



Introduction
There is an extensive ongoing debate in the media as well as in the scientific literature on the potential negative effect of contact and collision sport participation on long-term neurocognitive function (Casson & Viano, Reference Casson and Viano2019; Manley et al., Reference Manley, Gardner, Schneider, Guskiewicz, Bailes, Cantu and Iverson2017; Putukian et al., Reference Putukian, Echemendia, Chiampas, Dvorak, Mandelbaum, Lemak and Kirkendall2019). Specifically, it was suggested that the inherent exposure to (repeated) concussions or subconcussive blows may lead to an increased risk or earlier onset of neurodegenerative diseases and psychiatric disorders (Chiò, Benzi, Dossena, Mutani, & Mora, Reference Chiò, Benzi, Dossena, Mutani and Mora2005; Kerr, Marshall, Harding, & Guskiewicz, Reference Kerr, Marshall, Harding and Guskiewicz2012; Lehman, Hein, Baron, & Gersic, Reference Lehman, Hein, Baron and Gersic2012; Mackay et al., Reference Mackay, Russell, Stewart, MacLean, Pell and Stewart2019), declines in neurocognitive performance (Hume et al., Reference Hume, Theadom, Lewis, Quarrie, Brown, Hill and Marshall2017; Pearce, Rist, Fraser, Cohen, & Maller, Reference Pearce, Rist, Fraser, Cohen and Maller2018), and neuroimaging abnormalities (Koerte et al., Reference Koerte, Mayinger, Muehlmann, Kaufmann, Lin, Steffinger and Shenton2016; Strain et al., Reference Strain, Womack, Didehbani, Spence, Conover, Hart and Cullum2015) in retired athletes. While most research on the topic has been conducted with American soccer players (Manley et al., Reference Manley, Gardner, Schneider, Guskiewicz, Bailes, Cantu and Iverson2017), similar findings have also been reported in rugby (Hume et al., Reference Hume, Theadom, Lewis, Quarrie, Brown, Hill and Marshall2017; Pearce et al., Reference Pearce, Rist, Fraser, Cohen and Maller2018), ice hockey (Tremblay et al., Reference Tremblay, De Beaumont, Henry, Boulanger, Evans, Bourgouin and Lassonde2013), and soccer (soccer) (Chiò et al., Reference Chiò, Benzi, Dossena, Mutani and Mora2005; Koerte et al., Reference Koerte, Mayinger, Muehlmann, Kaufmann, Lin, Steffinger and Shenton2016; Mackay et al., Reference Mackay, Russell, Stewart, MacLean, Pell and Stewart2019). However, other studies with retired contact sport athletes report no such effects related to the prevalence of neurodegenerative diseases and psychiatric disorders (Deshpande et al., Reference Deshpande, Hasegawa, Rabinowitz, Whyte, Roan, Tabatabaei and Small2017; McMillan et al., Reference McMillan, McSkimming, Wainman-Lefley, Maclean, Hay, McConnachie and Stewart2017; Vann Jones, Breakey, & Evans, Reference Vann Jones, Breakey and Evans2014), neurocognitive performance (Esopenko et al., Reference Esopenko, Chow, Tartaglia, Bacopulos, Kumar, Binns and Levine2017; McMillan et al., Reference McMillan, McSkimming, Wainman-Lefley, Maclean, Hay, McConnachie and Stewart2017), or neuroimaging abnormalities (Zivadinov et al., Reference Zivadinov, Polak, Schweser, Bergsland, Hagemeier, Dwyer and Willer2018).
