, collected prior to being randomized to receive either ABC or DEF, did not differentiate families who completed the 48 or 60 month DB-DOS assessments from those who did not, t (151) = –0.95, p = .34.
Parent gender
The vast majority of the assessments were completed with mothers (n = 164) compared to fathers (n = 8). These fathers were all married, and indicated that they were the primary caregiver for the child. All primary analyses were run with a sample containing only mothers to determine if results changed. All significant results remained (p values < .05) in the sample containing mothers only. In addition, differences between mothers and fathers on the outcomes of interest were explored. There were no significant differences between mothers and fathers with regard to parent-reported child social–emotional competence, observed child social–emotional competence, or parent sensitivity. However, these results should be viewed with caution given the small number of fathers in the current study.
Primary analyses
Parent-reported social–emotional competence
In the repeated ANCOVA analyses, group (ABC, DEF, or low-risk biological comparison) was the between-subject variable, time (pre- vs. postintervention) was the within-subject variable, and parent-reported social–emotional competence was the dependent variable. Child gender was included as a covariate.
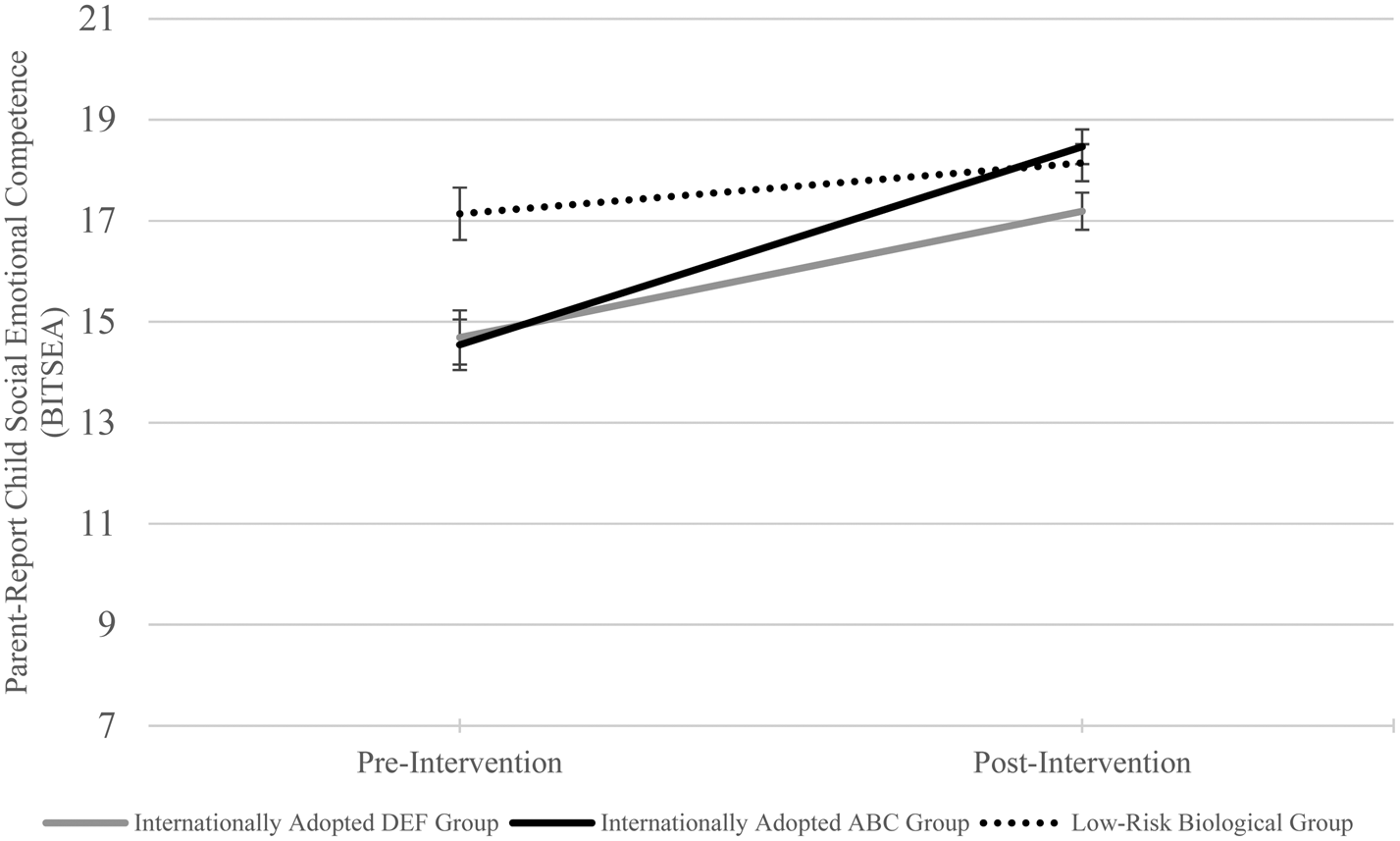
There was a significant interaction between group and time, F (2, 129) = 7.24, Wilks’ λ = 0.90, p < .01. This interaction is depicted in Figure 2. At preintervention, there was not a significant difference in parent-reported social–emotional competence between the ABC group (M = 14.7, SE = 0.5) and the DEF group (M = 14.6, SE = 0.5), F (1, 86) = 0.02, p = .89, d = 0.03. However, the low-risk biological comparison group had significantly higher parent-reported social–emotional competence scores (M = 17.1, SE = 0.5) than the ABC group, F (1, 90) = 13.21, p < .01, d = 0.72, and the DEF group, F (1, 83) = 13.51, p < .01, d = 0.76.

