Introduction
Nasogastric tube insertion is a common procedure performed daily on hospital wards. It enables access to the stomach and allows drainage of stomach contents, aiding enteral feeding and prevention of aspiration.
Nasogastric tube insertion is normally a ‘blind’ technique. Difficulties can arise due to anatomical variation of the larynx and pharynx, physical obstruction to the tube, or altered physiology of swallowing. A paralysed, intubated patient poses problems due to both anatomical obstruction and lack of patient cooperation (i.e. lack of conscious swallowing). Head and neck malignancy may also skew the anatomy of the larynx, as may treatments such as radiotherapy. Furthermore, kyphosis may affect the success of insertion, due to impaired neck extension.
When nasogastric tube insertion fails, direct visualisation can assist, achieved using a laryngoscope or flexible nasendoscope on the ward or under a general anaesthetic in the operating theatre.Reference Karagama, Lancaster and Karkanevatos1 However, these techniques may prove unsuccessful, as direct vision does not allow for manipulation of the nasogastric tube.
Therefore, we propose a nasogastric tube insertion technique utilising a flexible nasendoscope, which can be employed in a ward setting to safely insert the nasogastric tube when previous attempts have proved difficult or impossible.
Prerequisites
This technique requires: (1) a nasogastric tube; (2) no previous history or evidence of stricture of the cricopharynx or oesophagus; and (3) no history of pharyngeal pouch.
Method
A fine, short length of sodium alginate dressing (Kaltostat; ConvaTec UK, Uxbridge, United Kingdom) is used to tie the nasogastric tube to the flexible nasendoscope, just short of the tip. A further sodium alginate tie may be used to anchor the nasogastric tube to the nasendoscope proximally (Figure 1).

Fig. 1 Nasogastric tube attached to flexible nasendoscope with sodium alginate ties.
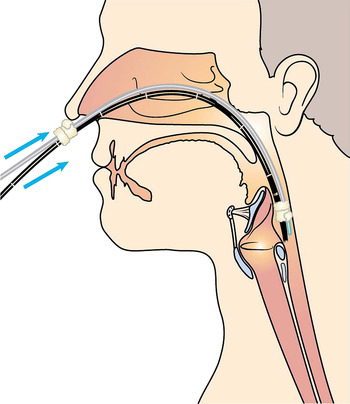
Following nasal application of local anaesthetic, the nasendoscope is passed through the nasal cavity and the nasopharynx. The larynx is viewed directly, and the nasendoscope with nasogastric tube attached is passed into the pyriform fossa and then into the upper oesophagus, with the patient swallowing to facilitate relaxation of the cricopharyngeus (Figure 2). The nasogastric tube is then slowly advanced as the nasendoscope is gently retracted. This gentle tension is sufficient to loosen the sodium alginate ties, thus separating the nasendoscope from the nasogastric tube. The position of the nasogastric tube in the oesophagus is verified under direct vision while retracting the nasendoscope (Figure 3). Once the nasogastric tube is in the oesophagus, it is inserted to the appropriate length and secured.

Fig. 2 Passage of flexible nasendoscope, with attached nasogastric tube, into the oesophagus.

Fig. 3 The flexible nasendoscope is retracted, leaving the nasogastric tube within the oesophagus. The position of the nasogastric tube is verified by the nasendoscope as it is withdrawn.
The position of the nasogastric tube can then be confirmed by a chest X-ray, or by aspiration of gastric contents.
Discussion
This is a quick procedure conducted under direct vision, which can be performed on the ward. It does not require assistance, and inadvertent laryngeal insertion is avoided. Importantly, the method avoids the need for a general anaesthetic.
The method does require the attachment of a sodium alginate dressing tie to the tip of the nasendoscope, and this tie can be expectorated or swallowed. However, ingestion of such a tie poses no potential risks (ConvaTec UK, personal communication) as it is composed essentially of cellulose. A safety study of sodium alginate ingestion showed no adverse effects, other than a bulk laxative effect when taken in high doses over a prolonged period.Reference Anderson, Brydon, Eastwood and Sedgwick2
This method of nasogastric tube insertion requires appropriate preparation of the nose with local anaesthetic, together with appropriate alignment of the nasendoscope with the nasogastric tube.
In addition, a careful, detailed clinical history is required prior to the use of this method, to exclude the possibility of a cricopharyngeal stricture, oesophageal stenosis or pharyngeal pouch. In the presence of such anomalies, the substantial bulk of the nasendoscope nasogastric tube apparatus could result in oesophageal perforation. If there is any doubt, the method should not be attempted, and a general anaesthetic may be required.
At the time of writing, we had successfully used this method four times. No complications had been noted.
Conclusion
We believe that this method provides a quick, simple means of overcoming the difficulties often encountered with nasogastric tube insertion in otolaryngological patients. The method can be performed by any staff member trained in flexible nasendoscope usage (e.g. swallow therapists, endoscopy nurses, Senior House Officer and registrar ENT surgeons).