The results regarding the long-term effect of repeated subconcussive head impacts (RSHI) as experienced when heading the ball in soccer are similarly inconsistent (Putukian et al., Reference Putukian, Echemendia, Chiampas, Dvorak, Mandelbaum, Lemak and Kirkendall2019). It has been suggested that exposure to RSHI in soccer may lead to neuronal damage comparable to that of repetitive concussions (Maher, Hutchison, Cusimano, Comper, & Schweizer, Reference Maher, Hutchison, Cusimano, Comper and Schweizer2014). Due to the growing public concern, the US Soccer Federation recently banned heading in children under the age of 10 years. The first studies on the topic were conducted in the early 1990s by Tysvaer and Lochen (Reference Tysvaer and Lochen1991), who found mild to severe neuropsychologic deficits in former soccer players compared to a control group, with a higher prevalence of impairment in “typical headers”. However, more recently, two systematic reviews on the topic involving mostly active soccer players found no convincing evidence for this association (Kontos et al., Reference Kontos, Braithwaite, Chrisman, McAllister-Deitrick, Symington, Reeves and Collins2017; Tarnutzer, Straumann, Brugger, & Feddermann-Demont, Reference Tarnutzer, Straumann, Brugger and Feddermann-Demont2017). Interestingly, both meta-analyses noted that studies involving more senior or retired athletes were more likely to report adverse outcomes. Thus, it is possible that some of the inconsistencies in the literature stem from a lack of differentiation between studies involving active versus retired athletes.
Several underlying mechanisms were proposed to explain the link between repeated head impacts and negative long-term outcomes. One compelling hypothesis states that RSHI and concussion may accelerate the otherwise normal cognitive ageing process and thus lead to exacerbated cognitive decline and earlier clinical manifestation of neurodegenerative diseases (Broglio, Eckner, Paulson, & Kutcher, Reference Broglio, Eckner, Paulson and Kutcher2012; Moretti et al., Reference Moretti, Cristofori, Weaver, Chau, Portelli and Grafman2012). In normal brain ageing, peak performance in fluid cognitive abilities is achieved during the third decade of life and declines gradually thereafter (Salthouse, Reference Salthouse2010). Specifically, speed-related domains are characterised by a nearly linear decline, while memory and reasoning show modest declines until 60 years of age and accelerating declines thereafter (Salthouse, Reference Salthouse2019). These cognitive changes are accompanied by structural and functional changes in the brain, including alterations in neuronal structure, loss of synapses, and dysfunction of neuronal networks (Gunning-Dixon, Brickman, Cheng, & Alexopoulos, Reference Gunning-Dixon, Brickman, Cheng and Alexopoulos2009; Morrison & Hof, Reference Morrison and Hof1997). The theory linking (sub)concussive head impacts to accelerated cognitive decline proposes that in individuals with previous head injuries less ageing-related neuronal loss is needed to produce a clinically observable deficit (Figure 1) (Moretti et al., Reference Moretti, Cristofori, Weaver, Chau, Portelli and Grafman2012). Based on the neuropsychological profiles of concussions and cognitive ageing, any adverse effects up to middle age may be most apparent in speed-related domains.

Fig. 1. Hypothetical changes in neural networks in normal ageing and after brain injury. (a) healthy network, (b) healthy network with age-related neuronal loss, (c) network damaged by brain injury, (d) network damaged by brain injury and with age-related neuronal loss. Copyright 2012 by Elsevier. Reprinted with permission from Moretti et al. (Reference Moretti, Cristofori, Weaver, Chau, Portelli and Grafman2012).
To date, only a limited number of studies have assessed whether a differential ageing effect can be observed on neurocognitive or neuroimaging measures in retired contact sport athletes (Esopenko et al., Reference Esopenko, Chow, Tartaglia, Bacopulos, Kumar, Binns and Levine2017; Koerte et al., Reference Koerte, Mayinger, Muehlmann, Kaufmann, Lin, Steffinger and Shenton2016; Tremblay et al., Reference Tremblay, De Beaumont, Henry, Boulanger, Evans, Bourgouin and Lassonde2013). Tremblay et al. (Reference Tremblay, De Beaumont, Henry, Boulanger, Evans, Bourgouin and Lassonde2013) reported an interaction between age and group, when comparing ventricular volume and cortical thickness between concussed and non-concussed ice hockey and American soccer players. A significantly greater decrease in cortical thickness with age was also found in retired soccer players compared to non-contact sport controls (Koerte et al., Reference Koerte, Mayinger, Muehlmann, Kaufmann, Lin, Steffinger and Shenton2016). Further, greater exposure to RSHI was correlated with thinner cortex, and thinner cortex was predictive for lower processing speed in the same sample. However, a recent study by Esopenko et al. (Reference Esopenko, Chow, Tartaglia, Bacopulos, Kumar, Binns and Levine2017) found no differential ageing effect on neurocognitive performance in retired ice hockey players relative to a control group. Thus, while there is some evidence supporting the accelerated decline hypothesis in relation to changes in brain structure, an analogous relationship has not been reported for neurocognitive measures.