Figure 2. Pre- and postintervention group differences in parent-reported child social–emotional competence (BITSEA). ABC, Attachment and Biobehavioral Catch-up. DEF, Developmental Education for Families. BITSEA, Brief Infant–Toddler Social and Emotional Assessment.
At postintervention, the ABC group (M = 18.5, SE = 0.3) had significantly higher parent-reported social–emotional competence than the DEF group (M = 17.2, SE = 0.4), F (1, 86) = 7.64, p < .01, d = 0.55. The low-risk comparison group (M = 18.1, SE = 0.4) still had significantly higher social–emotional competence than the DEF group, F (1, 83) = 4.16, p < .05, d = 0.41, but did not differ from the ABC group, F (1, 90) = 0.28, p = .60, d = -0.12, at postintervention.
Observed child social–emotional competence
Separate analyses were performed for each of the three DB-DOS contexts: examiner present, examiner busy, and parent. Figure 3 depicts the results.

Figure 3. Postintervention group differences in observed child social–emotional competence (DB-DOS). ABC, Attachment and Biobehavioral Catch-up. DEF, Developmental Education for Families. DB-DOS, Disruptive Behavior Diagnostic Observation Schedule. *p < .05. **p < .01.
DB-DOS examiner present context
Controlling for child age, children adopted internationally whose parents received the ABC intervention exhibited significantly higher levels of social–emotional competence (M = 10.8, SE = 0.4) than children whose parents received the DEF intervention (M = 9.2, SE = 0.5), F (1, 89) = 5.64, p < .05, d = 0.51, in the examiner present context. The low-risk biologically related group (M = 10.2, SE = 0.5) did not significantly differ from the DEF intervention group, F (1, 70) = 1.04, p = .31, d = 0.33, or the ABC intervention group, F (1, 83) = 0.01, p = .98, d = –0.21.
DB-DOS examiner busy context
Children whose parents received the ABC intervention also demonstrated higher social–emotional competence scores (M = 5.6, SE = 0.4) than children whose parents received the DEF intervention in the examiner busy context (M = 4.5, SE = 0.4), F (1, 89) = 4.08, p < .05, d = 0.42. Children in the low-risk biologically related group (M = 5.8, SE = 0.5) scored higher in competence than children in the DEF group, F (1, 70) = 4.20, p < .05, d = 0.45, but did not significantly differ from children in the ABC group, F (1, 84) = 0.21, p = .65, d = 0.07.
DB-DOS parent context
In the parent context, children in the ABC group again scored higher in social–emotional competence (M = 10.2, SE = 0.3) than children in the DEF group (M = 9.3, SE = 0.4), F (1, 89) = 4.87, p < .05, d = 0.44, controlling for child age. Children in the low-risk biological group (M = 10.9, SE = 0.4) scored higher than children in the DEF intervention group, F (1, 70) = 9.03, p < .05, d = 0.74, but did not significantly differ from children in the ABC intervention group, F (1, 83) = 2.44, p = .12, d = 0.22.