These inconsistencies may partly be due to several methodological difficulties including very small sample sizes, ambiguity of concussion definition and diagnosis, and issues with recall bias when assessing concussion history or RSHI exposure retrospectively. In the present study, we will therefore not attempt to quantify these variables, but assess cognitive ageing in a large sample of athletes at high risk for RSHI and concussions relative to a normative sample. We chose to analyse female soccer players as soccer players have an inherently high exposure to RSHI (heading) and concussions, and previous literature has almost exclusively focused on male athletes. This is an important gap in the literature as female soccer players have a higher incidence of concussions compared to male soccer players (Prien, Grafe, Rossler, Junge, & Verhagen, Reference Prien, Grafe, Rossler, Junge and Verhagen2018) and, additionally, may be particularly vulnerable to the (long-term) effects of repetitive head impacts (Covassin, Savage, Bretzin, & Fox, Reference Covassin, Savage, Bretzin and Fox2018; Esopenko, Simonds, & Anderson, Reference Esopenko, Simonds and Anderson2018).
The aim of the present study was consequently to investigate whether there is an interaction between age and soccer exposure in their effects on neurocognitive performance. In other words, is playing elite soccer associated with exacerbated cognitive ageing?
Method
This cross-sectional study was conducted as part of two multicentre projects on concussion in soccer. The inclusion criteria for the present analyses were female sex, 15 to 49 years of age, and (previous) participation in elite soccer. Elite soccer was defined as playing in the first league and/or for the national team of Switzerland, Germany, or The Netherlands. Data from active elite female soccer players aged 15–29 years were collected in Switzerland; players were contacted through their soccer clubs and all clubs of the first Swiss league took part in the study. Data from retired elite female soccer players aged 30–49 years were collected in Germany and The Netherlands; contact details of eligible retired players were compiled through records available online and with the help of two well-connected retired female soccer players who acted as study ambassadors. All players who gave written informed consent to participate in the study underwent an initial screening. In participants under 18 years of age, informed consent was obtained from the parents. No player was suffering from a current head injury or symptomatic neurologic/psychiatric disorder; however, individual test results (n = 9, .54%) were excluded if at least two of the following three indicators deemed the score invalid: (a) the manufacturers validity indicator (Boyd, Reference Boyd2015), (b) the test administrator at time of testing, (c) scores were outliers (Xi > Q3 or <Q1 ± 1.5*IQR). Ethical approval was given by the ethical review boards of Münster, Germany (2016-449-f-S), Kanton Zurich, Switzerland (2017-01921), and the VU University Medical Center Amsterdam, The Netherlands (2017.360).
Relevant demographic and player characteristics were assessed via an online questionnaire and included age, native language, handedness, education, playing position, and concussion history. Concussion was defined as a direct blow to the head, face, neck, or elsewhere on the body with an impulsive force transmitted to the head resulting in specific clinical symptoms that may or may not include loss of consciousness as described by the Concussion in Sports Group (McCrory et al., Reference McCrory, Meeuwisse, Dvorak, Aubry, Bailes, Broglio and Vos2017). Neurocognitive performance was evaluated in the players native language (92.5%) or language of their country of residency (7.5%) using the computerised neuropsychological test battery CNS Vital Signs (CNSVS). This test battery was chosen, as it is one of the core computerised neurocognitive test batteries recommended for the assessment of sport-related concussion (Broglio et al., Reference Broglio, Kontos, Levin, Schneider, Wilde, Cantu and Joseph2018), and well established for the measurement of subtle cognitive deficits (de Oliveira & Brucki, Reference de Oliveira and Brucki2014). There is evidence that CNSVS is sensitive to age-related differences over the lifespan (Gualtieri & Johnson, Reference Gualtieri and Johnson2006), able to identify malingerers (Gualtieri & Hervey, Reference Gualtieri and Hervey2015), and to discriminate between healthy subjects and patients with various psychological or neurological disorders (Gualtieri & Johnson, Reference Gualtieri and Johnson2008; Gualtieri, Johnson, & Benedict, Reference Gualtieri, Johnson and Benedict2006; Iverson, Brooks, Langenecker, & Young, Reference Iverson, Brooks, Langenecker and Young2011; Meskal, Gehring, van der Linden, Rutten, & Sitskoorn, Reference Meskal, Gehring, van der Linden, Rutten and Sitskoorn2015).
The core test battery is comprised of seven well-established neuropsychological tests, which generate 10 domain scores and 1 composite score (memory; combining visual and verbal memory capacities). Five domain scores and the composite memory score were included in the analysis (Table 1). Excluded domain scores were either considered redundant or were lacking variability (i.e., 96.3% of participants scored ≥38 of 40 points on the continuous performance test). Normative data for the test battery were published by Gualtieri and Johnson (Reference Gualtieri and Johnson2006) and are based on a sample of healthy male and female US American participants without previous head injury or past neurological disorders.
Table 1. Description and calculation of domain scores for CNS Vital Signs

Note: CPT, Continuous Performance Test; FTT, Finger Tapping Test; SAT, Shifting Attention Test; SDC, Symbol Digit Coding Test; ST, Stroop Test; VBM, Verbal Memory Test; VIM, Visual Memory Test.
To assess whether there is an interaction between cognitive ageing and playing soccer, the soccer player sample was split into four age groups (15–19, 20–29, 30–39 and 40–49 years), analogous to the classification of the US norm sample (n = 585). All participants in the younger two age groups were still active soccer players, while the older two age groups consisted of retired players. As we did not have access to the original data set of the norm sample, data were simulated based on the published means, SDs, and sample sizes per age group. After visual inspection of the domain score distributions in our sample, normal distributions were simulated for all but one domain. Scores for complex attention were simulated assuming a log-normal distribution. All raw domain scores were subsequently standardised and inverted where necessary, resulting in a uniform scale for all domains with a mean of 100, an SD of 15, and higher scores reflecting better performance.
All data were processed with SPSS (V.25, IBM) and R (V.3.5.3). Descriptive statistics are presented as means with SDs and frequencies with percentage. Mean differences in neurocognitive performance between soccer players and the norm sample by age group were reported with 95% bias corrected and accelerated confidence intervals (CIs) based on 1000 bootstrap samples. To investigate the interaction between cognitive ageing and playing soccer, we used a two-way factorial ANOVA based on 20% trimmed means, due to violation of assumptions related to normality and/or homoscedasticity (Wilcox, Reference Wilcox2016). Variables entered into the model were age groups (four groups: 15–19, 20–29, 30–39, 40–49 years), study population (two groups: norm sample vs. soccer players), and interaction terms. As further information on the norm sample was not available, we were not able to adjust the model for potential confounders such as education, sex, or language. Bonferroni correction was used to control the false discovery rate at α = .05 (p < .0083). Significant interaction effects were followed up with simple effects analysis.