Parent sensitivity mediating intervention effects on child social competence
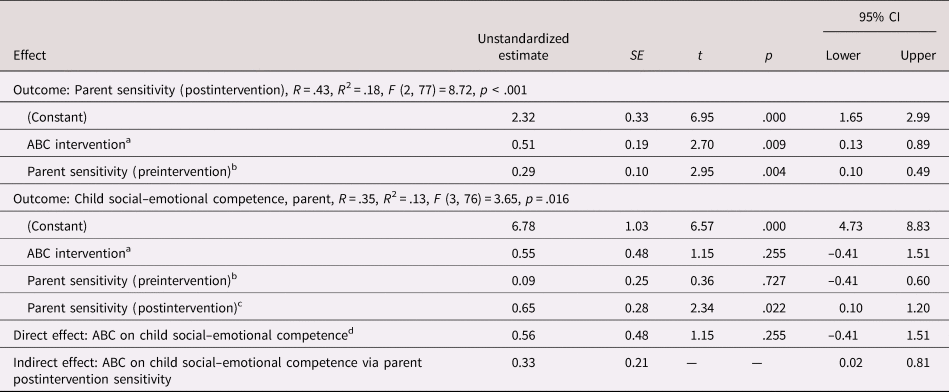
We next examined whether parent sensitivity postintervention mediated the ABC intervention's effects on internationally adoptive children's social–emotional competence outcomes, controlling for parent sensitivity at preintervention. Examination of bivariate correlations revealed that postintervention parent sensitivity was significantly associated with observed social–emotional competence in the parent context (see online-only Supplemental Table S.4). Postintervention parent sensitivity was not associated with parent-reported social–emotional competence or observed social–emotional competence in the examiner present or busy contexts. Therefore, we examined a mediation model with observed social–emotional competence in the parent context as the outcome. PROCESS v.3.3 (Hayes, Reference Hayes2016) was used to test a mediation model, with intervention group as the predictor, observed child social competence with parent when children were between 48 and 60 months old as the outcome, and postintervention parent sensitivity when children were between 12 and 36 months old as the mediator. Parent sensitivity at preintervention was included as a covariate in these mediational analyses. Results indicated that the mediational effect was statistically significant, given that the 95% confidence interval around the unstandardized coefficient of the indirect effect [0.02, 0.81] did not include 0 (see Table 3). In addition, the direct effect of intervention group on observed child social–emotional competence with parent was no longer significant with the mediator included (p = .26). This suggests that postintervention parent sensitivity fully mediated the association between intervention group and observed child social–emotional competence with the parent.
Table 3. Mediation model of ABC intervention predicting observed child social–emotional competence via parent sensitivity

Note: SE, standard error. CI, confidence interval. ABC, Attachment and Biobehavioral Catch-up. DB-DOS, Disruptive Behavior Diagnostic Observation Schedule. aABC intervention was coded as 1 = ABC, 0 = DEF. bParent sensitivity (preintervention) was measured prior to beginning the interventions. cParent sensitivity (postintervention) was measured during the follow-up visits when children were approximately 12, 24, and 36 months old. dObserved child social–emotional competence was measured with the DB-DOS parent context when children were 48 to 60 months old.
Discussion
The results of this study provide strong support for the efficacy of the ABC intervention in improving the development of social–emotional competence among internationally adopted children. Children who received this brief, 10-session intervention were more likely to have higher levels of parent-reported social–emotional competence at 24 to 36 months old and exhibit higher levels of observed social–emotional competence at 48 to 60 months old than children whose parents received the control intervention. Consistent with prior literature showing that internationally adopted children exhibit problems in social–emotional competence (Almas et al., Reference Almas, Degnan, Radulescu, Nelson, Zeanah and Fox2012), internationally adopted children who received the control intervention showed lower social–emotional competence than low-risk comparison children in both parent report and observational contexts. In contrast, internationally adopted children whose parents received ABC were similar to low-risk biological children in both parent-reported and observed social–emotional competence. These results indicate that the brief, preventative ABC intervention can alter the social–emotional developmental trajectories of internationally adopted children so that they are similar to the trajectories of children who have not experienced early adversity. To our knowledge, this is one of the first studies to demonstrate that a parenting-focused intervention can have a positive impact on adopted children's social–emotional competence. In addition, this study builds on prior research by intervening with children adopted much later than in prior work (Juffer, Bakermans-Kranenburg, & van IJzendoorn, Reference Juffer, Bakermans-Kranenburg and van IJzendoorn2005), demonstrating adopted children's plasticity and receptivity to enhanced parenting into toddlerhood.
Previous work demonstrated that ABC improved parent sensitivity in this sample of internationally adoptive families (Yarger et al., Reference Yarger, Bernard, Caron, Wallin and Dozier2019). The current study extended these earlier findings by evaluating whether these changes in parenting behavior were the mechanism by which improvements in internationally adoptive children's development occur. The current study provides some evidence that parent sensitivity postintervention mediated the positive effect of ABC on social–emotional competence, providing evidence for this purported mechanism of change in ABC. Interestingly, parent sensitivity mediated intervention group differences only for children's observed social–emotional competence while they were interacting with their parents. More sensitive parents tended to elicit greater social–emotional competence from their children in a parent-directed laboratory task, whereas associations between parent sensitivity and parent-reported social–emotional competence and social–emotional competence in the contexts administered by an examiner following standardized procedures were smaller and nonsignificant (r = .08–.09).