Results
Participant Demographics
A total of 240 female soccer players aged 15–49 years took part in the study; 174 active Swiss players, 51 retired German players, and 15 retired Dutch players. Sample size and player characteristics by age group are shown in Tables 2a and 2b. Handedness, native language, and playing position were similar across age groups; the majority of players reported German (77.5%) as their native language, right handedness (91.8%), and midfield (36.7%) or defence (35.4%) as their main playing position. Further, 10% of active (aged 15–29 years) and 3% of retired players (aged 30–49 years) reported a concussion in the last year. Around half of retired players (n = 32) had at least one concussion during their lifetime. Differences across age groups were noted in sex distribution of the norm sample and match exposure of soccer players. There were fewer females in the youngest norm sample group, and soccer players aged 40–49 years had the highest match exposure. Additionally, educational attainment varied as a function of age across groups. Overall, the sample was well educated; the vast majority of players aged 20–49 years had obtained a higher secondary degree (58.9%) or above (39.7%).
Table 2a. Characteristics of elite female soccer players and the norm sample by age group

Note: SD, standard deviation.
Table 2b. Characteristics of elite female soccer players by age group
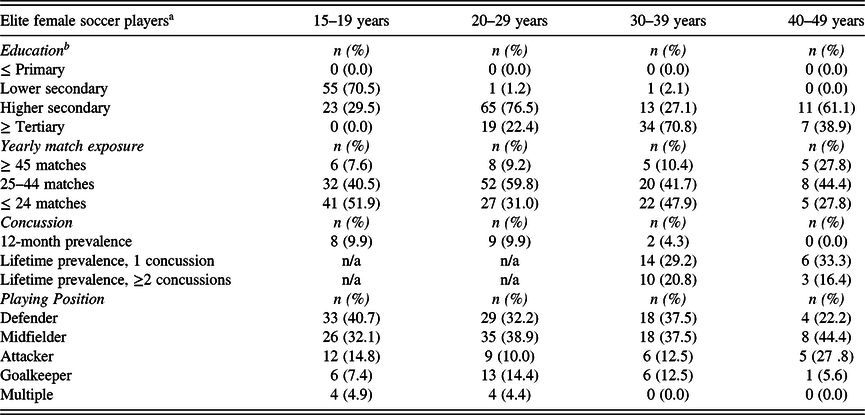
Note: afurther information on norm sample not available; bdefintion according to the International Standard Classification of Education (ISCED, 2011 – UNESCO Institute for Statistics, 2012).
Cognitive ageing in female soccer players compared to the norm sample
In the norm sample, cognitive performance generally peaked during the third decade of life and declined thereafter with the exception of complex attention, which showed declines only after the fourth decade of life (Figure 2, supplementary Table S1). Similar, albeit less consistent age trends were observable in the female soccer player sample (Figure 2, supplementary table S1). Soccer players scored higher than the norm sample in all domains and across all age groups with the exception of reaction time (Figure 2, Table 3). The largest mean differences between study populations across age groups were observed in the psychomotor speed domain, with values ranging from 9.80 (95% CI = 4.09, 15.50) in the oldest age group to 16.54 (95% CI = 11.61, 21.47) in the youngest age group (Table 3).

Fig. 2. Neurocognitive performance in elite soccer players and the norm sample; note that lines are a visual aid and do not represent data points; *significant interaction effect.
Table 3. Mean differences in neurocognitive performance between soccer players and the norm sample by age group and interaction effects

Note: MD, mean difference; CI, confidence interval; areference group: norm sample; bbias corrected and accelerated based on 1000 bootstrap samples;*p < .0083.
There were no significant interactions between age group and study population in their effects on test performance in the domains memory, psychomotor speed, reaction time, complex attention, and cognitive flexibility (Table 3). However, a significant interaction was found on tests of processing speed (F = 16.89, p = .002). Simple effects analysis revealed that processing speed scores of soccer players were significantly better than those of the norm sample in the younger two age groups, 15–19 years (F = 30.06, p < .001) and 20–29 years (F = 33.25, p < .001), but not in the older two age groups, 30–39 years (F = 2.69, p = .102) and 40–49 years (F = 1.43, p = .232).
Discussion
The aim of the present study was to investigate whether there is an association between playing elite soccer and exacerbated cognitive ageing. This was studied by investigating the interaction between age group and study population (elite soccer players vs. general population) in their effects on neurocognitive performance. We found that cognitive ageing effects were similar in elite soccer players and controls in all but one domain. This is in line with several studies suggesting that participation in elite-level contact sports may not lead to later-life cognitive dysfunction (Deshpande et al., Reference Deshpande, Hasegawa, Rabinowitz, Whyte, Roan, Tabatabaei and Small2017; Willer et al., Reference Willer, Tiso, Haider, Hinds, Baker, Miecznikowski and Leddy2018). Significant interactions were only observed in the domain processing speed, where soccer players outperformed the norm in the younger two age groups, but not in the older two age groups. As processing speed is highly sensitive to both the effects of cognitive ageing and brain injury (Salthouse, Reference Salthouse2010; Tarnutzer et al., Reference Tarnutzer, Straumann, Brugger and Feddermann-Demont2017), this finding does fit the initial hypothesis well. However, as this effect could only be observed in one out of six domains, we gather that our data do not support the exacerbated decline hypothesis at this point.
It should be noted, however, that given the limitations of this study drawing any firm conclusions would be premature. Particularly, the chosen age range prevents inferences about age trends in soccer players beyond middle age. While age-related cognitive decline of fluid abilities is generally evident from early adulthood onwards, there is great interindividual variability regarding the onset and rate of decline (Moretti et al., Reference Moretti, Cristofori, Weaver, Chau, Portelli and Grafman2012). In the norm sample, age trends were very consistent and in line with the findings from large-scale studies (Salthouse, Reference Salthouse2010), while less consistent age effects were observed in the soccer player sample. It may be that in elite soccer, age-related cognitive decline, and thus, the proposed exacerbation due to RSHI or concussion, only becomes apparent later in life; especially, considering that lifestyle factors such as regular physical activity are believed to positively correlate with cognitive reserve. The cognitive reserve theory maintains that individuals with high cognitive reserve have more robust neuronal networks. Due to either compensatory or neuroprotective mechanisms, this may delay age-related cognitive decline and mitigate the impact of brain damage/pathology on clinical outcomes (Stern, Reference Stern2009). Hence, the suspected cumulative effect of previous head impacts and age-related cognitive decline may have been compensated by cognitive reserve in players up to middle age.
Another noteworthy result of this study is the effect of study population on neurocognitive performance. The youngest age group of elite female soccer players performed better in all test domains when compared to age-matched controls. The greatest mean differences in this age group were found in domains related to processing speed and motor speed tasks. This is in line with the literature, suggesting sport-context-specific (Mann, Williams, Ward, & Janelle, Reference Mann, Williams, Ward and Janelle2007), and general cognitive enhancements through sports. In soccer and other strategic sports, a positive relationship between abilities underlying higher executive functioning and on pitch performance has been reported by several recent studies (Huijgen et al., Reference Huijgen, Leemhuis, Kok, Verburgh, Oosterlaan, Elferink-Gemser and Visscher2015). The superior performance of young elite soccer players may be explained through the rich and cognitively stimulating environment of elite sports in combination with the positive effects of physical activity (Voss, Kramer, Basak, Prakash, & Roberts, Reference Voss, Kramer, Basak, Prakash and Roberts2010). In light of the focus on adverse outcomes, it is important to note that contact sport also seems to have inherent beneficial effects on cognitive performance. Of course, self-selection effects cannot be ruled out, as players with better executive functioning may have a higher likelihood to be selected for an elite-level team.
The trend of soccer players outperforming the norm sample is maintained across all age groups and domains with the exception of reaction time. Reaction time was the only domain, in which soccer players performed worse than the norm sample (age groups 20–29 and 30–39 years). However, it is unlikely that this is an effect of exposure to RSHI or concussion, as similar results were reported by Hume et al. (Reference Hume, Theadom, Lewis, Quarrie, Brown, Hill and Marshall2017), who found retired rugby players with and without previous concussions as well as non-contact sport athletes to have significantly worse reaction time scores compared to the US norm. This is surprising since rapid information processing and inhibitory control are skills frequently required and trained in the team sport environment.