It is critical to consider other possible mechanisms by which the ABC intervention may have enhanced internationally adoptive children's social–emotional competence. Decreases in dysfunctional parenting behaviors and improvements in the psychological well-being of parents may have buffered children against risks associated with exposure to early adversity (Luthar & Eisenberg, Reference Luthar and Eisenberg2017). ABC has been shown to reduce harsh and intrusive parenting behaviors as well as increase sensitivity (Yarger et al., Reference Yarger, Bernard, Caron, Wallin and Dozier2019), and these changes may help account for the improvements in child social–emotional functioning. In addition, the positive interactions and psychological support provided by the parent coach may have contributed to improvements in parents’ psychological well-being or parenting self-efficacy, which in turn could support the improvements in child social–emotional functioning (Lieberman, Silverman, & Pawl, Reference Lieberman, Silverman, Pawl and Zeanah2005; Luthar & Ciciolla, Reference Luthar and Ciciolla2015; Toth, Gravener-Davis, Guild, & Cicchetti, Reference Toth, Gravener-Davis, Guild and Cicchetti2013).
Strengths, weaknesses, and future directions
The current study has several strengths that enhance the interpretation of the results. Use of both observational and parent-reported assessments of social–emotional competence increases confidence in the results, as findings were replicated across two different methods of assessment. Randomization to the experimental or control intervention allows us to infer a causal relation between the ABC intervention and later improved social–emotional competence. In addition, the inclusion of a low-risk, nonadopted sample provided evidence that ABC improved internationally adopted children's social–emotional competence to a greater extent than DEF, but also that ABC normalized children's social–emotional competence to levels observed in a typical developmental trajectory. Finally, outcomes were assessed across several years of follow-up, and continued until children were 5 years old, allowing us to demonstrate that ABC resulted in relatively long-term improvements in social–emotional competence for children adopted internationally.
The results of this study should be evaluated with regard to its limitations as well. Although there appeared to be no significant differences at preintervention between ABC and DEF groups, and no demographic factors contributing to attrition, the current study did observe significant differences in the number of participants who completed the 48 month and 60 month DB-DOS assessments. Therefore, it is possible that unmeasured factors may have influenced participation in follow-up visits (e.g., satisfaction with intervention, and children with more significant medical or behavioral concerns). Future research should examine other aspects of children's development that may be impacted by ABC; difficulties with inattention, internalizing symptoms, and externalizing behavior are also areas known to be problematic in internationally adopted children (Jufferet al., Reference Juffer, Bakermans-Kranenburg and van IJzendoorn2005; Lindblad, Ringbäck Weitoft, & Hjern, Reference Lindblad, Ringbäck Weitoft and Hjern2010). Future work should also investigate if there are subgroups of adopted children for whom ABC is most effective or needed. In addition, continued work should assess the long-term impact of ABC and improvements in parental sensitivity on children's continued social–emotional development, especially as children enter school and interact more with same-aged peers.
Conclusions
Adoption itself is a profound intervention for children with histories of adversity, with dramatic improvements in a range of developmentally relevant areas observed postadoption (van IJzendoorn & Juffer, Reference van IJzendoorn and Juffer2006). Therefore, it is especially noteworthy that the ABC intervention resulted in improvements in social–emotional competence above and beyond any effects of adoption. Specifically, the parents in the current study exhibited average to above average levels of parenting quality prior to intervention. Most prior work on ABC's positive impacts on children was conducted among parents referred to CPS for concerns of maltreatment, making this study's sample of parents unique. The current results show that improvements in parenting quality in a group of parents that is already providing relatively high-quality care can have meaningful positive impact on high-risk children. Specifically, ABC enhanced the social–emotional competence of children adopted internationally to that of a typical developmental trajectory; changes were observed across multiple methods of assessment, and up to 2 years following the completion of the intervention.
Supplementary material
Supplementary material available online at https://doi.org/10.1017/S0954579420000255
Acknowledgments
We gratefully acknowledge the help of occupational and physical therapists at the Children's Hospital of Philadelphia, who helped to adapt the control intervention to address the specific needs of internationally adopted children. We thank the children and families who participated in the research.
Financial support
The project described was supported by National Institutes of Mental Health Grant R01MH052135 to the senior author (M.D.). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health. Trial Registration: Clinicaltrials.gov; NCT00816621.