Our study has several limitations. First, only very limited information was available on the norm sample, and therefore, we cannot rule out that the norm sample included participants that have been exposed to RSHI during their lives. Additionally, we were not able to adequately match the study groups on relevant socio-demographic factors such as sex, education, and native language. However, since age trends in cognitive performance were our primary interest, socio-demographic differences between age groups, not study groups, are the main concern. Language, sex, and several other relevant variables were assessed and found to be similarly distributed across age groups. Thus, while the lack of adequate matching is a significant concern for the interpretation of main effects, we do not expect language or sex to have a differential effect on cognitive ageing in our relatively young sample. This notion is corroborated by a previous study with male and female soccer players aged 15–30 years; when stratifying the sample by sex, age effects were found to persist (Prien, Junge, Brugger, Straumann, & Feddermann-Demont, Reference Prien, Junge, Brugger, Straumann and Feddermann-Demont2019). However, no information on educational attainment was available for the norm sample, and therefore, education-related cohort biases cannot be ruled out. It is also noteworthy that fewer soccer players aged 40–49 years had a tertiary degree than players aged 30–39 years. Another source of potential cohort bias is the overlap of age groups with player status (active/retired) and country of residency; while all active players (aged 19–29 years) were from Switzerland, all retired players (aged 30–49 years) were from Germany or The Netherlands. Further, it could be argued that any interaction effects may only be apparent in previously concussed soccer players and are masked by the majority of non-concussed athletes included in the study. However, this is unlikely as lifetime concussion prevalence in the two older age groups was high (50%) and 10% of soccer players in the younger age groups reported a concussion in the previous year alone. Finally, recruitment for the eldest age group fell short, and thus, results for this age group must be interpreted more carefully.
The findings of the present study hold key information for meaningful future research on the topic of cognitive ageing in contact sport athletes. First, cross-sectional studies investigating the potential long-term effect of RSHI or concussion on cognitive performance in contact sport athletes should focus on age groups older than 50 years, as clinically observable differences seem unlikely in younger age groups. Second, as elite athletes generally perform better on neurocognitive tests than the normal population, it is important to choose an adequate control group (e.g., elite athletes from non-contact sports). Third, when conducting research on neurocognitive performance across the lifespan, it would be desirable to control for variables related to cognitive reserve. Recommended proxies for cognitive reserve in elite athletes are (childhood) IQ, literacy, or composite measures (Stern, Reference Stern2012). While educational attainment is one of the most commonly used proxies, it is not a valid measure when investigating groups under 25 years of age.
Conclusion
While there was a clear trend in the effect of study population on neurocognitive performance, ageing effects were similar in soccer players and controls. Female soccer players generally performed better on tests of cognitive function compared to the norm; however, evidence did not support an overall exacerbated cognitive ageing process. This is the first study using a lifespan approach to research neurocognitive performance in contact sport athletes, and we believe that this approach may hold promise for insightful research in the future.
Acknowledgements
The authors thank the players for participation in the study. We highly appreciate the cooperation of team physicians and coaches of the first league Swiss soccer clubs and U21 teams. We especially thank Birgit Prinz and Leonne Stentler for their invaluable help with the recruitment of retired German and Dutch soccer players. The authors further thank Karin Mani, Alexander Grafe, and Victoria Sump for coordination and administration of the neurocognitive testing. We thank Dzmitriy Katsiuba for digitalisation of the data and Jos Twisk for his assistance with data analysis. The authors gratefully acknowledge FIFA for the support and funding of this study.
Conflicts of Interest
The authors declare that there are no conflicts of interest to disclose.
Funding Information
The study was funded by the Fédération Internationale de Football Association (FIFA).
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1355617720000119.








